



to synthesize the Italian epidemiological contribution to knowledge on indoor pollution respiratory impact, and to analyze the perspective of some GARD countries on the health effects of indoor air pollution.
ResultsItalian epidemiological analytical studies confirmed a strong relationship between indoor air pollution and health in general population. Environmental tobacco smoke, biomass (wood/coal) fuel for cooking/heating and indoor allergens (house dust mites, cat and dog dander, mold/damp) are the most relevant indoor pollution sources and are related to respiratory and allergic symptoms/diseases in Italy and in other GARD countries such as Mexico, Brazil, Vietnam, India, Nepal and Kyrgyzstan.
Community-based global health collaborations are working to improve prevention, diagnosis and care of respiratory diseases around the world, specially in low- and middle-income countries, through research and education.
Conclusionsin the last thirty years, the scientific evidence produced on respiratory health effects of indoor air pollution has been extensive, but the necessity to empower the synergies between scientific community and local administrations remains a challenge to address in order to implement effective interventions.
Based on abundant evidence of indoor pollution health effect, WHO, scientific societies, patient organizations and other members of the health community should work together to pursue the GARD vision of “a world where all people breathe freely” and encourage policy makers to increase their engagement in advocacy for clean air.
Chronic respiratory diseases (CRDs) are among the most common non-communicable diseases worldwide. CRDs include chronic obstructive pulmonary disease (COPD), asthma, occupational lung diseases and pulmonary hypertension. The World Health Organization (WHO) Global Alliance against CRDs (GARD) vision is “a world in which all people breathe freely” and the aim of the WHO CRDs Programme is to support Member States, specially in low- and middle-income countries (LMICs), for reducing the toll of morbidity, disability and premature mortality of CRDs, specifically asthma and COPD.1
Household air pollution (HAP) ranks 9th out of 69 risk factors linked to attributable deaths included in the Global Burden of Disease (GBD) project. HAP, caused by incomplete combustion of solid fuels and kerosene used for cooking/heating, was responsible for 3.2 million premature deaths in 2020 (over 237,000 in under 5 year-old children): 21% due to lower respiratory infections (LRI), 19% to COPD and 6% to lung cancer. HAP accounted for the loss of an estimated 86 million healthy life years in 2019, with the largest burden for women living in LMICs. Almost half of deaths due to LRI among under 5 year-old children are caused by PM (soot) from HAP.2 Most deaths occur in three GBD Super Regions: South Asia (36%), sub-Saharan Africa (30%), and Southeast Asia, East Asia, and Oceania (28%).3
This paper is the fourth of the Series on “Air pollution and health”4–6 and is strictly linked to the companion paper on indoor pollution. 7
MethodsThere are two main sections, an Italian perspective and the perspectives from other GARD countries: the first summarizes results of the role of various indoor air pollutants on CRD-related outcomes in different Italian epidemiological studies; the second includes main results obtained in other GARD countries.
In Italy, epidemiological surveys on general population samples and school-children and adolescents were designed and conducted by the National Research Council (CNR), individually or in collaboration with other research groups, since the late 1970s. Health effects (e.g. allergic and respiratory symptoms/diseases, lung function tests, serum immunoglobulin E (IgE), exhaled nitric oxide (FeNO)) of indoor air pollution in general population (adult and children) were assessed.8–21
In particular, the Italian main results derive from the Po Delta (PD) and Pisa (PI) analytical prospective studies,12,22–28 “Italian Studies on Respiratory Disorders in Children and the Environment” (SIDRIA) study,15,29,30 “Epidemiologic study on environment and health in women” (SEASD) study,14 “Health Effects of School Environment” (HESE) study,31,32 “Geriatric study on health effects of air quality in nursing homes in Europe” (GERIE) study,18 the Palermo (PA) studies on children-adolescents,16,17 “Indoor and Outdoor Air Quality and Respiratory Health in Malta and Sicily” (RESPIRA) project19,20 and “CHildhood ASthma and Environment Research” (CHASER) study.21
The perspectives from other GARD countries concern recent results from Mexico, Brazil, Vietnam, India, Nepal and Kyrgyzstan. An update on respiratory health impact of indoor air quality was performed through a PubMed Search for the period 2000–2022, focusing questionnaire and lung function tests. In addition, a part is dedicated to the community-based global health collaborations “Free Respiratory Evaluation and Smoke-exposure reduction by primary Health cAre Integrated gRoups” (FRESH AIR), “UK National Institute for Health Research, Global Health Research Unit on Respiratory Health” (RESPIRE) and “Global Health Respiratory Network” (GHRN).
ResultsAn Italian perspectiveResults of CNR epidemiological surveys are summarized taking into account two different approaches of indoor air pollution assessment: qualitative evaluation from standardized questionnaires; quantitative evaluation (through active or passive samplers).
Indoor qualitative evaluationIn Italy (Table 1), it became clear in the early nineties that the fuel for cooking or for heating and that kind of heating are associated with increased prevalence rates of respiratory symptoms or impaired lung function. In PD males, significantly increased odds ratios (ORs) were found for: cough and dyspnea with bottled gas for cooking; cough and phlegm with stove for heating; cough with natural gas stove and fan or stove powered by other fuels.23 In females, significantly increased ORs were found only for dyspnea with bottled gas for cooking, stove for heating, natural gas stove, stove or fan powered by other fuels.23 In PI males, significantly increased ORs were shown for: cough and phlegm associated with bottled gas for cooking in males; wheeze and shortness of breath with wheeze associated with the use of a stove or forced-air circulation in females.24 In 8–19 years PD non-smokers, significantly higher prevalence rates of wheeze, dyspnea, diagnosis of asthma were found in subjects of both sexes using bottled gas for cooking and exposed to passive smoking.22
Main studies carried out by CNR about the effects of indoor air pollution on respiratory health in Italy.
