

Individuals recovering from SARS-CoV-2 (COVID-19) infection1 show impaired lung function, particularly diffusion capacity (DLCO).2 In addition, high prevalence of muscle weakness and impairment in physical performance have been reported in individuals without any prior motor limitations.3,4 While data report cardiac injury among professionals athletes,5-7 less is known about the potential damage to lung function and ventilatory response to exercise in asymptomatic elite athletes. Soccer is a highly physiologically demanding sport, with additional stress resulting from frequent matches and high load training sessions, ventilatory parameters playing a role in performance.8,9
In asymptomatic professional soccer players, we retrospectively report data of lung function and cardiopulmonary exercise tests after return to negativity to nasal/throat swabs for COVID-19 by polymerase chain reaction. We compare the findings with data of evaluations before the start of the sport season for license to professional activity.
The study was approved by the Ethical Committee of ICS Maugeri (2515 CE, February 9th, 2021) and participants signed the informed consent for the scientific use of their data.
Players underwent daily swabs to assess return to Covid negative. Before the sport season (T0) and the day immediately after return to Covid negative (T1: 14.3±5.4 days from testing positive), participants underwent flow-volume curve and cardiopulmonary incremental exercise test on treadmill according to standards 8,9 to be permitted to resume activity. Researchers performing analysis of data but not those performing assessments were blind to players’ identity.
Data are shown as mean ± standard deviation (SD). A Student's t-test was carried out for differences between T1 and T0. In case of failure of normality test, a Mann-Whitney Rank Sum test was performed. Linear regressions between days of Covid positive and velocity at peak exercise (VELpeak) and velocity at anaerobic threshold (VELAT) respectively, were also computed. A p value <0.05 was considered as statistically significant.
Sixteen players (22.9 ± 4.5 years; Body-Mass Index: 23.4 ± 1.9 Kg/m2) from three teams were evaluated: as expected, none reported smoking habit or any relevant disease, with negative chest physical examination. After comprehensive evaluation, including cardiological tests, all players could return to sport professional activity.
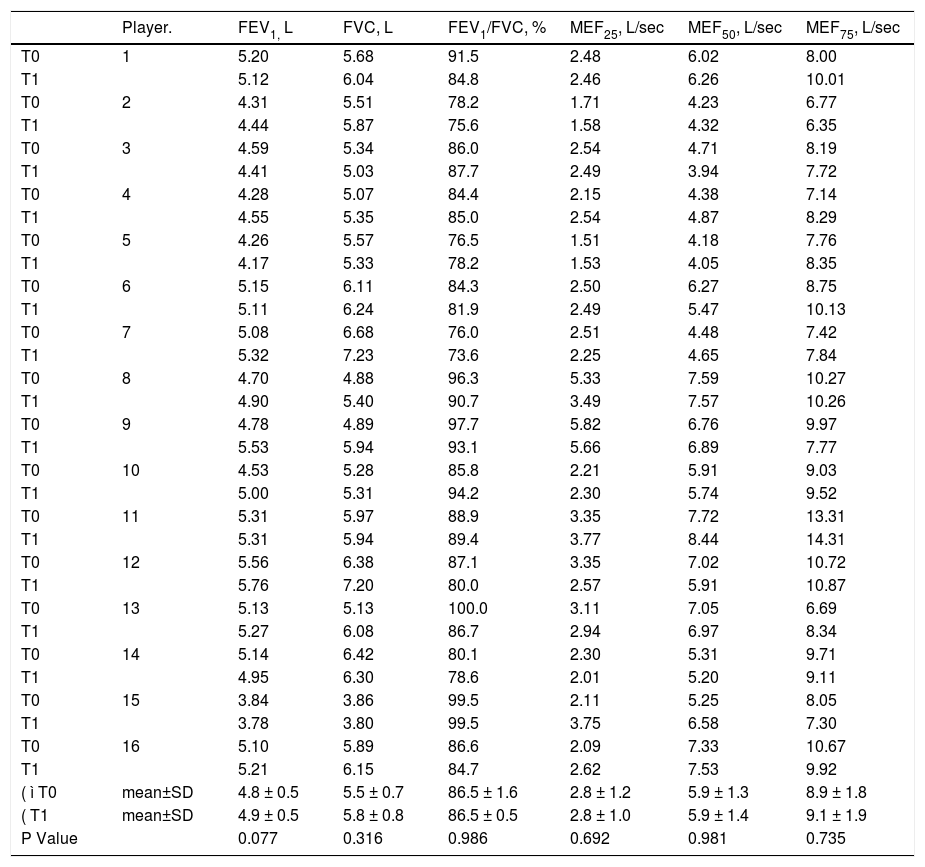
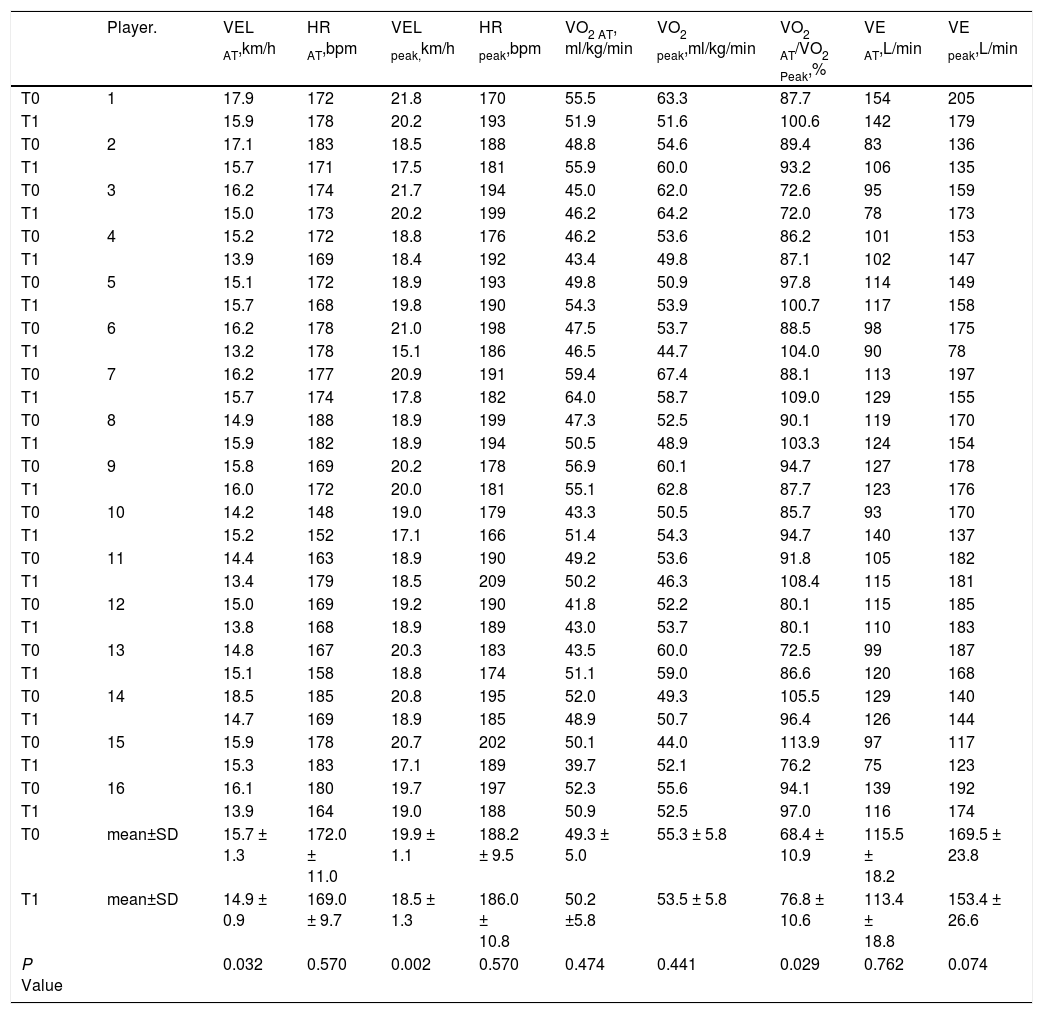
As compared to T0, at T1 there was no significant reduction in dynamic lung volumes (Table 1). However, players showed a significant mean reduction in VELpeak and VELAT, with a significant increase in oxygen consumption at anaerobic threshold to peak oxygen consumption ratio (Table 2). There was no significant correlation between days when Covid positive and T1-T0 changes in VELpeak or VELAT.
Individual and mean data of lung function.
