


During an archaeological excavation at a mediaeval monastery (Flor da Rosa, Crato, Portugal), a skeleton of a adult woman was found with two calcifications in the thoracic cage. The location and the macroscopic analysis of the calcifications allowed them to be assigned as pleural plaques. Spectrometric analysis and scanning electronic microscopy enabled to establish that it originated with an infectious process. These results associated with the lesions found in the ribs and vertebrae strongly suggest tuberculosis as the cause of these pleural plaques.
Durante uma escavação arqueológica de um mosteiro mediaeval (Flor da Rosa, Crato, Portugal) foi encontrado um esqueleto de uma mulher adulta, com 2 calcificações na caixa torácica. A localização e a análise macroscópica das calcificações permitiu que fossem consideradas como placas pleurais. A análise espectrométrica e a microscopia eletrónica de varrimento permitiram determinar que tiveram origem num processo infecioso. Estes resultados, associados com as lesões encontradas nas costelas e vértebras, sugerem nitidamente a tuberculose como causa dessas placas pleurais.
Two pleural plaques (pathological calcifications of soft tissues) were found in the thoracic cage of the skeletal remains of a woman (FR 857), exhumed at the necropolis of the “Mosteiro da Flor da Rosa” (Crato, Portugal), during an archaeological excavation at this mediaeval monastery. The excavation took place between 1989 and 1992 and revealed about one hundred graves inside and around the church. The coins that accompanied some of the burials, which constituted almost the only grave goods, gave a dating for the cemetery between the XIV to the XIX centuries. The skeletons were found in a supine position, their lower limbs were extended and their upper limbs were folded according to Christian ritual practices.
Using infra-red spectroscopy and scanning electronic microscopy to identify the mineral content grades, the structure of the pleural plaque surface and the elemental composition, we suggest that the plaques had an infectious origin, as discussed below. In spite of the fact that the skeleton was in a poor state and incomplete, other interesting pathological lesions were observed: new bone formation on the pleural face of ribs and vertebral body osteolysis.
As far as we know pleural plaques are not a common finding on archaeological series: there are one from Israel,1 two in France,2 three in Switzerland, 3–5one in Slovakia,6 two in Hungary, one from Bácsalmás7,8 and the second from Pitvaros7. All of these pleural plaques, except the one from Bácsalmás, which is reported to date from the 17th century, were mediaeval. The oldest is dated from the 6th century (Saint-Denis, France) and the most recent from the 15th century (Bina, Slovakia). Although the exact dating of the present case is not confirmed, according to the archaeological report9 its stratigraphy strongly suggests the 15th century.
The aim of this study was to describe the pleural plaques and to identify the most probable aetiology.
Material and methodsSex and age diagnoses were performed according to Buikstra & Ubelaker10 recommendations.
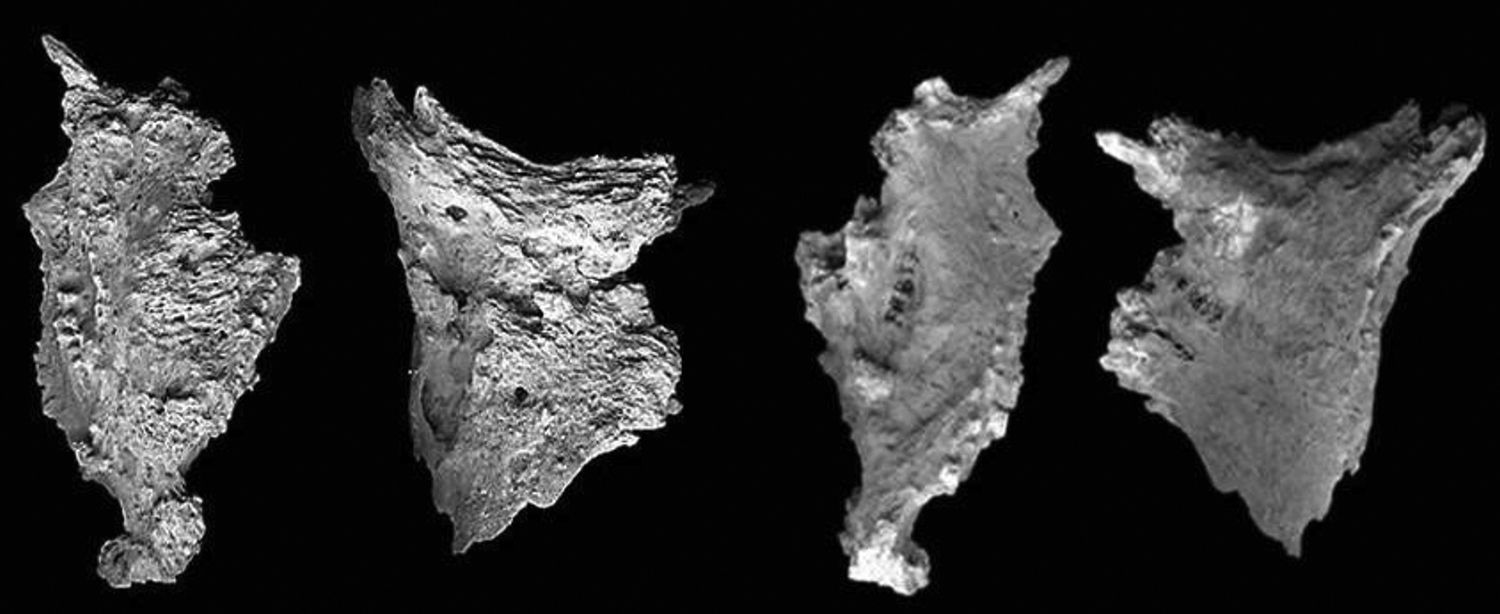
After studying both pleural plaques macroscopically, two samples were taken from the most irregular surface of one of them (fragment II – Fig. 1A and B): one sample of the edge and one sample of the inner side. In order to quantify mineral composition, these samples were analysed by infra-red spectroscopy (Fourier transform IR spectroscopy, according to Pavia et al.11) by Dr. M. Daudon at the Biochemistry Laboratory of the “Hôpital Necker-Enfants Malades” (Paris). Each portion of the bone was ground, mixed with potassium bromide and pressed into pellets, which subsequently were analysed.