| Author and year of publication | Population | Indoor setting | Exposure | Health outcome | Main results |
|---|---|---|---|---|---|
| Cooking and heating | |||||
| Viegi et al., 1991 (ref. 22) | 381 subjects (8–19 year-old) living in Po River Delta area | Home | Cooking fuel and kind of heating | Chronic cough, attacks of shortness of breath with wheeze, wheeze, dyspnea, rhinitis and asthma | Among ETS exposed subjects, use of bottled gas for cooking than natural gas significantly associated with higher prevalence rates of wheeze (8%), dyspnea (11%) and diagnosis of asthma (11%). |
| Viegi et al., 1991 (ref. 23) | 3289 subjects (8–64 year-old) living in Po River Delta area | Home | Cooking fuel and kind of heating | Chronic cough, chronic phlegm, dyspnea and lung function | In males, significant associations between:
|
| Viegi et al., 1992 (ref. 24) | 3866 subjects (5–90 year-old) living in Pisa | Home | Cooking fuel and kind of heating | Cough, phlegm, wheeze, attacks of shortness of breath with wheeze | In non-smoking males, significant association between:
|
| SHS | |||||
| Paoletti et al., 1995 (ref. 25) | 255 non-smoking subjects (8–20 year-old) living in the Po River Delta area | Home | SHS | Cough, phlegm, wheeze, attacks of shortness of breath with wheeze, asthma | In SHS exposed subjects than unexposed, significantly higher prevalence rates of cough (7.5%) and phlegm (5.9%). |
| Simoni et al., 2001 (ref. 26) | 867 non-smoking women (8–73 year-old) | Home, school/work or elsewhere | SHS | Asthma (symptoms/diagnosis) | In non-smoking woman, SHS exposure vs no SHS exposure significantly associated with asthma (OR 1.90; 95% CI 1.1–3.4) |
| Simoni et al., 2003 (ref. 28) | 120 elderly subjects (≥65 year-old) living in Pisa and Po River Delta area | Home | SHS | Acute respiratory symptoms | In SHS exposed subjects than unexposed, higher occurrence of acute respiratory symptoms both in winter (31 vs 29%) and summer (33 vs 16%). |
| Simoni et al., 2007 (ref. 14) | 2195 never smoking women (mean age 47 years) living in Pisa, Po River Delta, Rome and Viterbo | Home/work | SHS to husband/partner, at workplace, in other places | Current dyspnea, anyshortness of breath at rest, recent wheeze, recent attacks of shortness of breath with wheeze,asthma diagnosis/symptoms, obstructive lung diseases (diagnosis of asthma/chronicbronchitis/ emphysema),current cough/phlegm and rhino-conjunctivitis | In women, combined SHS exposure of husband/partner and at work vs no SHS exposure significantly associated with:
|
| Cibella et al., 2011 (ref. 16) | 2150 children (10–17 year-old) living in Palermo | Home | SHS | Current asthma and rhino-conjunctivitis | PAR% for current asthma attributable to SHS = 18.1%.PAR% for rhino-conjunctivitis attributable to SHS = 18.8%. |
| Ciluffo et al., 2022 (ref. 21) | 179 asthmatic children (5–16 year-old) living in Palermo | Home | SHS | Uncontrolled asthma | In children, SHS exposure during pregnancy vs no SHS exposure during pregnancy associated with higher risk of uncontrolled asthma later in life (OR 3.82; 95% CI 1.11–13.06). |
| Particulate matter, nitrogen dioxide, formaldehyde and carbon dioxide | |||||
| Simoni et al., 2002 (ref. 27) | 383 subjects (15–72 year-old) living in the Po River Delta | Home | NO2-index* (high: > median value) and PM2.5-index* (high: > median value) | Acute respiratory illnesses with fever, chronic bronchitis and/or asthmatic symptoms without fever, irritation without fever | In winter, on the whole sample significant associations between:
|
| Simoni et al., 2003 (ref. 28) | 120 elderly subjects (≥65 year-old) living in Pisa and Po River Delta area | Home | PM2.5-index* (high: > median value) | Acute respiratory symptoms | High PM2.5-index exposure (vs low) associated with acute respiratory symptoms:
|
| Simoni et al., 2004 (ref. 12) | 1090 subjects (≥15 year-old) living in Pisa and Po River Delta area | Home | NO2-index* (high: > median value) and PM2.5-index* (high: > median value) | Acute respiratory illness, bronchitic and/or asthmatic symptoms without fever and without acute respiratory illness, increased PEF maximum amplitude, increased PEF diurnal variation | On the whole sample significant associations between:
|
| Simoni et al., 2010 (ref. 31) | 654 children (10 year-old) living in five European countries (Siena and Udine, Italy; Reims, France; Oslo, Norway; Uppsala, Sweden; Århus, Denmark). | School | PM10 and CO2 | Wheezing, dry cough at night, rhinitis and nasal patency | Schoolchildren exposed to elevated CO2 levels (>1000 ppm) (vs low) showed a higher risk for:
|
| Cibella et al., 2015 (ref. 17) | 303 children (10–17 year-old) living in Palermo | Home | NO2 (high: >28 µg/m3 in spring; > 41.4 µg/m3 in winter) | Current asthma, wheeze, chronic phlegm and rhino-conjunctivitis | Children with current asthma were significantly more exposed to high level of indoor NO2 than low level (89% vs 11%); the same for children with wheeze episodes in the last 12 months (78% vs 22%), chronic phlegm (82% vs 18%), and rhino-conjunctivitis (66% vs 44%). |
| Bentayeb et al., 2015 (ref. 18) | 600 elderly subjects (>65 year-old) living in seven European countries (Uppsala, Sweden; Warsaw, Poland; Athens, Greece; Reims, France; Arezzo, Italy; Århus, Denmark; Brussels, Belgium) | Nursing home | PM10, PM0.1, formaldehyde, nitrogen, NO2 and CO2 (high: >median value of the distribution of each pollutant) | FEV1/FVC, breathlessness, cough, wheeze, COPD and exhaled carbon monoxide | Significant associations between:
|
| Drago et al., 2018 (ref. 20) | 73 children (10–15 year-old) living in Gela, Niscemi, Mazzarino and Butera (Sicily) | Home | PM2.5 mass concentration; fractions of Cd, Ce, La, and Tl in PM2.5+ | Asthma symptoms in the last 12 months (wheezing/whistling in the chest and chest sounded wheezy during/after exercise or dry cough at night) | Asthma symptoms in the last 12 months significantly associated with:
|
| Allergens | |||||
| Simoni et al., 2005 (ref. 29) | 20,016 children (6–7 year-old) and 13,266 adolescents (13–14 year-old) living in five areas of northern Italy (Turin, Milan, Mantua, Trent, and Emilia- Romagna), five areas of central Italy (Rome, Florence, Empoli, Siena, and Colleferro), and two areas of the south (Bari, Palermo). | Home | Moulds, dog and cat danders | Wheeze, asthma and cough/chronic phlegm | In children, compared with no allergen exposure, significant associations between:
