


Maximal inspiratory pressures (MIP) and maximal expiratory pressures (MEP) are useful indices of respiratory muscle strength in athletes.
The aims of this study were: to describe the strength of the respiratory muscles of Olympic junior swim team, at baseline and after a standard physical training; and to determine if there is a differential inspiratory and expiratory pressure response to the physical training.
A cross-sectional study evaluated 28 international-level swimmers with ages ranging from 15 to 17 years, 19 (61%) being males. At baseline, MIP was found to be lower in females (P=.001). The mean values reached by males and females were: MIP(cmH2O) = M: 100.4 (±26.5)/F: 67.8 (±23.2); MEP (cmH2O)=M: 87.4 (±20.7)/F: 73.9 (±17.3). After the physical training they reached: MIP (cmH2O)=M: 95.3 (±30.3)/F: 71.8 (±35.6); MEP (cmH2O)=M: 82.8 (±26.2)/F: 70.4 (±8.3).
No differential pressure responses were observed in either males or females. These results suggest that swimmers can sustain the magnitude of the initial maximal pressures. Other studies should be developed to clarify if MIP and MEP could be used as a marker of an athlete's performance
Pressões inspiratórias máximas (PIM) e pressões expiratórias máximas (PEM) são indicadores úteis de força muscular em atletas.
Os objetivos desse estudo foram: descrever a força da musculatura respiratória de uma equipe Olímpica júnior de natação, em repouso e após um exercício físico padronizado e. determinar o diferencial de pressão inspiratória e expiratória obtido como resposta ao exercício físico.
Um estudo descritivo avaliou 28 nadadores de nível internacional, com idades variáveis entre 15 a 17 anos, sendo 19 (61%) do sexo masculino. Em repouso, os valores mais baixos de PIM foram encontrados no sexo feminino (p=0,001). Os valores médios alcançados no sexo masculino (M) e feminino (F) foram: PIM (cmH2O)=M: 100,4 (±26,5)/F: 67,8 (±23,2); PEM(cmH2O)=M: 87,4 (±20,7)/F: 73,9 (±17,3). Após o exercício físico foram obtidos os seguintes valores: PIM (cmH2O) = M: 95,3 (±30,3)/F: 71,8 (±35,6); PEM (cmH2O)=M: 82,8 (±26,2)/F: 70,4 (±8,3).
Não foram registrados diferenciais de pressões inspiratórias e expiratórias máximas em resposta ao exercício, em ambos os sexos. Esses resultados sugerem que os nadadores olímpicos conseguiram sustentar a magnitude das pressões máximas iniciais. No entanto, outros estudos deverão ser realizados afim de verificar se PIM e PEM poderiam ser empregados como marcadores de performance de atletas
Nowadays, elite athletes from various sports, including swimming, undertake specific training to build the respiratory muscles, hoping to improve their competitive results.
During exercise the body's demand for oxygen increases and the breathing volume must also rise. This requires numerous muscles surrounding the lungs to contract in a highly coordinated manner. As the intensity of exercise increases, these respiratory muscles must contract more forcefully and quickly to keep pace with the bodies increase in metabolism. This important role of the respiratory muscles has generated great interest in respiratory muscle fitness.
Early studies examining respiratory muscle training demonstrated that the strength of the respiratory muscles can be enhanced and that improvements were specific to the type of training undertaken, even in highly trained athletes. 1 Importantly, this indicates there is potential for improving respiratory muscle function, even in those individuals who undertake heavy physical training on a regular basis. Thus, it is generally accepted that maximal inspiratory pressures (MIP) and maximal expiratory pressures (MEP) are useful for the assessment of respiratory muscle performance in adults and children. Surprisingly, measurement of respiratory muscle strength has not been widely investigated in the context of competitive swimming, although this sport presents an exceptionally challenging exercise environment. International-level swimmers represent a group of individuals who traditionally have the most highly developed respiratory systems and muscles due to the breathing requirements of the sport.2,3. Furthermore, inspiratory muscle training might result in an improvement in performance among competitive athletes.4
The aim of this study was threefold: First, to assess the strength of the respiratory muscles in international-level swimmers at baseline as well as after a standard physical training; Second, to determine if there is a differential inspiratory and expiratory pressure response to standard physical training and to examine the pulmonary function at the baseline; Third, to compare maximal pressures according to gender.
Subjects and methodsThis was a cross-sectional study of Brazilian world-ranked swimmers that was conducted during August 2006. Thirty-one international-level swimmers participated in the study.
All swimmers were non-smokers and without any current clinical problems. They were not receiving any medical therapy, ergogenic supplements or other nutritional aids.
