

This study aims to evaluate compliance of HIV patients to TB screening and treatment, identifying determinants for non-compliance.
We reviewed clinical records of all HIV infected patients first attended in a Portuguese-Infectious-Unit from 2007 to 2010 (152 patients). Screening included: symptom inquiry, chest X-ray, TST/IGRA. In 2008 a protocol was established with a TB outpatient clinic allowing patients to choose where to perform screening (decentralization).
All patients were offered screening; 69 (45.4%) accepted. Before decentralization, out of 78 patients, 20 (25%) accepted screening. After decentralization, out of 64 patients, 49 (76.6%) accepted screening. Decentralization was associated with higher levels of acceptance (p<0.001), having an AIDS-defining-disease (p=0.002) and being older (p=0.04) was associated with lower screening acceptance. LTBI was diagnosed in 14 and active-TB in 18 cases; 14 cases of active-TB were later diagnosed during hospital appointments. For active-TB, being on HAART was related with treatment adherence (p=0.03).
In this population, improving health care access was important for screening compliance.
Este estudo teve por objetivo avaliar a adesão dos doentes VIH ao rastreio e tratamento da TB, identificando fatores determinantes para a não adesão.
Foram revistos os registos clínicos de todos os doentes infetados pelo VIH, observados pela primeira vez numa Unidade de Doenças Infeciosas Portuguesa entre 2007 e 2010 (152 doentes). O rastreio incluía: inquérito de sintomas, telerradiografia torácica e TST/IGRA. Em 2008, foi estabelecido um protocolo com um Centro Diagnóstico Pneumológico, que permitia aos doentes escolher o local para serem rastreados (descentralização).
O rastreio foi oferecido a todos os doentes, tendo 69 (45%) aceitado. Antes da implementação do protocolo de descentralização, de 78 doentes, 20 (25%) aceitaram ser rastreados. Após a descentralização, de 64, 49 doentes (76,6%) aderiram ao rastreio. A descentralização dos cuidados de saúde mostrou estar associada a uma maior adesão ao rastreio (p<0,001); enquanto ter uma doença definidora de sida (p=0,002) ou ter mais idade (p=0,04) foram associados a uma menor adesão ao rastreio.
O diagnóstico de TB infeção latente foi feito em 14 doentes e de TB ativa em 18; 14 casos de TB ativa foram diagnosticados posteriormente durante o seguimento em consulta hospitalar. Nos doentes com TB ativa, estar em terapêutica HAART mostrou associação com a adesão ao tratamento da TB (p=0,03). Nesta população, a melhoria no acesso aos cuidados de saúde foi importante na aceitação do rastreio de tuberculose.
The risk of tuberculosis (TB) is 20–37 times higher in human immunodeficiency virus (HIV) infected individuals than in non-infected1 and for HIV patients with latent tuberculosis infection (LTBI) the annual risk of developing active-TB is 5–10%.1 Identification and preventive treatment of HIV individuals with LTBI, are a priority in the fight against TB.2 This study aimed to analyze TB screening compliance in HIV patients and to address the identification of determinants for TB treatment non-compliance.
MethodologyWe reviewed clinical records of all individuals (inpatients and outpatients) with HIV infection, first attended in a Portuguese Hospital Infectious Unit (responsible for a population of 330,000 inhabitants) from 2007 to 2010.
In 2008, a protocol was established with a TB outpatient clinic with the aim of improving access to health care (decentralization) – TB screening could be done in the Hospital Unit or TB outpatient clinic, according to patient preference. It included: symptom inquiry, chest radiography, tuberculin skin test (TST) and interferon-gamma-release-assay (IGRA). Sputum smear and culture were performed when active-TB was suspected.
Whenever active-TB was diagnosed, combined free of charge treatment was offered and since 2008, patients have been able to choose where to take medication (directly observed-treatment). The decision to initiate preventive therapy included: TST (≥5mm) and/or IGRA positive, after active-TB exclusion. Candidates to initiate preventive therapy (IPT) were offered self-administered daily isoniazid for 9 months. Treatment compliance was assumed if ≥80% of prescribed doses were taken. Preventive treatment compliance was assumed for patients who came every week to collect medication and monthly to clinical appointment.
