

In the study of lung lesions, tissue samples necessary for a pathomorphological assessment may be obtained by different techniques: surgical, bronchoscopic and percutaneous methods (like computed tomography (CT) guided transthoracic needle biopsy (TTNB) by fine-needle aspiration biopsy (FNAB) or by core-needle biopsy (CNB)).1 The decision to perform FNAB or CNB is multifactorial and highly operator dependent. The diagnostic accuracy of FNAB is almost as good as CNB in the diagnosis of malignant lesions, especially if onsite cytopathological evaluation is available.2 However, for diagnosis of benign lesions CNB is preferred, with a diagnostic yield of 52–91%, when compared to 20–50% with FNAB, for definitive diagnosis of benign lesions.3 Although CT-guided CNB has been shown to be an accurate means of diagnosing lung malignancies, there is relatively little information about its utility in diagnosing benign conditions.4 Previous series of lung CNB have included benign diagnosis but have not provided details of the histological features,4 and there are no studies specifically addressing interstitial lung diseases (ILD). The aim of this work is to evaluate the use of CT-guided CNB in patients with suspected ILD: diagnostic yield for the different types of ILD, factors that influence it and complications.
All patients followed in our ILD outpatient clinic with suspected ILD, who underwent CT-guided CNB between 08/2010 and 02/2015, were consecutively recruited into this prospective study. All cases were discussed in a multidisciplinary meeting before being proposed to CT-guided CNB. Before the procedure, risks and possible complications were explained to each patient and informed consent was obtained. The procedure was performed by an interventional radiologist. All cases were performed using the Philips 16-slice spiral CT (120kV, 250mA and a 3-mm thickness; Philips Healthcare, Andover, MA, USA) for imaging guidance. The biopsy tool used was an automated biopsy gun (Magnum™, Bard Biopsy Systems, AZ, USA) with an 18 or 20-gauge needle. The patient lay on the CT table and the puncture point and access routine were determined by CT scan to a desired area of diseased lung. Following local anesthesia, the needle was inserted through the skin and advanced to the lesion. CT scans were performed to confirm the position of the needle. Once the needle was located in an appropriate position within or near the lesion, the operator triggered the needle, trapping the specimen in the sample notch. Immediately after the procedure, a chest CT scan was performed to evaluate post procedural complications and 1 and 4h after the procedure the patient performed a chest X-ray. Data were analyzed with SPSS 19.0, the χ2 test was used for the statistical analysis. Statistical significance was attributed to p<0.05.
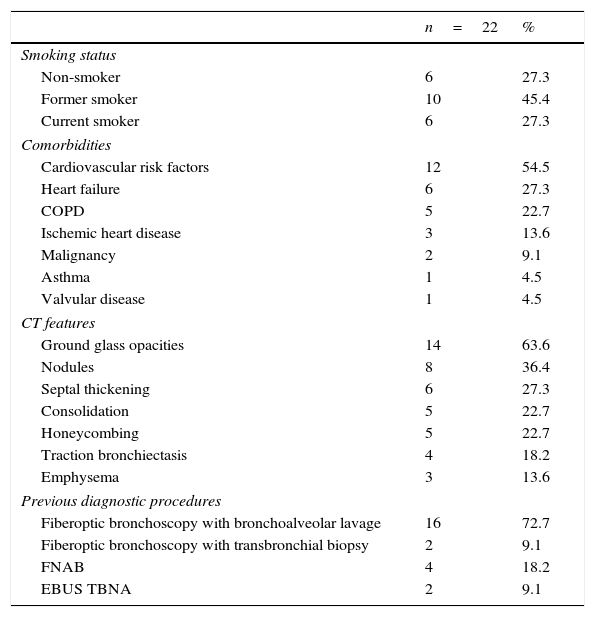
During the study period 22 patients underwent CT-guided CNB (22 CNB). Table 1 shows their characteristics.
Patients characteristics (CT, computed tomography; FNAB, fine-needle aspiration biopsy; EBUS-TBNA, endobronchial ultrasound transbronchial needle aspiration).
| n=22 | % | |
|---|---|---|
| Smoking status | ||
| Non-smoker | 6 | 27.3 |
| Former smoker | 10 | 45.4 |
| Current smoker | 6 | 27.3 |
| Comorbidities | ||
| Cardiovascular risk factors | 12 | 54.5 |
| Heart failure | 6 | 27.3 |
| COPD | 5 | 22.7 |
| Ischemic heart disease | 3 | 13.6 |
| Malignancy | 2 | 9.1 |
| Asthma | 1 | 4.5 |
| Valvular disease | 1 | 4.5 |
| CT features | ||
| Ground glass opacities | 14 | 63.6 |
| Nodules | 8 | 36.4 |
| Septal thickening | 6 | 27.3 |
| Consolidation | 5 | 22.7 |
| Honeycombing | 5 | 22.7 |
| Traction bronchiectasis | 4 | 18.2 |
| Emphysema | 3 | 13.6 |
| Previous diagnostic procedures | ||
| Fiberoptic bronchoscopy with bronchoalveolar lavage | 16 | 72.7 |
| Fiberoptic bronchoscopy with transbronchial biopsy | 2 | 9.1 |
| FNAB | 4 | 18.2 |
| EBUS TBNA | 2 | 9.1 |
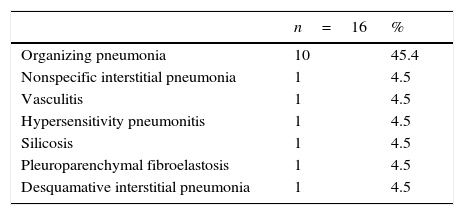
The main reasons for performing CNB were: surgical contra-indications (n=15; 68.2%) and patient refusal of surgical lung biopsy (n=7; 31.8%). Diagnostic histological features were obtained in 17 cases (77.3%). The suspected diagnosis was confirmed, after multidisciplinary meeting, in 16 cases (72.7%), as shown in Table 2. Multivariate statistical analysis indicated no statistically significant predictors of histological diagnosis.
Organizing pneumonia was significantly more diagnosed with CNB in patients with consolidations on CT and ground glass opacities (p<0.05). Minor complications were observed in 5 (22.7%) cases (4 alveolar hemorrhage and 1 pneumothorax requiring invasive chest tube drainage). No patient required hospitalization. The occurrence of complications was significantly higher in current smokers (p<0.05; 5 vs. 0) and COPD patients (p<0.05; 5 vs. 0). The median follow-up of the patients with confirmed diagnosis after the CNB was 18.3±10.9 months.
CT-guided lung biopsy is a diagnostic procedure with a high diagnostic accuracy for benign pulmonary lesions.5 At this point, to the best of the authors’ knowledge, this study was the only one where only suspected ILD patients submitted to CNB were analyzed. This study had some limitations such as being a retrospective study and the small sample size. There is also an important bias related to the selection of patients with lesions considered more suitable for transthoracic approach. In our study we had a diagnostic yield of 73%, which is consistent with the literature reports for benign disease.4 After multidisciplinary discussion, organizing pneumonia was diagnosed in almost half of the cases (45%), and the same diagnosis was maintained throughout the follow-up in all patients. As it is the first study of CT-guided CNB specifically in patients with suspected ILD, it brings new information about the usefulness of CNB in this setting. CT-guided CNB is a safe and valid procedure in the diagnostic approach of selected patients with suspected ILD, particularly in patients with suspected OP. Due to the size of our sample, as well as the selection bias, more studies are needed to confirm the role of this technique in the diagnosis of ILD.
Conflicts of interestThe authors have no conflicts of interest to declare.