|
| Simoni et al., 2005 (ref. 30) | 20,016 children (5–11 year-old) and 13,266 adolescents (12–17 year-old) living in five areas of northern Italy (Turin, Milan, Mantua, Trent, and Emilia-Romagna), five areas of central Italy (Rome, Florence, Empoli, Siena, and Colleferro), and two areas of the south (Bari, Palermo). | Home | Moulds/dampness | Asthma, rhino-conjunctivitis, wheeze and persistent cough/phlegm | In children, compared with no allergen exposure, significant associations between:
|
| Lombardi et al., 2010 (ref. 15) | 20,016 children (6–7 year-old) living in five areas of Northern Italy (Turin, Milan, Mantua, Trent, Emilia-Romagna), four areas of Central Italy (Florence, Empoli, Siena, Colleferro) and two areas of Southern Italy (Bari, Palermo) | Home | Cat and dog danders | Current wheezing, current asthma and current rhino-conjunctivitis | Compared with no allergen exposure, significant associations between:
|
| Simoni et al., 2011 (ref. 32) | 654 children (10 year-old) living in five European countries (Siena and Udine, Italy; Reims, France; Oslo, Norway; Uppsala, Sweden; Århus, Denmark). | School | Moulds (colony-forming units, cfu/m3) and fungal DNA (cell equivalents, CE/g dust) | Past year dry cough at night, persistent cough, rhinitis, FEV1 and FVC | Children exposed to elevated viable mould levels (≥ 300 cfu/m3) (vs low) showed higher risk of:a)past year dry cough at night (OR 3.10; 95% CI 1.61–5.98);b)persistent cough (OR 3.79; 95% CI 2.40–5.60);c)rhinitis (OR 2.86; 95% CI 1.65–4.95). 104 CE/g dust increase of Aspergillus/Penicillium DNA was associated with wheeze (OR 2.14; 95% CI 1.05–4.36).100 CE/g dust increase of Aspergillus versicolor DNA was associated with:a)wheeze (OR 1.48; 95% CI 0.99–2.21);b)cough (OR 1.75; 95% CI 1.17–2.62);c)rhinitis (OR 1.75; 95% CI 1.18–2.60).There were inverse associations of Aspergillus versicolor DNA with FVC (B −0.12; 95% CI −0.24–0.02) and Streptomyces DNA with both FEV1 (B −0.14; 95% CI −0.22-(−0.05)) and FVC (B −0.13; 95% CI −0.23-(−0.04)) |
| Cibella et al., 2011 (ref. 16) | 2150 children (10–17 year-old) living in Palermo | Home | Moulds /dampness, Dermatophagoides mix, dog dander and cat dander | Current asthma and rhino-conjunctivitis | PAR% for current asthma attributable to:
|
| Ruggeri et al., 2017 (ref. 19) | 125 children (10–14 year-old) living in a Southern Mediterranean (Sicily and Malta) | Home | Der p 1 | Wheeze in the last 12 months, Der p 1-specific IgE level and FeNO | Der p 1 was positively correlated with both high Der p 1-specific IgE and FeNO in children with last 12 months wheeze. |
OR: odds ratio.
95% CI: 95% confidence interval.
SHS: secondhand smoke.
NO2: nitrogen dioxide.
RSP: Respirable Suspended Particulate Matter.
PM10: particulate matter < 10 µm.
PM2.5: particulate matter ≤ 2.5 µm.
PM0.1: particulate matter <0.1 µm.
CO2: carbon dioxide.
FEV1: forced expiratory volume in one second.
FEF25–75: forced mid-expiratory flow.
MEF50: maximal expiratory flow at 50%.
PEF: peak flow.
eNO: exhaled Nitric Oxide.
PAR%: Population attributable risk, expressed as percent.
Der p 1: the major allergen of Dermatophagoides pteronyssinus.
FeNO: exhaled nitric oxide.
Cd: Cadmium.
Ce: Cerium.
La: Lanthanum.
Tl: Thallium.
IgE: Immunoglobulin E.
* NO2-IndEx and PM2.5-IndEx: daily indices of exposure to NO2 and to PM2.5 computed as the product of weekly mean concentration of pollutant and the daily time of exposure (i.e. the time spent at home).
The importance of secondhand smoke (SHS) exposure as a risk factor for respiratory diseases was also pointed out. Higher occurrence of cough and phlegm in young non-smokers and of acute respiratory symptoms in the elderly exposed to SHS were shown in PD and PI studies.25,28 In 867 PD non-smoking women, SHS was a significant risk factor for asthma.26 In 2195 non-smoking women, living in PI, PD, Rome and Viterbo, SHS exposure both to husband/partner and at work was a significant risk factor for dyspnea, cough/phlegm and rhino-conjunctivitis, any shortness of breath at rest, wheeze and attacks of shortness of breath with wheeze, asthma diagnosis/symptoms, obstructive lung diseases (diagnosis of asthma/chronic bronchitis/emphysema).14 In 2150 PA schoolchildren, SHS was responsible for 18.1% of current asthma and 18.8% of rhino-conjunctivitis.16 Passive smoking exposure during pregnancy was related to a higher risk of uncontrolled asthma in a recent cohort study on PA asthmatic children.21
In the SIDRIA-2 study, carried out in 2002 in 12 areas of northern, central and southern Italy, mold exposure in the first year of life was positively associated with wheezing, asthma and rhino-conjunctivitis in children and adolescents, and with cough/phlegm only among children. Mould exposure in the previous year was a significant risk factor for wheeze, among children, and wheeze was most strongly related to early and current mould/dampness exposure; the same occurred in adolescents for rhino-conjunctivitis.29,30 In 2150 PA children, mould/dampness exposure was responsible of about 7% of current asthma and rhino-conjunctivitis cases.16
In the SIDRIA-2 study, dog exposure in the first year of life increased the risk for wheezing in children and for cough/phlegm in both children and adolescents. Lifetime dog exposure was significantly related to cough/phlegm in adolescents. Finally, cat exposure in the first year of life was significantly associated with current wheezing, asthma and rhino-conjunctivitis in children.15,29 In PA children, cat and dog exposures were responsible of 7.2% and 5.3% of current asthma cases, and of 1.4% and 1.0% of rhino-conjunctivitis cases, respectively.16