Abbreviations. FEV1, Forced Expiratory Volume at 1 second; FVC, Forced Vital Capacity; MEF75, maximal expiratory flow at 75% of FVC; MEF50, Maximal Expiratory Flow at 50% of FVC; MEF25, Maximal Expiratory Flow at 25% of FVC.
Individual and mean data of exercise test.
Abbreviations. VELAT, exercise velocity at anaerobic threshold; HRAT, heart rate at anaerobic threshold; VEL peak: velocity at peak exercise; HRpeak, heart rate at peak exercise; VO2 AT, oxygen consumption at anaerobic threshold; VO2peak, oxygen consumption at peak exercise; VEAT, Minute Ventilation at anaerobic threshold; VEpeak, minute ventilation at peak exercise.
We have no data for immediately before infection, therefore we had to compare data after return to Covid negative with pre sport season evaluation. It has been reported that a competitive season improves ventilatory profile response to exercise in elite athletes.9 Therefore, we may argue that after the prolonged period of training and competitions performed before pandemic, the physical performance of our players would have been higher than at T0, and as a consequence the differences with post return to Covid negative even greater.
What could be the cause of reduced physical performance in these individuals? It may be argued that rest and lack of training due to imposed quarantine (at least while Covid positive) may have influenced results. However, there was no significant correlation between days when Covid positive (and rest) and reduction in exercise velocity. In addition, due to the lack of assessment of DLCO we cannot exclude any lung involvement beyond dynamic lung volumes.
We were unable to report any data of cardiac function. However, we know that all these players were allowed to return to their activity after cardiological evaluation. A large screening has reported a 3.8% prevalence of abnormalities in cardiologic screening of professional athletes 19±17 days after a positive test.6 In another study 2.3% of athletes with recent infection were diagnosed with clinical and subclinical myocarditis.7 Our study seems to suggest the importance of assessing lung function in the comprehensive evaluation of elite athletes.
Our study has the limitations of the small sample size and the flaws of a retrospective design like the lack of assessment of DLCO (or a chest CT scan), respiratory or peripheral muscle function and the lack of cardiological data.
In conclusion, with the above limitations, this study suggests that reduction in exercise performance in professional soccer players after return to negativity for COVID-19 is not associated with a reduction in dynamic lung volumes. Despite the relatively small sample size and the possible lack of external validity of these results, our findings may be useful for guiding sport medical supervisors of these players. Our study indicates also the need to assess lung function for a full evaluation of these individuals. However, to exclude any potential lung involvement, assessment also of DLCO should be mandatory.
This work was partly supported by the “Ricerca Corrente” funding scheme of the Italian Ministry of Health.