Statistical analysisTwo groups were studied – those who accepted and those who declined screening, and later on, those that “accept” or “decline” treatment. Univariate and multivariate logistic regression were performed. Odds-ratios and associated 95% confidence intervals were calculated. Statistical significance was assumed for p-values≤0.05.
ResultsDuring the period studied, 152 patients were attended to, 114 (75%) men, mean age 38.5 years-old. The mean CD4 count was 279cells/μl; 60 (39.4%) injecting drug users; 46 (30.2%) had heterosexual and 21 (13.8%) homosexual risk behaviour. In 25 patients, the cause of HIV infection was: unknown (20), transfusion4 and congenital.1 Fifteen patients had TB exposure and 9 previous history of TB; 64 had Hepatitis C virus (HCV) (42.1%), 12 (7.8%) had Hepatitis B virus (HBV) co-infection and 34 (22.3%) clinically defined AIDS (Table 1). Seventy-four patients had known HIV infection at first hospital attendance.
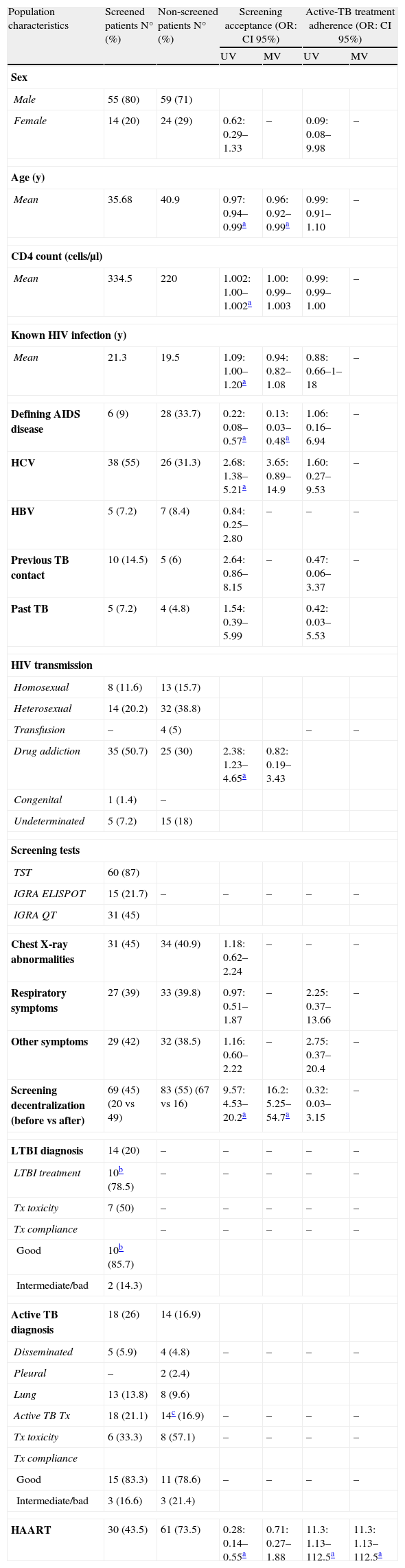
HIV population description and analysis.
