

A relevant (but still unpredictable) proportion of patients after COVID-19, particularly those hospitalized with severe acute disease, may present persistent symptoms (i.e. long-COVID syndrome),1 even clustering in specific clinical presentation (i.e. more dyspnea, fatigue, or anxiety/depression, etc).2 Patients suffering from asthma and COPD have been considered less exposed to infection,3 however, there is a lack of data on their prevalence in the long-COVID populations. We hypothesized that individuals with existing chronic airway disease could experience more long term symptoms and/or have respiratory functional impairment 6 months after discharge. Thus we aimed at: i) determining the prevalence of asthma and COPD at the follow-up in a cohort of patients recovering from COVID-19 pneumonia; ii) investigating their dyspnea grade, pulmonary function, and exercise tolerance.
A post-COVID service was established at the Respiratory Outpatient Clinic (University Hospital of Modena Policlinico) for all patients previously hospitalized and cases of SARS-CoV-2 infection not requiring admission for in-person follow up 3-6 months after discharge or recovery from viral infection. Out of 911 patients followed up between July 2020 and February 2022, 780 were hospitalized (85.6%). From the cohort of individuals previously hospitalized, we selected patients with existing diagnosis of asthma or COPD at hospital admission and newly diagnosed at the follow up according to the international guidelines.4,5 Other individuals with asthma or COPD but not hospitalized for COVID-19, patients with confirmed interstitial lung disease, concomitant neuromuscular diseases, cognitive impairment or severe psychiatric disorders, and patients not able to perform follow up assessment were excluded.
This study summarises the clinical-functional assessment of 82 patients (10.5%) reviewed following hospital discharge. The mean time from discharge to follow up was 4 ±1.1 months. Out of 82 individuals, 41 were asthmatic patients and 41 COPD. The prevalence of asthma in the study cohort was 5.2%, and the same for COPD.
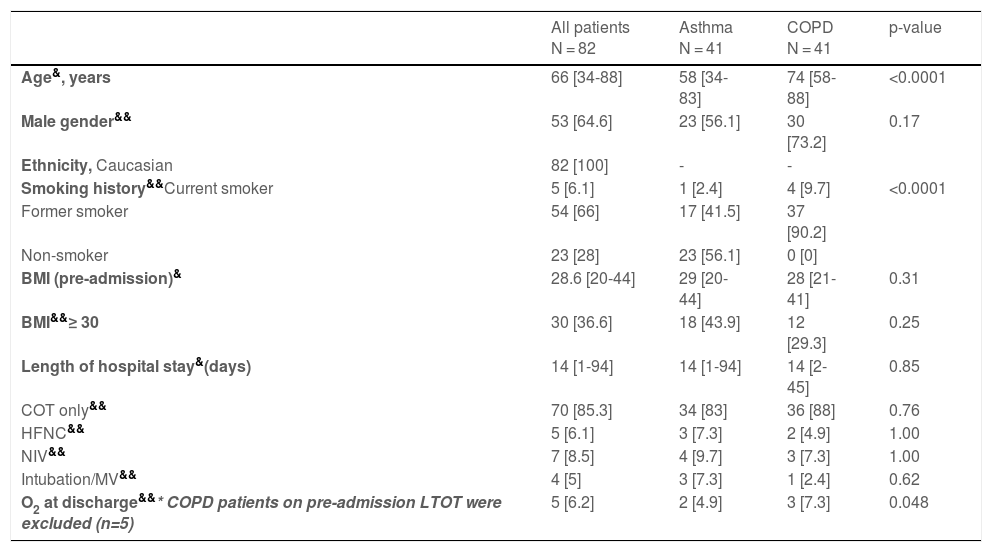
The characteristics of the participants and a summary of their COVID-19 admission are reported in Table 1a; patients with asthma and COPD were similar except for age and smoking history, as expected. Out of 41 patients with asthma, 3 (7.3%) were newly diagnosed, whereas 18 (44%) COPD patients had new diagnosis at the follow up. In patients with asthma, 18 (47%) were allergic, 19 (48%) obese, and 2 (5%) had bronchiectasis. The 23 patients with confirmed COPD were predominantly in GOLD 1-2 grades (87%). The newly diagnosed COPD patients were predominantly male (83%), all former or current smokers, and with similar grade of the disease.
Characteristics of the study population on hospital admission.
| All patients N = 82 | Asthma N = 41 | COPD N = 41 | p-value | |
|---|---|---|---|---|
| Age&, years | 66 [34-88] | 58 [34-83] | 74 [58-88] | <0.0001 |
| Male gender&& | 53 [64.6] | 23 [56.1] | 30 [73.2] | 0.17 |
| Ethnicity, Caucasian | 82 [100] | - | - | |
| Smoking history&&Current smoker | 5 [6.1] | 1 [2.4] | 4 [9.7] | <0.0001 |
| Former smoker | 54 [66] | 17 [41.5] | 37 [90.2] | |
| Non-smoker | 23 [28] | 23 [56.1] | 0 [0] | |
| BMI (pre-admission)& | 28.6 [20-44] | 29 [20-44] | 28 [21-41] | 0.31 |
| BMI&&≥ 30 | 30 [36.6] | 18 [43.9] | 12 [29.3] | 0.25 |
| Length of hospital stay&(days) | 14 [1-94] | 14 [1-94] | 14 [2-45] | 0.85 |
| COT only&& | 70 [85.3] | 34 [83] | 36 [88] | 0.76 |
| HFNC&& | 5 [6.1] | 3 [7.3] | 2 [4.9] | 1.00 |
| NIV&& | 7 [8.5] | 4 [9.7] | 3 [7.3] | 1.00 |
| Intubation/MV&& | 4 [5] | 3 [7.3] | 1 [2.4] | 0.62 |
| O2 at discharge&&* COPD patients on pre-admission LTOT were excluded (n=5) | 5 [6.2] | 2 [4.9] | 3 [7.3] | 0.048 |
Key: Data reported as mean and range or number and % as appropriate.