Indoor quantitative evaluationIn Italy (Table 1), the direct measurements of particulate matter < 2.5 µm (PM2.5) and nitrogen dioxide (NO2) were carried out in 140 PD households during winter and summer. The concentration of monitored pollutants was larger in winter than in summer. Significantly higher indoor NO2 levels were found in the houses with gas-furnace heating and/or with gas water heater located inside the home. PM2.5 was significantly higher in smokers’ homes, and significantly related to the number of cigarettes smoked.33 Only in winter, there were significant associations of bronchitic/asthmatic symptoms with NO2 and PM2.5 values above the median. In summer, this association emerged for PM2.5 only in non-smokers.27 Moreover, in PD and PI adults, NO2 and PM2.5 exposures were associated with acute respiratory symptoms and mild lung function impairment.12 In an elderly sample, the occurrence of acute respiratory symptoms was consistently higher in relation to the high respirable suspended PM (RSP) exposure, compared to low exposure.28
In the GERIE study, for the first time, the relationships between indoor air quality, comfort parameters and respiratory morbidity among European elderly people living in nursing homes were investigated. The following associations were found: particulate matter <0.1 µm (PM0.1) with forced expiratory volume in one second (FEV1)/ forced vitality capacity (FVC) <70% and wheeze; PM10 and CO2 with breathlessness and cough; NO2 with FEV1/FVC<70%, breathlessness and cough; formaldehyde with COPD and exhaled carbon monoxide. Pollutant effects were more pronounced in the case of poor ventilation.18
In the HESE study, schoolchildren exposed to CO2 levels >1000 ppm showed a higher risk for dry cough and rhinitis; nasal patency was significantly lower in those exposed to PM10 >50 µg·m−3.31
PA adolescents, exposed to the highest indoor NO2 concentrations, had increased frequency of current asthma, wheezing in the last 12 months, chronic phlegm, and rhino-conjunctivitis.17
In the RESPIRA project, assessment of respiratory health, determination of PM elemental composition and of selective markers of smoking were performed in 73 houses of adolescents living in Sicily (Gela, Niscemi, Mazzarino and Butera). When corrected for confounding factors, PM2.5, Cadmium (Cd), Cerium (Ce), Lanthanum (La) and Thallium (Tl) were associated with increased probability of having respiratory symptoms.20 Further, Dermatophagoides pteronyssinus (Der p 1) was positively correlated to both high Der p 1-specific IgE and Fractional exhaled nitric oxide (FeNO) in children with last 12 months wheeze.19
In the HESE study, an elevated concentration of moulds (≥300 cfu/m3) in the classroom was associated with higher risk of dry cough at night, persistent cough and rhinitis in the last 12 months. Aspergillus/Penicillium DNA was associated with wheeze, and Aspergillus versicolor DNA with wheeze, rhinitis and cough; there were inverse associations of Aspergillus versicolor DNA with FVC and Streptomyces DNA with both FEV1 and FVC.32
The perspectives from other GARD countriesA Mexican perspectiveIn Mexico (Table 2), 9–12 year-old children spend 85% of their time indoors.34 Airborne pollen, indoor and outdoor pollutants may influence sick building syndrome (SBS).35 In a study carried out in Monterrey (Nuevo Leon) 91% of subjects reported at least 1 SBS symptom, and fatigue was the most frequent (74.6%). Quercus and Fraxinus pollen were related with headaches, while humidity and NOx were associated with eye and nasal symptoms.35
Main studies about the effects of indoor air pollution on respiratory health in some GARD countries.
| Author and year of publication | Country | Population | Exposure | Health outcome | Main results |
|---|---|---|---|---|---|
| Cooking and heating | |||||
| Melsom et al., 2001 (ref. 76) | Nepal | 121 schoolchildren (11–17 year-old) | Open fire or burning stove without a flue | Asthma | The risk of asthma was higher among children exposed to smoky fuels (defined as living in a house with an open fire or burning stove without a flue) than for those not exposed (OR 2.2; 95% CI 1.0- 4.5). |
| Regolado et al., 2006 (ref. 37) | Mexico | 841 non-smoking women (≥38 year-old) | Cooking fuel | Phlegm, cough, wheezing and FEV1/FVC | Among non-smoking women, use of biomass for cooking than natural gas significantly associated with higher prevalence rates of:
|
| Johnson et al., 2011 (ref. 66) | India | 900 non-smoking women (≥30 year-old) | Biomass fuel | COPD | COPD prevalence was higher in biomass fuel users (vs clean fuel users) (OR 1.24; 95% CI 0.36–6.64) |
| da Silva et al., 2012 (ref. 48) | Brazil | 1402 individuals | Indoor-Biomass and Outside-Biomass | Cough, wheezing and dyspnea | In adults (≥20 year-old), significant associations between:
|
| Agrawal et al., 2012 (ref. 67) | India | 156,316 subjects (20–49 year-old) | Cooking fuel | Asthma | In adult women, biomass and solid fuels (vs cleaner fuels) were associated with asthma (OR 1.26; 95% CI 1.06–1.49). |
| Kurmi et al., 2013 (ref. 72) | Nepal | 1648 individuals (≥ 16 year-old) | Biomass smoke | FEV1/FVC | Airflow obstruction (defined as FEV1/FVC below the lower limit of normal) was significantly higher in subject exposed to the domestic biomass burning compared with those using liquid petroleum gas fuel (OR 2.06; 95% CI 1.16–3.67). |
| Bhat et al., 2013 (ref. 69) | India | 214 children (<5 year-old) | Cooking fuel | ALRTI | Cooking fuel other than liquid petroleum gas (vs liquid petroleum gas) was associated with ALRTI (OR 3.58; 95% CI 1.23–10.45). |
| Acharya et al., 2015 (ref. 71) | Nepal | 4802 children (<5 year-old) | Solid fuel | ARI | The risk of developing ARI was higher among children from the households using solid fuel in comparison with the children from households using cleaner fuel (OR 1.79; 95% CI 1.02–3.14). |
| Sinha et al., 2017 (ref. 73) | India | 1200 adults (≥ 30 year-old) | Biomass fuel | COPD | Biomass fuel use resulted strongly associated with COPD (AOR 2.64; 95% CI 1.48–4.71) |
| Svendsen et al., 2018 (ref. 36) | Mexico | 5210 children (9–11 year-old) | Fireplace heat, central air conditioning, humidifier use and cooking with gas stoves | Allergy and asthma | Allergy prevalence:
|
| Ramírez-Venegas et al., 2018 (ref. 38) | Mexico | 1333 women (>35 year-old) | Biomass smoke | Cough, phlegm, wheezing, dyspnea, FEV1, FVC, FEV1/FVC and SaO2 | The prevalence of respiratory symptoms was significantly higher in women with biomass smoke exposure compared with those without exposure:
|