 Pleural plaques, external convex side. From left to right: Fragment I; Fragment II (true size). (): Pleural plaques, internal concave side. From left to right: Fragment I; Fragment II (true size). Maximum length, maximum width and average thickness of fragments I and II are, respectively: 64.43/34.14/6.86mm and 55.46/43.43/7.8mm. Scanning electron microscopy (Hitachi TM 3000, SU-70, 30keV) was performed to study the pleural plaques surface and its element composition. Because both fragments were found in the same skeleton and show similar macroscopic aspects, only one of them was analysed.")
(A) Pleural plaques, external convex side. From left to right: Fragment I; Fragment II (true size). (): Pleural plaques, internal concave side. From left to right: Fragment I; Fragment II (true size). Maximum length, maximum width and average thickness of fragments I and II are, respectively: 64.43/34.14/6.86mm and 55.46/43.43/7.8mm. Scanning electron microscopy (Hitachi TM 3000, SU-70, 30keV) was performed to study the pleural plaques surface and its element composition. Because both fragments were found in the same skeleton and show similar macroscopic aspects, only one of them was analysed.
Observation of this poorly preserved skeleton of a woman revealed, in addition to the pleural plaque, deposits of new bone in the pleural surfaces of the ribs, presenting a striated aspect, as well as some lytic lesions in several thoracic vertebral bodies.
Macroscopic observation of the plaques revealed the following features: solid, mineral, thin with spiculated margins, slightly bent (especially the larger one), irregular granular external convex side, smooth and striated internal concave side.
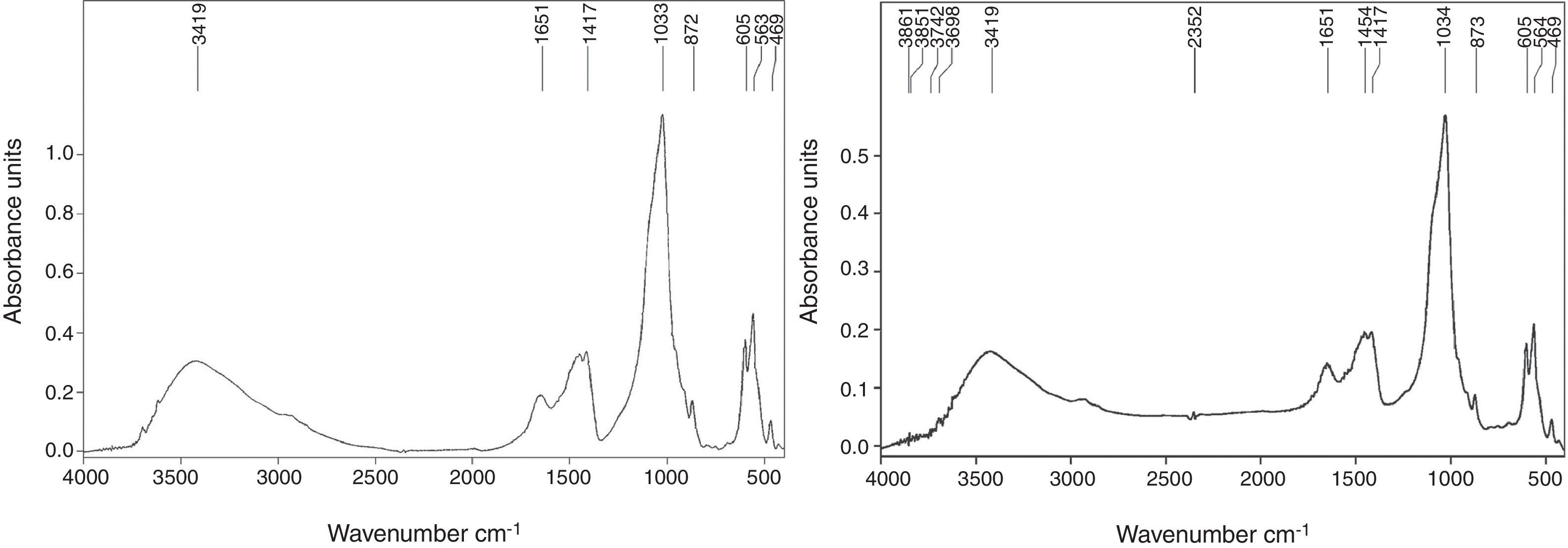
The spectroscopic analysis revealed a similar composition between the edge and the inner side of the plaque fragment (Fig. 2 A and B; Fragment II).