| Population characteristics | Screened patients N° (%) | Non-screened patients N° (%) | Screening acceptance (OR: CI 95%) | Active-TB treatment adherence (OR: CI 95%) | ||
| UV | MV | UV | MV | |||
| Sex | ||||||
| Male | 55 (80) | 59 (71) | ||||
| Female | 14 (20) | 24 (29) | 0.62: 0.29–1.33 | – | 0.09: 0.08–9.98 | – |
| Age (y) | ||||||
| Mean | 35.68 | 40.9 | 0.97: 0.94–0.99a | 0.96: 0.92–0.99a | 0.99: 0.91–1.10 | – |
| CD4 count (cells/μl) | ||||||
| Mean | 334.5 | 220 | 1.002: 1.00–1.002a | 1.00: 0.99–1.003 | 0.99: 0.99–1.00 | – |
| Known HIV infection (y) | ||||||
| Mean | 21.3 | 19.5 | 1.09: 1.00–1.20a | 0.94: 0.82–1.08 | 0.88: 0.66–1–18 | – |
| Defining AIDS disease | 6 (9) | 28 (33.7) | 0.22: 0.08–0.57a | 0.13: 0.03–0.48a | 1.06: 0.16–6.94 | – |
| HCV | 38 (55) | 26 (31.3) | 2.68: 1.38–5.21a | 3.65: 0.89–14.9 | 1.60: 0.27–9.53 | – |
| HBV | 5 (7.2) | 7 (8.4) | 0.84: 0.25–2.80 | – | – | – |
| Previous TB contact | 10 (14.5) | 5 (6) | 2.64: 0.86–8.15 | – | 0.47: 0.06–3.37 | – |
| Past TB | 5 (7.2) | 4 (4.8) | 1.54: 0.39–5.99 | 0.42: 0.03–5.53 | ||
| HIV transmission | ||||||
| Homosexual | 8 (11.6) | 13 (15.7) | ||||
| Heterosexual | 14 (20.2) | 32 (38.8) | ||||
| Transfusion | – | 4 (5) | – | – | ||
| Drug addiction | 35 (50.7) | 25 (30) | 2.38: 1.23–4.65a | 0.82: 0.19–3.43 | ||
| Congenital | 1 (1.4) | – | ||||
| Undeterminated | 5 (7.2) | 15 (18) | ||||
| Screening tests | ||||||
| TST | 60 (87) | |||||
| IGRA ELISPOT | 15 (21.7) | – | – | – | – | – |
| IGRA QT | 31 (45) | |||||
| Chest X-ray abnormalities | 31 (45) | 34 (40.9) | 1.18: 0.62–2.24 | – | – | – |
| Respiratory symptoms | 27 (39) | 33 (39.8) | 0.97: 0.51–1.87 | – | 2.25: 0.37–13.66 | – |
| Other symptoms | 29 (42) | 32 (38.5) | 1.16: 0.60–2.22 | – | 2.75: 0.37–20.4 | – |
| Screening decentralization (before vs after) | 69 (45) (20 vs 49) | 83 (55) (67 vs 16) | 9.57: 4.53–20.2a | 16.2: 5.25–54.7a | 0.32: 0.03–3.15 | – |
| LTBI diagnosis | 14 (20) | – | – | – | – | – |
| LTBI treatment | 10b (78.5) | – | – | – | – | – |
| Tx toxicity | 7 (50) | – | – | – | – | – |
| Tx compliance | – | – | – | – | – | |
| Good | 10b (85.7) | |||||
| Intermediate/bad | 2 (14.3) | |||||
| Active TB diagnosis | 18 (26) | 14 (16.9) | ||||
| Disseminated | 5 (5.9) | 4 (4.8) | – | – | – | – |
| Pleural | – | 2 (2.4) | ||||
| Lung | 13 (13.8) | 8 (9.6) | ||||
| Active TB Tx | 18 (21.1) | 14c (16.9) | – | – | – | – |
| Tx toxicity | 6 (33.3) | 8 (57.1) | – | – | – | – |
| Tx compliance | ||||||
| Good | 15 (83.3) | 11 (78.6) | – | – | – | – |
| Intermediate/bad | 3 (16.6) | 3 (21.4) | ||||
| HAART | 30 (43.5) | 61 (73.5) | 0.28: 0.14–0.55a | 0.71: 0.27–1.88 | 11.3: 1.13–112.5a | 11.3: 1.13–112.5a |
N°, number; %, percentage; y, years; UV, univariate analysis; MV, multivariate analysis; OR, Odd-ratio; 95% CI, 95% confidence interval; TB, tuberculosis; LTBI, latent tuberculosis infection; HIV, human immunodeficiency virus; AIDS, acquired immunodeficiency syndrome; HCV, Hepatitis C virus; HBV, Hepatitis B virus; TST, tuberculin skin test; IGRA, interferon-gamma-release-assay; QT, quantiferon-TB; Tx, treatment; HAART, Highly-Active-Antiretroviral-Therapy.