| Fernandes et al., 2018 (ref. 46) | Brazil | 996 subjects (≥18 year-old) | Biomass smoke | Asthma | In individuals with asthma, exposure to smoke from wood stoves vs no exposure significantly associated with:
|
| Naz et al., 2018 (ref. 70) | Nepal | 17,780 children (<5 year-old) | Cooking fuel | Mortality | The use of cooking fuel was associated with total under-five mortality (OR 2.19; 95% CI 1.37–3.51), with stronger associations evident for sub-group analyses of neonatal mortality (OR 2.67; 95% CI 1.47–4.82) |
| Baggio et al., 2019 (ref. 44) | Brazil | 22,485 individuals (>18 year-old) | Solid fuels | Bronchitis/asthma | In women, solid fuels vs clean fuels associated with higher risk of bronchitis/asthma (OR:1.43). |
| Brakema et al., 2019 (ref. 81) | Kyrgyzstan | 392 individuals (>18 year-old) | PM2.5 | COPD | The highest PM2.5 exposure (vs the lowest exposure) associated with COPD (OR 3.17, 95% CI 1.01–9.49). |
| Rao et al., 2022 (ref. 68) | India | 4662 individuals (>30 year-old) | Biomass fuel (wood, dung, crop) and mosquito coil | Poor respiratory health | Poor respiratory health was associated with:
|
| SHS | |||||
| Melsom et al., 2001 (ref. 76) | Nepal | 121 schoolchildren (11–17 year-old) | SHS | Asthma | Asthma was associated with cigarette smoking by two or more family members (OR 1.9; 95% CI 1.0–3.9). |
| Gupta et al., 2006 (ref. 75) | India | 62,109 adults | SHS | Asthma | Asthma was associated with:
|
| Dahal et al., 2009 (ref. 77) | Nepal | 6056 children (<5 year-old) | SHS | ARI | The risk of ARI symptoms was higher among children born to mothers who smoked more frequently than their counterparts (AOR 1.41; 95% CI 1.02–1.96). |
| Schvartsman et al., 2013 (ref. 53) | Brazil | 105 children (6–23 months-old) | SHS | Wheezing | On the whole sample significant associations between:
|
| Fernández-Plata et al., 2016 (ref. 39) | Mexico | 3187 schoolchildren (8–17 year-old) | SHS | Respiratory symptoms (cough, wheezing, phlegm and dyspnea), respiratory infections (common cold, sore throat and bronchitis), FEV1 and FVC | OR of between 1.4 and 2.3 predicting respiratory symptoms in those exposed to passive smoking, exhibiting a trend to increase with the number of persons smoking inside the home; for recent respiratory infections, OR were between 1.2 and 1.5.Levels of FEV1 and FVC in individuals exposed to passive smoking were 6.8 and 14.1 ml, respectively, below those of non-exposed children. |
| Freire et al., 2016 (ref. 52) | Brazil | 120 subjects (30–50 year-old) | SHS | FEV1 | FEV1% predicted was significantly lower in the passive smoking group when compared with the control group (93.41 ± 14.90 vs 101.9 ± 9.81). |
| Fernandes et al., 2018 (ref. 54) | Brazil | 375 adolescents (13-14 year-old) | SHS | Wheezing | Wheezing was associated with more than 20 cigarettes per day smoked by parents or other household members (OR 3.6; 95% IC 1.2–10.7). |
| Thapa et al., 2016 (ref. 78) | Nepal | 198 children (<5 year-old) | SHS | ARI | ARI was associated with:
|
| Schivinski et al., 2017 (ref. 51) | Brazil | 78 schoolchildren (6–14 year-old) | SHS | PEF | In SHS exposed children there was lower PEF (4.194 L/s ± 1.278 vs 5.064 L/s ± 1.604) than in those unexposed. |
| Sinha et al., 2017 (ref. 73) | India | 1200 adults (≥ 30 year-old) | SHS | COPD | The risk of COPD was higher among subjects exposed to SHS than for those not exposed (AOR 7.9; 95% CI 3.32–13.18). |
| Rivera et al., 2021 (ref. 40) | Mexico | 536 children (6–8 year-old) | SHS and PM2.5 | Wheeze | Among children born to mothers exposed to SHS in pregnancy when compared with unexposed mothers, significant association between higher prenatal and early life PM2.5 exposure and higher cumulative risk ratios of:
|
| Allergens | |||||
| Lâm et al., 2014 (ref. 62) | Vietnam | 684 subjects (23–72 year-old) | Any mite, cockroach, any animal and to any allergen | AR | AR were strongly associated with sensitisation to:
|
| Álvarez-Chávez et al., 2016 (ref. 41) | Mexico | 18 sensitized children (3–6 year-old) | Dust | Specific sensitivity (IgE) to Dermatophagoides pteronyssunus | Significant association found was between the presence of dust and sensitivity with the allergen Dermatophagoides pteronyssunus (dust mite) (Kappa value: 0.44; p = 0.01). |
| Fernandes et al., 2018 (ref. 54) | Brazil | 375 adolescents (13–14 year-old) | Pets | Wheezing | Contact with animals in the first year of life (dogs, cats, other furry animals, or birds) was associated with wheezing (OR 3.2; 95% IC 1.1–8.8). |
| Svendsen et al., 2018 (ref. 36) | Mexico | 5210 children (9–11 year-old) | Ant, spider and dog | Allergy and asthma | Allergy prevalence:
|
| Segura-Medina et al., 2019 (ref. 42) | Mexico | 42 patients with asthma (18–76 year-old) | Muolds | ACT, FEV1 and FVC | Concentrations of some moulds were negatively associated with parameters of asthma control in male subjects, but not in female patients; significant Spearman correlation coefficient in male were:
|
| Neto et al., 2019 (ref. 55) | Brazil | 878 children (9–12 year-old) | Cat | Asthma | Having a cat during the first year of life was a risk factor associated with asthma (OR 1.73; 95% IC 1.07–2.78). |
| Deka et al., 2022 (ref. 74) | India | 150 patients (3–12 year-old) | Pets and dampness | Asthma | Compared with no allergen exposure, significant associations between:
|
FEV1: forced expiratory volume in the first second.
FVC: forced vital capacity.
ALRTI: acute lower respiratory tract infections.
ARI: acute respiratory tract infections.
COPD: chronic obstructive pulmonary disease.
AOR: adjusted odds ratio.
SaO2: oxygen saturation.
mMRC: Modified Medical Research Council Dyspnea Scale.
OR: odds ratio.
95% CI: 95% confidence interval.
SHS: secondhand smoke.
PM2.5: particulate matter ≤ 2.5 µm.
RR: cumulative risk ratios.
ACT: Asthma Control Test.
AR: allergic rhinitis.
PEF: peak flow.
Poor respiratory health: (i) individual with symptoms of chronic bronchitis, namely cough with expectoration for three or more months; for two or more years (ii) wheezing or chest tightness/breathlessness in the morning and positive response to either of the three questions; previous diagnosis of asthma, use of medication for asthma or history of attack of asthma in the previous 12 months that made the respondent feel short of breath.