MV, mechanical ventilation
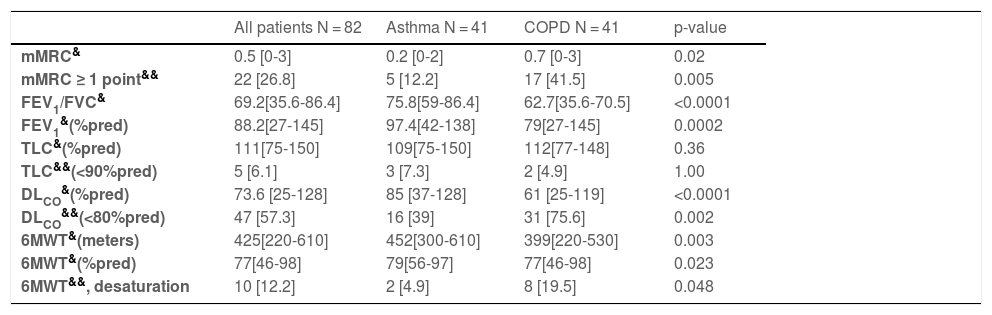
Modified Medical Research Council (mMRC) dyspnea grade,6 spirometry and lung diffusing capacity (DLCO)7 parameters, and six-minute walk distance (6MWT)8,9 were collected at the follow up as outcomes (Table 1b). Persisting oxygen desaturation during exercise was observed in 9.7% of cases: 6 COPD patients with 3 newly diagnosed and 2 asthmatic patients with confirmed diagnosis.
Follow-up assessment in the study population.
| All patients N = 82 | Asthma N = 41 | COPD N = 41 | p-value | |
|---|---|---|---|---|
| mMRC& | 0.5 [0-3] | 0.2 [0-2] | 0.7 [0-3] | 0.02 |
| mMRC ≥ 1 point&& | 22 [26.8] | 5 [12.2] | 17 [41.5] | 0.005 |
| FEV1/FVC& | 69.2[35.6-86.4] | 75.8[59-86.4] | 62.7[35.6-70.5] | <0.0001 |
| FEV1&(%pred) | 88.2[27-145] | 97.4[42-138] | 79[27-145] | 0.0002 |
| TLC&(%pred) | 111[75-150] | 109[75-150] | 112[77-148] | 0.36 |
| TLC&&(<90%pred) | 5 [6.1] | 3 [7.3] | 2 [4.9] | 1.00 |
| DLCO&(%pred) | 73.6 [25-128] | 85 [37-128] | 61 [25-119] | <0.0001 |
| DLCO&&(<80%pred) | 47 [57.3] | 16 [39] | 31 [75.6] | 0.002 |
| 6MWT&(meters) | 425[220-610] | 452[300-610] | 399[220-530] | 0.003 |
| 6MWT&(%pred) | 77[46-98] | 79[56-97] | 77[46-98] | 0.023 |
| 6MWT&&, desaturation | 10 [12.2] | 2 [4.9] | 8 [19.5] | 0.048 |
Key: Data reported as mean and range or number and % as appropriate.
According to the study purpose, we were able to show interesting findings.
First, data collection helped quantify the proportion of patients with diagnosis of asthma and COPD in a large cohort of people at the follow up after COVID-19 pneumonia. The prevalence of asthmatic patients is in line with that observed in the general population in Italy,10 but it seems larger than previously reported data in COVID-19 patients.11,12 On the other hand, COPD patients in our study cohort are less prevalent than in the general population,13 which may support a different epidemiology within COVID-19 patients.3 Notwithstanding, the follow-up service provided a new diagnosis of chronic respiratory disease, particularly COPD. This provided patients with an opportunity for an appropriate disease identification and care plan.
Second, a clinically meaningful post-COVID mMRC dyspnea score observed in 41.5% of the COPD patients, who were in mild GOLD grade of severity, confirms the findings of Huang et al in a large population of patients discharged in Wuhan and assessed six months later.14 This emphasises that older age is not the only responsible factor for long-term residual dyspnea in COPD survivors.
Third, the reduction in DLCO (mean 73.6% pred with <80%pred in 57.3% of cases) as a marker of residual lung damage following interstitial pneumonia was similar to that observed in unselected patients treated with respiratory support therapies (HFNC, NIV, intubation),14-16 even though more frequent in COPD (75.6%) than in patients with asthma in our cohort.
Finally, the great proportion of people with asthma and obesity (43.9%), confirmed that this comorbidity makes asthma difficult to treat17 and may also impact negatively on the patient's perception of good health in individuals recovering from COVID-19.
Considering major limitations (i.e. the single-center analysis and the lack of pre-to-post comparison of pulmonary function test in patients with existing diagnosis of asthma and COPD), the study results are informative. Indeed, the patients with asthma and COPD is a representative real-word disease-group, and the follow up assessment can be useful for unknown diagnoses of chronic respiratory disease. Therefore, the findings highlight the importance of a tight respiratory follow-up assessment in individuals recovering from COVID-19 pneumonia who should be investigated for long-term symptoms including dyspnea, especially those underdiagnosed for having asthma or COPD.
FundingEC have received research grant support from Chiesi Italia S.p.A. (letter of intent signed on 09/04/2021).
Consent for data publicationThe consent for data publication was given by the Ethics Committee (CE 453/2020-OSS/AOUMO and CE EM453/2020-OSS/AOUMO).
None.