In the period studied, 69 (45.4%) of the HIV patients had TB screening. Before decentralization, 78 HIV patients were seen and 20 (25%) accepted screening. After decentralization, 49 of the 64 HIV patients (76.6%) accepted screening. Decentralization (p<0.001), longer period of HIV infection (p=0.04), drug-use (p=0.008), HCV (p=0.003) and higher CD4 count (p=0.012) were related with screening acceptance. AIDS defining disease (p=0.001), Highly-Active-Antiretroviral-Therapy (HAART) (p<0.001) and age increase (p=0.01) were negatively correlated. In multivariate analysis only decentralization was associated with acceptance (p<0.001), while having AIDS defining illness (p=0.002) and increasing ages (p=0.04) were associated with non-acceptance (Table 1).
LTBI was diagnosed in 14 patients and active-TB in 32; screening diagnosed 18 cases of active-TB (26%); 14 cases of active-TB were diagnosed later during hospital appointments – 7 had been screened and 1 had LTBI (abandoned preventive treatment).
Treatment analysisTreatment for TB and LTBI was offered to all identified patients – 10 LTBI and all active-TB patients completed treatment. In 2 cases, IPT was not completed because of hepatotoxicity. 36 patients (83.7%) had good treatment adherence, representing 10 from 12 cases with LTBI and 26 from 32 cases of active-TB (Table 1). Analyzing treatment compliance by multivariate logistic regression, no associated factor in LTBI patients was found. In active-TB, being on HAART was related with good treatment adherence (p=0.03) (Table 1).
DiscussionIn our population, improving health care access was important for compliance to screening. The advantages of doing the screening in the outpatient clinic were – tests and clinical consultation did not require previous appointment and the clinic was very easy to get to (bus, subway, trains were nearby). Like the hospital, all exams and clinical appointments were free of charge.
The TB outpatient clinic had rigorous TB control measures and active-TB patients were hospitalized or the nurse administrated medication under observation in their homes, until micobacteriological sputum negativation. Likewise, whenever active-TB or LTBI was diagnosed, combined treatment was offered, wherever the patient chose to do it.
Until recently, National Directorate of Health covered the costs of transportation for TB patients to TB clinics for medication or clinical appointments. This support has since been withdrawn. Health care access will be more difficult – decentralization can help to deal with this. Other studies have pointed out the importance of collaboration across services and a client-centred approach.3 Decentralization of care has been identified as a strength in case detection and retention in care among HIV patients.4
In our study, being on HAART was related with better compliance to active-TB treatment. When TB patients were on HAART combined therapy was always provided.
HAART was also associated with non-acceptance to screening in our population. Patients on HAART could have a “false” safety sensation related with therapy and increased CD4 count, which could explain their poor screening adherence in the absence of symptoms. The associations found in patients on HAART indirectly confirm that these issues are complex and multifactorial.
Although our study had the weakness of a small cohort of patients, analyzing together TB screening and treatment adherence suggests that improving health care access was determinant in screening compliance and it reinforces the need for further research and randomized prospective clinical trials to determine the most effective manner in order to deal with this risk population. Knowledge about factors associated with screening and treatment adherence is important to improve strategies aiming to enhance cure and prevent dissemination of TB.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Viveiros F, Adesão ao rastreio e tratamento da tuberculose em doentes infetados com VIH. Revista Portuguesa de Pneumologia. 2013. http://dx.doi.org/10.1016/j.rppneu.2013.03.001.