In 5210 elementary schoolchildren of the El Paso Independent School District, ant and spider pest problems within the past year, pet dogs, fireplace heat, central air conditioning, humidifier use, and cooking with gas stoves were positively associated with both allergy and asthma prevalence (ever and current). Lung function decreased among children who lived in homes with reported cockroach pest problem in the past year without concurrent use of pesticides.36
In 841 non-smoking ≥35 year-old women in the village of Solis (near Mexico City), compared with those cooking with gas, current use of a stove burning biomass fuel was associated with increased reporting of phlegm and reduced FEV1/FVC.37 In >35 year-old females in a suburban area of Mexico City, spirometry and oxygen saturation values were significantly lower with higher biomass exposure levels. Cough, phlegm, wheezing and dyspnea were significantly more frequent in women exposed to biomass.38
In 8–17 year-old schoolchildren from Mexico City and its metropolitan area (n = 3187), passive smoking was associated with a higher frequency of self-reported respiratory symptoms and respiratory infections. Levels of FEV1 and FVC in children exposed to passive smoking were reduced: such values decreased with increasing number of smokers at home and higher outdoor ozone levels.39 A study which involved 536 mother-child couples showed significant associations of higher prenatal and early life PM2.5 exposure with higher cumulative risk ratios of ever wheeze and current wheeze in the past year only among 6–8 year-old children born to mothers exposed to SHS in pregnancy.40
A significant association between dust and sensitivity to dust mite was found in homes of sensitized children in Hermosillo (Sonora).41 In 42 adult asthma patients in Mexico City, mould burden was negatively associated with parameters of asthma control only in males.42
Identification and quantification of persistent indoor organic pollutants were carried out in winter within three bus lines of Leon (Guanajuato) in order to determine their possible origin, the differences in the levels of contamination between routes, and the potential risk to the health of the users. Xylenes were the most representative organic pollutants with the potential to generate a higher risk to bus-users’ health (hazard quotient: 6.4–9.8), without dismissing the potential danger of other pollutants.43
A Brazilian perspectiveIn Brazil (Table 2), wood smoke is a major source of indoor air pollution, mainly among non-affluent people in rural areas.44 In Bahia state, childhood exposure to indoor wood smoke was reported by 84% adult rural-born asthmatics vs only 27% urban-born subjects;45 1.7% of asthmatic urban dwellers reported current use of wood stoves for cooking.46 In the north and northeast region, residential wood burning was significantly associated with higher risk of bronchitis/asthma only in women.44 The PURE study, a multinational 10 year cohort study on subjects from 22 urban communities and 42 rural areas, showed that Brazilians using solid fuel for cooking had higher cardiorespiratory mortality rate, compared to users of electric or gas stoves.47 In 1402 subjects living in Joao Camara, significantly increased ORs for cough, wheezing and dyspnea emerged in adults exposed to indoor stove and outside bonfire, compared to liquefied petroleum gas. Both non-smokers exposed to biomass and smokers exposed to gas had decreased %predicted-FEV1 and FEV1/FVC, as compared to non-smokers exposed to gas.48
Policies increasing access to clean fuel strongly reduced the utilization of wood fire during the last five decades.49 However, the interruption of the exposure does not avoid completely its late effects on respiratory health: in fact, previous exposure to indoor wood smoke predicts later uncontrolled asthma symptoms and lung function impairment in subjects no longer exposed, in comparison to never exposed ones.46
Tobacco-free policy contributed to the decreasing prevalence of smoking during the last few decades, but second-hand smoking remains an important source of indoor air pollution.50 It is associated with central and peripheral airway obstruction in children and adolescents.51 In adults, passive smoking is associated with impaired mucociliary clearance: exposure load correlates with worse hemodynamic parameters, reduced lung function and autonomic nervous system dysfunction.52 The probability of wheezing increased with the number of cigarettes smoked indoors in 105 children (6–23 months of age).53
In 375 Belo Horizonte adolescents, asthma symptoms were related to contact with animals during the first year of life and over 20 cigarettes per day smoked by parents or other household members.54 In 878 9–12 year-old children in Passo Fundo (Rio Grande do Sul), having an indoor cat during the first year of life was associated with asthma.55
PM is another source of indoor air pollution in large urban centers. In 2018, a strong correlation between indoor and outdoor concentrations of PM10 and PM2.5 in a nursing home in São Paulo City over thirty days of sequential sampling was observed.56 During the sampling period, indoor PM concentration exceeded the 2005 WHO guidelines.56 In the same year, high indoor concentrations of fine PM were observed in most studied residences in São Paulo metropolitan area, with indoor PM2.5 exceeding WHO recommendations in 43% of the residences; the highest values occurred in houses near heavy traffic areas during non-precipitating days.57 However, recent studies relating indoor concentration of PM and respiratory health are lacking.
A Vietnamese perspectiveIn Vietnam (Table 2), > 64% people live in rural areas with less accessibility to cleaner fuels. Energy Information Administration reported that about 25% of the total Vietnam's energy consumption was from solid biomass fuels and wastes: nearly 60% of biomass was consumed by households, mainly in rural areas.58
SHS is an important source of HAP: male smoker prevalence is very high (45.3%).
Despite the public places’ bans, SHS prevalence among adults ≥15 years remained high (89.1% in Bars/Cafes/Tea shops and 80.7% in restaurants, 37.9% in government offices, and 30.9% in universities).59
House ventilation is poor, especially in crowded city. People live very close to roadways and busy streets, which leads to increase PM and NO2 inside the houses. Recent studies, measuring outdoor and indoor air quality in Hanoi, were focused on particle number and particle mass concentrations, which showed the influence of traffic and construction activities in both outdoor and indoor environment.60,61
In South-East Asia, high temperature and humidity are an ideal habitat for mites and cockroaches.62,63 In Vietnam, the humidity and dampness are high, especially in Red River and Mekong delta.
Thus, moulds, bacteria, insects and mites grow rapidly and are linked to asthma, chronic rhinosinusitis, hypersensitivity pneumonitis and exacerbations of underlying respiratory diseases.64
In urban and rural environments, there are many allergens from house dust mites, cockroaches, and mouse infestations, contributing to respiratory diseases such as wheeze, asthma attacks, asthma, and allergic rhinitis, as emerged in 864 adults living in northern Vietnam.62
Many domestic behaviors and practices are associated with increased HAP: incense burning, poor ventilation and keeping moto-bikes in small houses, high concentrations of CO2 and volatile organic compounds (VOCs).
To reduce HAP in rural areas, use of cleaner biomass burning stoves, chimney for kitchen and gas to replace biomass fuels were incentivized. However, traditional way of cooking is still mostly used in remote areas.
In urban regions, better ventilation and use of air cleaners were encouraged, but the problem of residential overcrowding is very difficult to solve. Reducing the prevalence of smoking is a major goal, but it is time consuming.