Prior to participation, informed written consent and ethics committee approval were obtained.
The mean (SD) values for the participants according to gender were: 1) girls (n = 12): age, 16.25 (± 0.62) years; height, 167 (± 0.06) cm; weight, 56 (± 4.99) kg; swimming style: sprinter (n = 6), long distance (n = 6); 2) boys (n = 19): age, 16.53 (± 0.77) years; height, 182 (± 0.07) cm; weight, 75.1 (± 7.44) kg; swimming style, sprinter (n = 9), long distance (n = 10).
The BMI was obtained by collecting the height and body mass of participants in the study. For body mass measurements, a Filizola® (model PL 200, Sao Paulo, Brazil) digital scale with a maximum capacity of 300kg was used. Height was obtained using a ruler fixed to the scale. BMI was obtained through dividing the body mass (kg) by the height squared (m2). BMI categories were based on the revised CDC growth chart and definitions.5
Respiratory muscle strength was measured as the maximum inspiratory and expiratory mouth pressures. MIP and MEP were measured using an analogical manovacuometer (± 300 cmH2O) Medica® (model M120, Sao Paulo, Brazil). The manometer calibration was in accordance with the manufacturer's recommendations. During the test, the individuals remained seated with their nasal airflow interrupted by a nose clip. MIP was always taken after a maximal expiration, while MEP was registered from total lung capacity.
Before measurements were taken, each individual was familiarized with the equipment and shown how the maneuvers were to be done. The maximal inspiratory and expiratory pressure maneuvers were carried out for a minimum of three trials with an interval of one minute between them. The maximal respiratory effort was sustained for approximately one second.6 The highest value of three correctly accomplished repetitions (difference of 10 % or less between trial values) was recorded for each trial. A single researcher, using the same verbal commands, performed the manovacuometer measurements for all individuals.
The measurement procedures followed the American Thoracic Society (ATS)/European Respiratory Society (ERS) statement on respiratory muscle testing.7
During the test session, a 10-minute whole body-stretching warm-up was followed by a 30-minute standard physical training according to the Brazilian Olympic protocol.8 This training included a maximal swimming effort at the end. Participants were instructed to achieve their fastest time over a 1200m free-swimming test.
All swimming tests were conducted in an indoor 25m swimming pool. The temperature of the water was 260°C. All tests were performed at the same time of the day to control for the effects of diurnal variation.
Measurements of MIP and MEP were done just before and after the training session and were performed at the poolside. The post-test was conducted immediately after finishing the 1200m free swim to minimize the recovery time available to the respiratory muscles for post-exercise assessment. Baseline measurements were compared to post physical session for differences in MIP and MEP.
Baseline spirometric parameters FVC, FEV1 and PEF were measured in the standing posture before the athletes were submitted to the physical training and after the ventilatory strength measurements. A portable spirometer (Micro Medical®, Kent, United Kingdom) was used in accordance to the procedures recommended by the European Respiratory Society.9
The subjects were asked to inhale completely and perform a forced expiratory vital capacity maneuver (FVC). This procedure was repeated until three satisfactory tracings were obtained. From these recordings we selected the largest value of FEV1. Both FEV1 and FVC were recorded as percent of predicted normal values. The largest PEF values were reported as well.
Results were shown by means, standard deviations and percentages. Statistical analyses were performed separately for males and females. The Kolmogorov-Smirnov test was used to investigate the data distribution. The respiratory muscle strength data were analyzed using paired (within group) and unpaired (between groups) t- tests. Statistical significance was set at P value = .05. All statistical analyses were conducted using SPSS for Windows v15.0. 10
ResultsThe studied sample of 31 subjects represents the whole junior team of Brazilian world-ranked swimmers.
BMI were higher in males than in females: 22.75 ± 1.8 and 20.11 ± 1.6, respectively (P < .001). Three (15.8 %) male athletes were classified as being at risk for overweight while the remaining were categorized as healthy weight.
Three male international-level swimmers were excluded from the analysis of the differential respiratory pressures (MIP/ MEP) response to the physical session. They alleged fatigue as the reason for not finishing the tests. The following mean (SD) values were observed at the baseline assessment: MIP = 85.6 cmH20 (± 10.2); MEP = 89.3 cmH20 (± 6.7); FEV1 = 4.7L/second (± 0.5); FEV1 % predicted = 121.6 (± 13.7); FVC = 5.8L (± 0.5); FVC % predicted = 165.7L (± 1.1) and PEF = 9.5L/second (± 1.6).
Mean values of MIP and MEP are presented in Figure 1.

