

The term “textiloma” (also “gossypiboma”) describes a sponge or other retained surgical material and the surrounding foreign body reaction. The most frequent sites of intrathoracic textiloma are the pleural and pericardial cavities. Textilomas are essentially inert and lead to aseptic foreign body reactions with fibroblastic reactions and encapsulation. This rare iatrogenic complication of surgery can have severe medical consequences, such as infection or formation of absesses. Because of its rarity, the diagnosis of textiloma is easily overlooked, particularly when the clinical presentation is delayed. Some patients remain clinically asymptomatic for many years, and then present clinical signs. The most common clinical manifestations are chest pain and cough.1–5
A 56 year-old man was admitted with cough and chest pain. The patient had undergone myocardial revascularization 6 months previously. A chest radiograph showed opacity in the lower left hemithorax. All laboratory tests were normal. A chest computed tomography demonstrated a posterior well-defined mass in the middle third of the left hemithorax, in close contact with the pleural surface (Fig. 1). Surgical exploration revealed well-encapsulated surgical gauze in the left hemithorax.
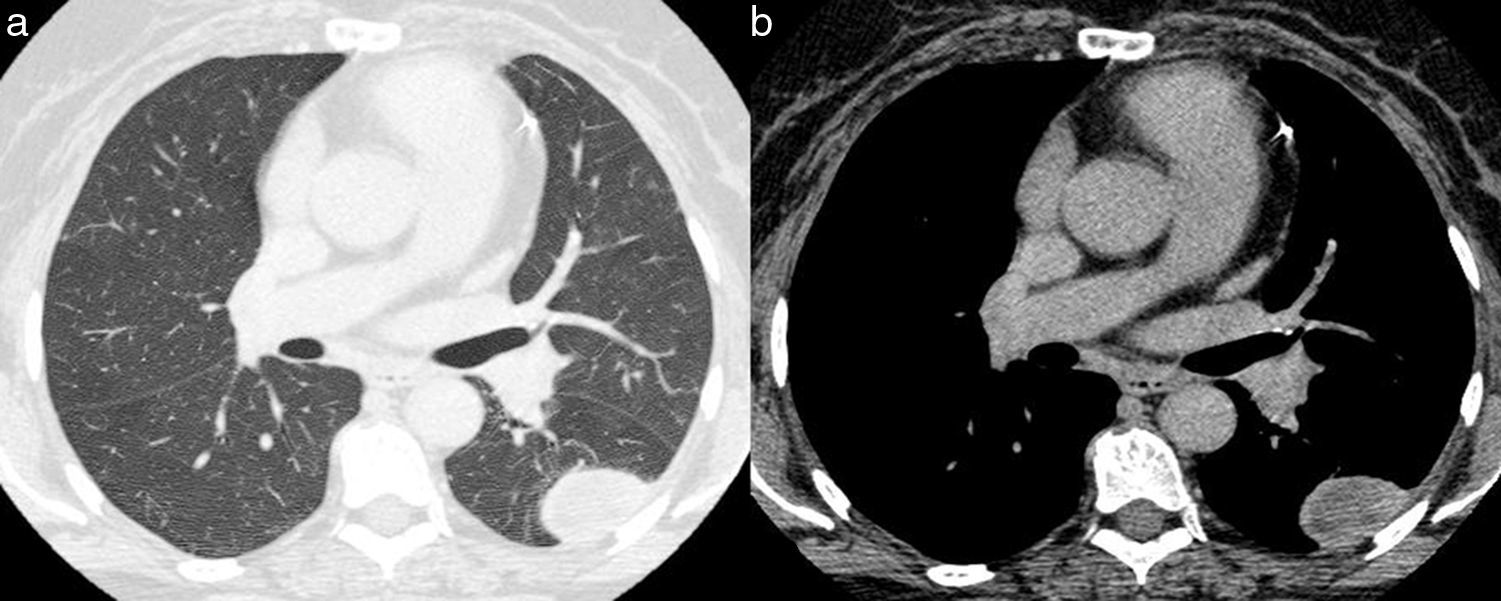
 and mediastinal (b) window settings reveal a well-defined mass of probable extrapulmonary origin (the larger diameter is related to the pleural surface, and the mass, in its anterior portion, forms an obtuse angle with the chest wall), located posteriorly in the middle third of the left hemithorax, in close contact with the pleural surface.")
Axial chest computed tomography images obtained with the pulmonary (a) and mediastinal (b) window settings reveal a well-defined mass of probable extrapulmonary origin (the larger diameter is related to the pleural surface, and the mass, in its anterior portion, forms an obtuse angle with the chest wall), located posteriorly in the middle third of the left hemithorax, in close contact with the pleural surface.
Computed tomography (CT) is the most effective method for detecting a retained intrathoracic textiloma. Thoracic textilomas most commonly present on CT as masses with regular contours and well-defined borders, demonstrating peripheral enhancement with the use of intravenous contrast material. The inner region frequently shows heterogeneous density and findings consistent with gas, calcification, sponge-like material, or a radiopaque marker.2–5 Gas may be present in the sponge mesh, resulting in a whorl-like pattern.4 However, a surgical sponge left in the pleural space does not typically result in images of gas because of the reabsorption of air by the pleura, which usually occurs within the first 30 days after surgery.2 Later, atypical calcification and the thick, irregular inflammatory wall of the mass may mimic a chronic infectious or granulomatous process or neoplasm. The inner region may present a folded or spongiform pattern, with or without air bubbles.2,3 In the early postoperative period, such radiological findings may be confused with abscess formation and complicated hematoma or seroma. The mass may also contain wavy, striped, high-density areas that represent the sponge itself, with a typical whorl-like appearance corresponding to the sponge fibers.2,4 The incorporation of radiopaque markers in swabs can significantly aid the radiological detection of a retained swab.2,5 When a radiopaque filament is present, the correct diagnosis may be established by plain radiography.4
In conclusion, textiloma is a rare complication of thoracic surgery. Because of its non-specific clinical and radiographic presentations, the diagnosis of intrathoracic textiloma may be easily overlooked. Early recognition and prompt treatment will reduce the sequelae of this undesirable condition. Thus, textiloma should be included in the differential diagnosis of an intrathoracic mass, in addition to hematoma and abscess formation, in any patient who has undergone thoracotomy.
Conflicts of interestThe authors have no conflicts of interest to declare.