The Projet Interuniversitaire Cible (PIC), between universities of Vietnam and Belgium from the year 2014 to 2023 aiming at reducing HAP, is being carried out with some preliminary positive results.65
A perspective from India and NepalIn a study conducted among 900 ≥ 30 year-old non-smoking women, from 45 rural villages of Tiruvallur district (Tamil Nadu, India) (Table 2), COPD prevalence was higher in biomass fuel users than in clean fuel users.66 The same association emerged for asthma in women within a nationwide large-scale cross-sectional survey on 156,316 subjects aged 20–49 years.67 In a survey on ≥35 year-old adults in 5 villages of Tiruvallur district, combined use of all three biomass fuel types (wood, dung and crop) and use of mosquito coil ≥5 days per week were associated with poor respiratory health.68 In 214 <5 year-old Indian children, cooking fuel other than liquid petroleum gas was found to be significant risk factors for acute LRI.69 From 2001 to 2011, use of cooking fuel was associated with total mortality in <5 years children from Nepal, with stronger associations evident for ≤28 days infants mortality.70 Associations were found also with acute respiratory tract infections (ARI).71
In a Nepalese population sample, prevalence of airflow obstruction was significantly higher in subject exposed to the domestic biomass burning, compared with those using liquid petroleum gas fuel.72 In 1200 ≥ 30 year-old adults in Mehrauli, a large urban community in South Delhi (India), SHS and biomass fuel use were found among the risk factors associated with COPD.73
In 150 clinically diagnosed 3–12 year-old asthmatics, damp environment, pets and passive smoking were significant risk factors for asthma.74
In a multicentric population study carried out in India, SHS exposure during childhood is an important risk factor for asthma and respiratory symptoms in non-smoking adults: a higher risk of having asthma emerged for exposures in childhood only or both in childhood and adulthood.75 In a Nepalese study, children asthma was associated with cigarette smoking by two or more family members and domestic use of smoky fuels.76 In a Nepalese study carried out on 6056 children, maternal smoking had a significant effect on children's ARI symptoms, mainly among those born to mothers who smoked more frequently.77 More recently, in a study carried out in Kathmandu, non-exclusive breastfeeding (with respect to exclusive one) increased the effect of household passive smoking on ARI.78
A perspective from KyrgyzstanIn Kyrgyzstan (Table 2), indoor pollution is a major risk factor among highlanders who use only biomass for cooking and heating, in poorly ventilated rooms. High level of indoor air pollution may cause respiratory symptoms among highlanders.79,80
In a study conducted in a highland and a lowland rural setting, COPD prevalence and indoor PM2.5 exposure was highest in the highlands, and were independently associated.81
The FRESH AIR research program found biomass use for heating and cooking by 71.2% and 52.0% of a sample of COPD patients, respectively;82 therefore, the health impact of reducing biomass exposure could be considerable. Among 99 adults and children living in rural communities, after implementing improved cookstoves/heaters, significant reductions of PM2.5 concentration (65%) and of daily respiratory symptoms and chest infections were found.83
A perspective from the International Primary Care Respiratory Group (IPCRG)The IPCRG is a clinically-led charitable organization for improving prevention, diagnosis and care of respiratory diseases in community settings around the world through research and education. Since 2011, in collaboration with multiple partners, IPCRG has been engaging with stakeholders in eight resource-limited settings in three continents to measure and to co-create evidence-informed programmes addressing exposure to poor indoor air and its impact on respiratory health. Where evidence about relevant interventions existed, implementation science methods were applied to test its relevance, impact and generalizability in different settings. Where it was lacking, knowledge gaps were identified and tacit colloquial and local evidence elicited to enrich understanding and to inform the development of new interventions.84
An IPCRG's FRESH AIR protocol was developed in Vietnam and in rural Uganda, contributing to an understanding that COPD may start early in life, and prevalence is highest in men and women aged 30–39, due to both high male smoking rates and also exposure to indoor biomass.85,86 RESPIRE, a Global Health Research Unit at the University of Edinburgh funded by the National Institute for Health Research (NIHR), aims to reduce the impact and number of deaths caused by respiratory diseases in Asia. A 2019 systematic review by RESPIRE found that the global prevalence of COPD among 30–79 year-old people was between 7.6%−10.3% depending on the definition used, and that smoking, biomass exposure and occupational exposure to dust or smoke were all substantial risk factors for COPD.87 RESPIRE and FRESH AIR researchers subsequently collaborated to review prevalence survey methodology for CRDs in LMICs to inform new surveys in Asia, finding that methods to map and measure COPD are more reliable than asthma.88
An adapted FRESH AIR protocol was applied in four countries with limited resources (Vietnam, Crete, Uganda and the Kyrgyz Republic), as part of a European Commission Horizon 2020 programme 2015–2019.89 It included:
- •
Structured rapid assessment highlighting three key factors that needed to be addressed: 1. perceived CRD identity when systems and education have been primarily about respiratory infection leading to inaccurate attribution of symptoms; 2. beliefs about causes of CRD: 65% strongly agreed that tobacco smoking caused symptoms, but only 19% for household air pollution; and other perceived causes included witchcraft and a hot-cold disbalance and 3. norms and social structures for example “real men smoke”.90
- •
Capacity building for health care providers (HCPs) to deliver Very Brief Advice (VBA) for quitting tobacco, pulmonary rehabilitation and community education about the harms of indoor air pollution from burning biomass fuels in the home.91
- •
Use of culturally appropriate engagement strategies including the use of photography and film.
It was concluded that contextualizing the programmes is feasible, acceptable and effective, and increases their sustainability.91
An estimated 2.6–3 billion people rely on solid fuels for cooking or heating increasing their risk of harm to their respiratory health. The impact of financial austerity may increase this use.92 Therefore, accelerating access to cleaner solutions was a target of many studies from the perspective of health, environment, climate and gender equity: yet, the results tended to be disappointing. IPCRG coordinates the Global Health Respiratory Network (GHRN), established in 2018, focusing on the poorest communities embracing use of clean cookstoves and clean fuel.93 Two studies explored the barriers to uptake and found that funds, knowledge and beliefs about the innovation of solid fuel cookstoves and clean fuels were common barriers. External policy and incentives are also important for clean fuels.94 Meanwhile, “disconnects” for example between solid fuel usage and perceived health impact and gender-related disconnect need to be understood.95 Co-developing local solutions with the community was important for success, including using sensory perceptions of mostly invisible air pollution to improve understanding. The Cleaner Cookstove Implementation Tool and the Clean Fuel Implementation Tool were proposed.94
FRESH AIR also revealed the socioeconomic impact of CRD in low-income settings: in particular, the “presenteeism” phenomenon where people attend school and work but their productivity drops; the desire among communities to improve the quality of the air they breathe. Where system-level changes are needed, making the case for change in resource-limited settings can be a major barrier.
DiscussionAn Italian perspectiveThe Italian epidemiological analytical studies confirmed a strong relationship between indoor air pollution and health status in the general population. Cooking and heating fuel, as well as SHS, were related to respiratory and allergic symptoms/diseases; exposures to NO2 and PM2.5 were associated with acute and chronic respiratory effects (symptoms, impaired lung function); allergen exposure was related to respiratory/allergic outcomes depending on allergen type and exposure period, with the strongest effects for early-life exposure.