There were no differences in mean values of MIP and MEP at baseline assessment compared to post exercise session, in either sex. Furthermore, both gender groups showed similar mean values of MIP and MEP, except at MIP baseline assessment when male swimmers reached a higher value (P < .001).
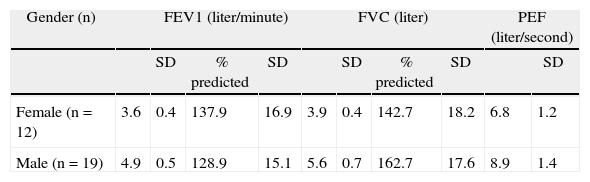
Table 1 shows ventilatory indices reached by female and male groups. Higher mean values of FEV1 and PEF were observed in male athletes compared to females (P < .001). Conversely, no difference between sexes was related to FVC (P > .05).
DiscussionTo the best of our knowledge this is the first study focused on MIP and MEP variation conducted in Brazilian athletes.
The main finding of this work is that mean values of MIP and MEP of male and female adolescent swimmers did not change significantly after the physical session. Thus, no MIP and MEP differential pressure responses to exercise suggest that these 28 athletes could sustain the magnitude of the initial maximal respiratory pressures. It is conceivable that international-level swimmers, who are used to upper limits of swimming exercises, were physically prepared and as a result, the exercise session induced no inspiratory or expiratory muscle strength decrease.
At baseline assessment, we observed a gender difference in MIP, with male swimmers reaching higher mean values. Pulmonary structural and morphologic differences between genders include smaller vital capacity and maximal expiratory flow rates, reduced airway diameter, and a smaller diffusion surface than among men of the same age and height. These differences may have an effect on the integrated ventilatory response, respiratory muscle work, and on pulmonary gas exchange during exercise. The consequence of these pulmonary effects is the potential impact on aerobic capacity and exercise tolerance, influencing the training response. 11–13 However, gender differences in MEP were not observed in our study.
Both male and female groups spirometric values were above percentages of predicted values. These findings were similar to those found by Armour, Donnelly and Bye.14 They suggest that adolescent swimmers may achieve greater lung volumes not because of greater inspiratory muscle strength, or differences in height, fat free mass, alveolar distensibility, age at start of training or sternal length or chest depth, but by developing physically wider chests, containing an increased number of alveoli, rather than alveoli of increased size. Even a larger static lung volume in swimmers is described as a consequence of an adaptational growth.15,16
Three male swimmers complained of fatigue. Their physical characteristics showed no particular feature that might explain their inability to complete the test. Although several studies found that, in general, athletes had greater fatigue resistance, none of them provided sufficient evidence of an association between athletic training and fatigue resistant respiratory muscles.17,18 Furthermore the influence of a common genetic predisposition for athleticism and strong respiratory muscles should not be ignored. 19,20 It is important to highlight that each measurement of MIP was made from residual volume, which has been shown to increase following exercise. As a result the diaphragm may be placed at a less than optimal position and thus make it less able to develop an appropriate pressure.3
It is known that appropriate body weight maintenance is important for athletic performance. According to the BMI percentiles employed in the present study three swimmers were considered at risk of being overweight. 20 BMI should be used cautiously when classifying fatness in international-level swimmers as a consequence of a high body weight due to a higher lean body mass.20,21
The results of the present study may have limitations connected to the lack of spirometric tests taken after the physical session to observe possible lung volume changes after maximal exercise training. Furthermore, the cross-sectional nature of this study made it impossible to discern causal relationships.
Another limitation to the study could be the motivation of the subjects to perform maximal respiratory maneuvers following the exercise session. This is difficult to assess, however, as measurements were performed during the pre Olympic training we believe the athletes were highly motivated.
ConclusionsNo changes were observed in the mean values of MIP and MEP for either gender measured at baseline and after a standard physical training. These results suggest that the swimmers could sustain the magnitude of the initial maximal pressures, with males presenting higher mean values of MIP at baseline.
Considering the uniqueness of the swimming environment, it is reasonable to suppose that measuring respiratory muscle function would be relevant to indicate the health of the respiratory system and to monitor the progress of swimmers' respiratory muscle training. Longitudinal studies focused on MIP and MEP should be developed in order to clarify whether both measures could be used as a guide of high-intensity training programs and a marker of the athletes' performance.
Conflict of interestAuthors declare that they don't have any conflict of interest.
The authors would like to thank the Brazilian Aquatic Sports Confederation (Confederação Brasileira de Desportos Aquáticos - CBDA) and Jon Haliburton for helping with manuscript translation.
The research was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES - Brazil).