 Spectroscopic analysis of the plaque edges. (B) Spectroscopic analysis of the plaque inner side.")
The following main mineral and organic components were found:
- 1
Carbapatite, usually detected in the band of 1034cm−1, displayed by far the highest values in both graphs.
- 2
Crystalline apatite, commonly detected in the ranges between 564cm−1 and 605cm−1, corresponded to the second highest values obtained.
- 3
The third highest values plotted in our graphs corresponded to a residual protein framework, identified by the bands of 1545cm−1 (starch band 2) and 1650cm−1 (starch band 1) usually connected to CoNH bounds, revealing the good conservation of the CH amino acids.
Although CH bounds seem well preserved, the amount of proteins still present in the plaques was not particularly high, as shown by the 2860cm−1 and 2960cm−1 lines. Phosphates were detected in the 500cm−1 band.
SEM image enabled us to see clusters of granules covering almost the entire pleural plaque surface (Fig. 3).
.")
This technique also provided the approximate element concentration of the plaque surface: oxygen 56.0%; calcium 15.9%; phosphorus 11.1%; silico 5.8%; aluminium 5.1%; sodium 2.0%; iron 1.5%; magnesium 1.1%; potassium 0.8%; chlorine 0.3% and sulfur 0.2%.
Discussion and conclusionsDifferences in surface roughness and orientation of the mineralizations on external and internal surfaces of the plaques presumably result from pleural mechanics. They are due to respiratory movements in the presence of a liquid medium during solidification.
The striking morphological similarity between the two plaques suggests that they probably originated from one complete pleural plaque.
The low level of crystallization, revealed by the low amount of apatite, is observable in the intensity report, by the distance separating the peak 1034cm−1 and the slope 1100cm−1, which excludes a possible confusion with an artefact triggered by post-mortem conditions.2 Moreover, the crystal network of the apatite remains moderately developed (peaks at 564cm−1, 605cm−1), suggesting that the formation occurred not long before the death of the individual. These observations also led us to assume that the infection was active at the moment of death.
Concerning the aetiology of the plaque, the absence of amosite, chrysotile and crocidolite, which are the specific minerals for asbestos, excludes asbestosis as the cause of this pleural plaque. A post-traumatic cause characterized by a calcified haematoma should also be excluded, since there were no traces of hematite and the recorded protein proportion was rather low.2 The exclusion of a strictly taphonomic origin of this calcification lies in the difference in the macroscopic morphology of the inner and outer surfaces which results from respiratory mechanics, and in the presence of CH and proteins in the spectrogram.
The high amount of carbonate ions incorporated in the apatite matrix (30% carbapatite) strongly points to the infectious origin of this pleural plaque, as carbapatite reflects the classic inflammation process. The buildup of inflammatory granuloma dominated by fibrosis tends to calcify and forms carbapatite, which in turn tends to crystallize.12,13
The relative element concentration provided by scanning electron microscopy shows an O, Ca, P molar ratio of 4:1:1 which seems to be compatible with the presence of calcium phosphate (carbapatite), and thus backs up the spectrometric analysis.
Macroscopically both plaques showed changes typical of an infectious origin: the rough side, spiculated, and the smooth side, striated.2,8 It is worth noting the great macroscopical similarity of these plaques to those ascribed to tuberculosis in the literature. In some cases, the agent was confirmed by molecular biology.7,8
The formation of new bone on the ribs combined with the presence of lytic lesions on several vertebral bodies is usually associated with infectious processes, which strengthens the hypothesis that tuberculosis is related to the origin of these calcifications.
Although molecular analysis could make a helpful contribution to the identification of the aetiology of these pleural plaques, it was not performed in this study due to the absence of several conditions regarded as essential for credibility. Among them are the facts that the collection of specimens at the excavation site was not performed under sterile conditions, and the taphonomic factors that might impact on preservation of ancient DNA were not strictly controlled.14,15
The non-renewable nature of archaeological remains, the uncertainty of DNA survival and the rarity of pleural plaques were all significant factors in the decision to not carry out potentially destructive molecular diagnosis at this point.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Authors’ contributionsTF and RG collected the macroscopical data for sex and age diagnosis and for characterization of the plaques and related lesions. PT provided access to spectrometric analysis and its interpretation. All the authors contributed to the final conception of the manuscript.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank Dr. M. Daudon of the Biochemistry Laboratory of the Hôpital Necker-Enfants Malades (INSERM U 90), Paris, for the analysis of the pleural plaque material, and VWR Portugal for scanning electronic microscope utilization.