In Italy, the GARD (GARD-I) initiative was launched in 2009 at the Ministry of Health which assumed the role of national coordinator. The overall objective of GARD-I is to reduce incidence, morbidity and mortality of respiratory diseases through an integrated and intersectoral approach aimed at their prevention, including the fight against the main modifiable risk factors.96 The working group “Project n.1 Prevention program for schools of indoor risks for respiratory and allergic diseases” produced a document on air quality in schools and risks for respiratory and allergic diseases in Italy, summarizing also the main steps to be taken to reduce indoor risks in school environments and warranting students’ well-being.97
Italian research groups participated in the SINPHONIE (Schools Indoor Pollution and Health – Observatory Network in Europe) project, performed by a consortium of 38 partners from 25 countries, contributing to release guidelines for healthy environments within European schools. These guidelines are primarily directed at the relevant policy-makers and at local authorities, secondarily to school-building designers and managers, schoolchildren and their parents, teachers and other school staff.98
In Italy, a prevention program for indoor environments is provided in the "Guidelines for the protection and promotion of health in confined environments" (Agreement between the Minister of Health, Regions and Autonomous Provinces - G.U. 27/11/2001).99
Moreover, the National Study Group (GdS) on Indoor Air Pollution (established in 2010 at the Italian Institute of Health - ISS) works to provide shared technical–scientific documents in order to allow harmonized actions at national level for improving the correct assessment of indoor air pollution.100
A perspective from other GARD countriesExposure to indoor air pollution, typically from multiple sources, is a risk factor for respiratory health, particularly in low resource settings, including people in high income countries in financial austerity. Addressing exposure should improve not only health outcomes, but also the environment, climate and also gender equity, because women typically have larger exposure than men. It will also break the cycle of infants in low resource settings having higher risks of developing CRD in later life. Success depends on developing deep insights into local beliefs and behaviours, and co-creating local primordial, primary and secondary prevention solutions building on the evidence generated about impactful interventions.
Through FRESH AIR and RESPIRE initiatives, data linking indoor air pollution and respiratory health were found and more engaging education about how we breathe and why we get breathless including new short films was created.101 In addition to smoke-related indoor air pollution, the risks of damp and mould on respiratory health have to be considered particularly in times of financial austerity when heating may be reduced and due to the impact of climate change. Researchers in island communities with high humidity and low-lying countries at risk of flooding have been developing innovative examples of community education about the risks and solutions.
Within the RESPIRE collaboration, a study performed in a rural low-literate community in southern India analyzed the lived experiences of people with CRDs: to adopt health behaviours which prevent chronic disease and ensure adequate management, people need to understand the disease, its associated risk factors and treatment options and awareness of the benefits of their health behaviours.102
Healthy behaviours are feasible but financial, social or cultural constraints may limit choices. CRDs awareness levels in rural community were limited to symptoms, duration, seasonality and available treatments for symptoms’ exacerbation. There was poor understanding of the condition, causes and risk factors for the disease.102
People typically were not aware that their disease was not curable or appreciate the efficacy of regular medications; the common practice was to attend nearby medical stores or get some local treatment for temporary relief of symptoms without consulting a doctor.102
Biomass fuel was commonly used for cooking; people were unaware that it was a risk factor for their disease and were happy to continue using it for long-term cultural practice or cost reasons.102 The use of a more efficient cooking technologies, developed with a participatory approach to meet cooking needs, showed a protective effect on the respiratory health in women and children living in the Central Mexican state of Michoacán.103,104
Improving health literacy and understanding of the disease can lead to early health seeking by the mainstream health care system. The role of HCPs in communicating with patients about risk factors, diagnosis, treatment and disease course is also extremely important. The family plays an important role in providing physical, economic and psychological support and can modulate the patient's health behavior.102
Changes in individual knowledge, awareness and attitudes should be accompanied by structural and policy changes (e.g. subsidized tariffs for gas connections, investments to address financial barriers, education and health awareness).102
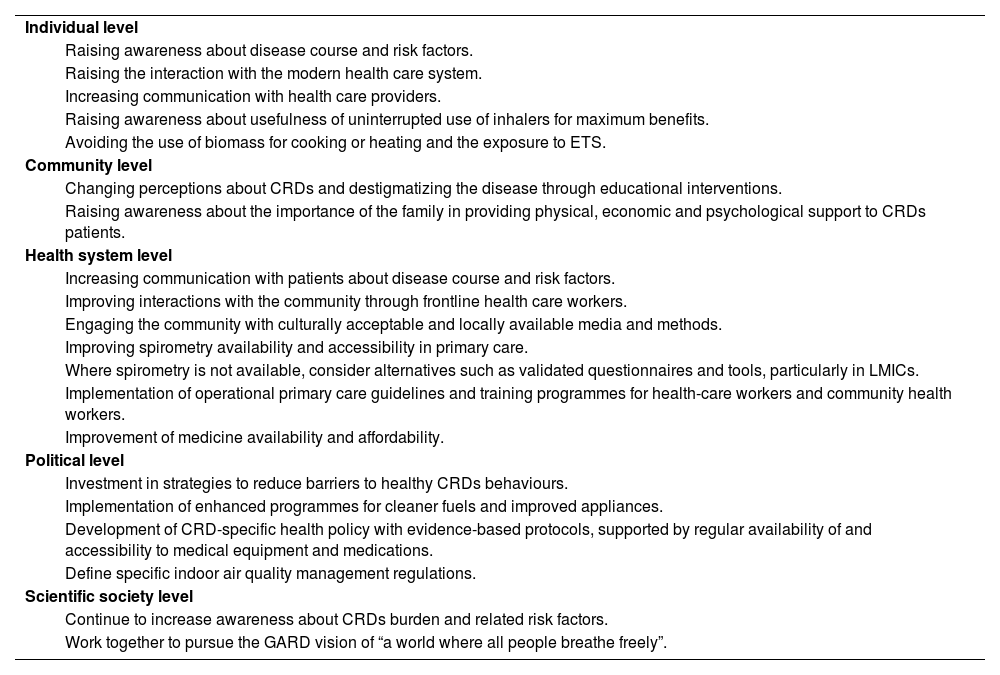
Specific interventions are needed for CRDs prevention at all levels, from patient to health system to policy (Table 3).
In the WHO European Region people spend approximately 90% of their time indoors: 2/3 of this time at home, the rest at workplace, school and public spaces.106 Hence, it is important to focus on indoor pollution.
In the absence of specific indoor air quality management regulations, the WHO has developed guidelines for indoor air quality and household fuel combustion to provide health-based recommendations on the best available fuels and technologies for protecting health.107–109
Thus, WHO, scientific societies, patient organizations and other members of the health community should work together to pursue, also for indoor air, the GARD vision of “a world where all people breathe freely” and encourage policy makers to increase their engagement in advocacy for clean air.
The authors wish to thank Patrizia Silvi (CNR Institute of Clinical Physiology, Pisa, Italy) for editorial assistance.
This work was supported in part by Ministry of Health in the framework of the National Plan for Complementary Investments (PNC) (project PREV-A-2022-12377010: MISSION).


