

Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a minimally invasive bronchoscopic technique included in the initial diagnostic workup of mediastinal and hilar lymphadenopathy and masses of unknown etiology.1,2
The value of EBUS-TBNA in the diagnosis of lymphoproliferative disorders (LPD) is not well established.1–8 LPD diagnosis requires lymph node sampling for pathologic and flow cytometry analysis. Are the samples obtained by EBUS-TBNA good enough to provide the diagnosis of LPD?
The usefulness of EBUS-TBNA in the diagnosis of LPD in patients with lymph nodes or mediastinal masses and clinical suspicion of LPD was evaluated.
One hundred and eighty nine patients underwent EBUS-TBNA to investigate the etiology of MLN between 2009 and 2012. The suspicion of LPD was based on past history of lymphoma or clinical manifestations and associated with unexplained lymph nodes. EBUS-TBNA biopsies were performed under general anesthesia. The ecoendoscope used was the Olympus-BF-TYPE-UC-180F, with a convex transducer (7.5MHz) and integrated Doppler mode. A dedicated 22-gauge needle (NA-201SX-4022-Olympus) was used to perform TBNA. The ultrasound processor was Olympus-EU-ME1. At least 3 or 4 punctures were made in each target station without rapid on-site cytology. Immunohistochemistry and flow cytometry were requested on all samples. The sample was considered adequate if lymphocytes, antracosis or a specific diagnosis was identified. A true positive diagnosis was made if there was a positive biopsy consistent with lymphoma by EBUS-TBNA or on subsequent follow-up by another method within 6 months. A true negative diagnosis was considered with a negative biopsy and stability or regression of the lymph nodes over a period of at least 6 months.
6.9% (13) patients had clinical suspicion of LPD. 61.5% were male, with mean age of 58.4±15.9 years. Nine patients had enlarged mediastinal lymph nodes and four mediastinal masses.
The EBUS-TBNA results were: three LPD, two granulomatous disease, four reactive lymph nodes and four inadequate samples. Among patients with non-diagnostic results (8), 37.5% (3) had LPD: one patient repeated EBUS-TBNA, one underwent a mediastinoscopy and one patient was diagnosed with LPD by peripheral lymph node biopsy. The diagnosis of reactive lymph node was confirmed in three patients after clinical and radiological monitoring (Table 1).
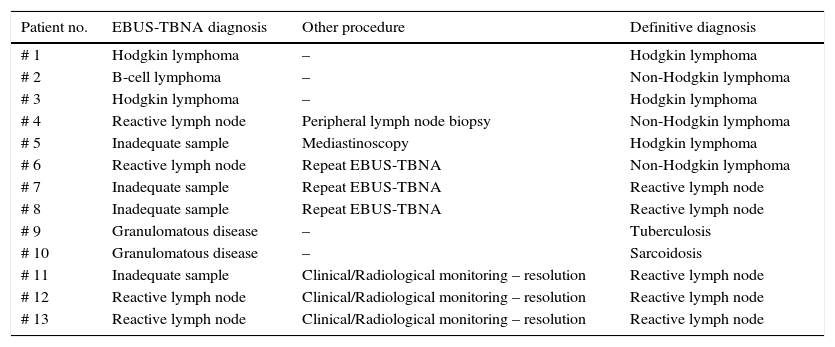
Endobronchial ultrasound needle aspiration results and method of final diagnosis in 13 patients with mediastinal lymph node with suspicion of lymphoma.
| Patient no. | EBUS-TBNA diagnosis | Other procedure | Definitive diagnosis |
|---|---|---|---|
| # 1 | Hodgkin lymphoma | – | Hodgkin lymphoma |
| # 2 | B-cell lymphoma | – | Non-Hodgkin lymphoma |
| # 3 | Hodgkin lymphoma | – | Hodgkin lymphoma |
| # 4 | Reactive lymph node | Peripheral lymph node biopsy | Non-Hodgkin lymphoma |
| # 5 | Inadequate sample | Mediastinoscopy | Hodgkin lymphoma |
| # 6 | Reactive lymph node | Repeat EBUS-TBNA | Non-Hodgkin lymphoma |
| # 7 | Inadequate sample | Repeat EBUS-TBNA | Reactive lymph node |
| # 8 | Inadequate sample | Repeat EBUS-TBNA | Reactive lymph node |
| # 9 | Granulomatous disease | – | Tuberculosis |
| # 10 | Granulomatous disease | – | Sarcoidosis |
| # 11 | Inadequate sample | Clinical/Radiological monitoring – resolution | Reactive lymph node |
| # 12 | Reactive lymph node | Clinical/Radiological monitoring – resolution | Reactive lymph node |
| # 13 | Reactive lymph node | Clinical/Radiological monitoring – resolution | Reactive lymph node |
The diagnosis of LPD was established in six patients. The sensitivity, negative predictive value and diagnostic accuracy of EBUS-TBNA in the diagnosis of LPD were 50, 70 and 76.9%, respectively.
In the literature, the yield of EBUS-TBNA in patients with lymphoma is not well defined with variable results; in the few studies published they vary between 22%1 and 91%.2
In this retrospective case study analysis, the prevalence of LPD was low (46.2%), with a low pretest probability in some cases, which could have hampered sensitivity.
According the Chest guideline about EBUS-TBNA, trials evaluating needle size were reviewed and both 21 and 22 gauge needles are considered adequate.6 The role of 19 gauge needles is yet to be defined, but it is likely that larger needles will provide superior sample quality and improve the yield and sensitivity of EBUS-TBNA in patients with mediastinal adenopathy secondary to lymphoma.
No data exist regarding the number of needle passes required to obtain a sufficient diagnostic yield for lymphoma.6,8 In the absence of rapid on-site evaluation (ROSE), usually 4 passes were done, the latter was used for immunophenotyping.4,7,8
The present study demonstrated that EBUS-TBNA has an important role in the diagnostic workup of mediastinal involvement of LPD. If available, it should be included in the initial evaluation because mediastinoscopy or thoracoscopy pose higher risk to the patient and increased cost. Considering the low negative predictive value of EBUS-TBNA for the diagnosis of lymphoma, patients with inconclusive results must be submitted to further diagnostic investigation.
Conflicts of interestThe authors have no conflicts of interest to declare.


