

Despite offering a potentially lifesaving intervention for severe acute respiratory failure (SARF), venovenous (V-V) ECMO is a highly invasive and costly resource that is itself associated with significant morbidity and mortality. Scoring systems such as the Murray1 and RESP score2 have been used to aid patient selection and prognostication during the COVID-19 pandemic.3 However, these scoring systems may not accurately assess the multisystem nature of COVID-19. Thus, we set out to analyze the utility of these scores alongside other demographic, clinical, ventilatory and laboratory variables of potential prognostic importance, in a cohort of COVID-19 cases with SARF.
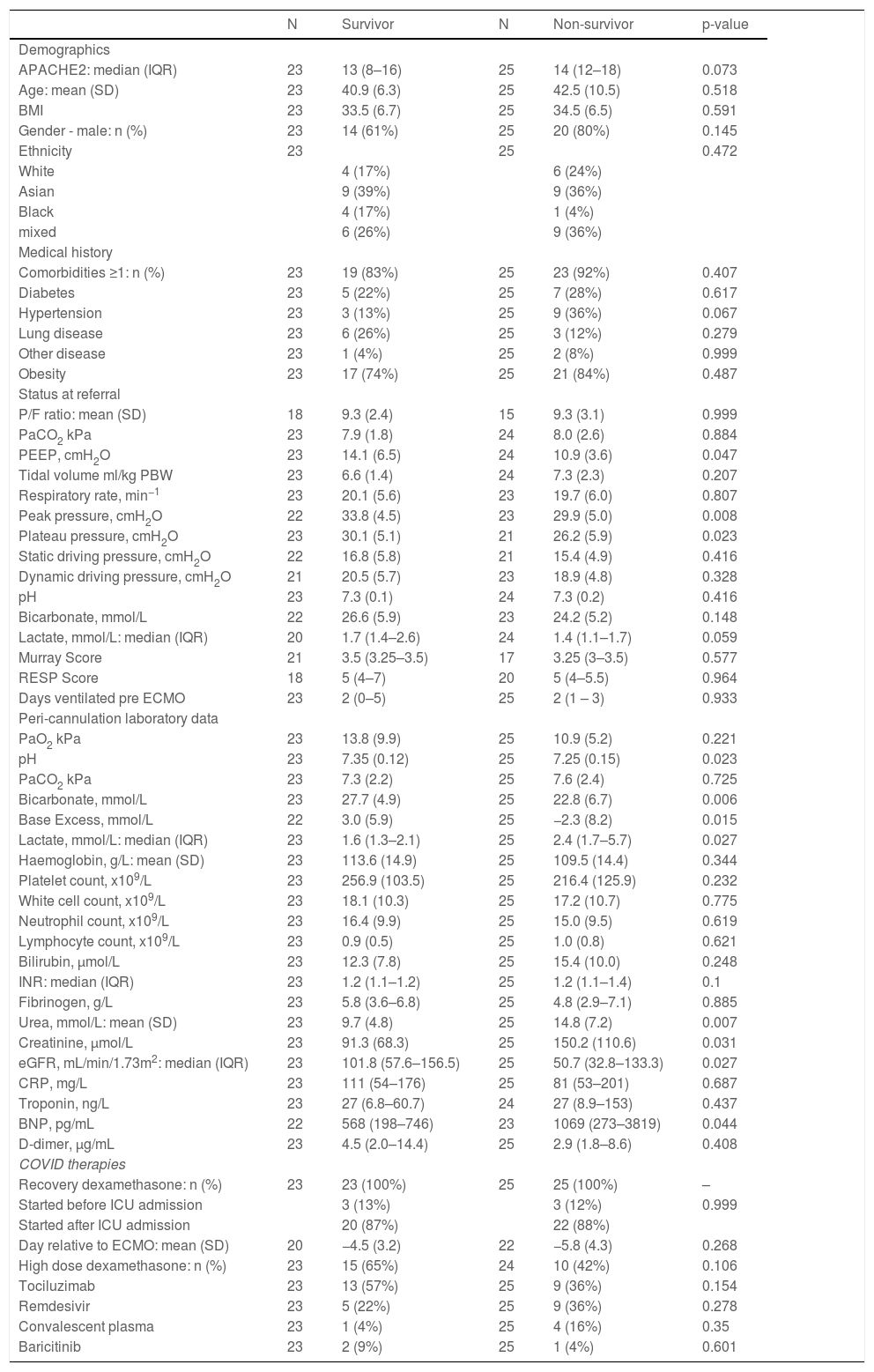
Prospectively collected data was retrospectively analyzed for all patients admitted to the Glenfield Adult Intensive Care Unit (GAICU; a large SARF and ECMO referral center in the UK) between October 2020 and March 2021 (inclusive) receiving V-V ECMO for a primary diagnosis of COVID-19 pneumonia. Demographic data alongside information provided at the time of referral in relation to ventilatory parameters and gas exchange were recorded (Table 1), and statistically compared between those who died and those who survived to ECMO decannulation and GAICU discharge (Table 2).
Baseline demographics, medical histories, baseline laboratory markers and COVID-19 treatment histories at referral and cannulation compared for survivors (n=23) and non-survivors (n=25). The differing n values reflect missing data points for these parameters. Normally-distributed data was expressed as a mean and standard deviation, whilst non-normally distributed data as a median and interquartile range. Continuous variables were compared using the Student t-test or Mann-Whitney test as appropriate, and categorical variables were compared using the Chi-squared test. Statistical analysis was performed in SAS 9.4 (SAS Institute Inc., Bucks., UK: https://www.sas.com/en_gb/contact.html).
APACHE2=acute physiologic assessment and chronic health evaluation 2 score, N=number, SD=standard deviation, IQR=interquartile range, BMI=body mass index, P/F ratio=ratio of partial pressure of arterial oxygen to fraction of inspired oxygen, pH=power of hydrogen, PaCO2=arterial partial pressure of carbon dioxide, PaO2=arterial partial pressure of oxygen, PEEP=positive end expiratory pressure, PBW=predicted body weight, INR=international normalized ratio, eGFR=estimated glomerular filtration rate, CRP=C-reactive protein, BNP=brain natriuretic peptide, ICU=intensive care unit.
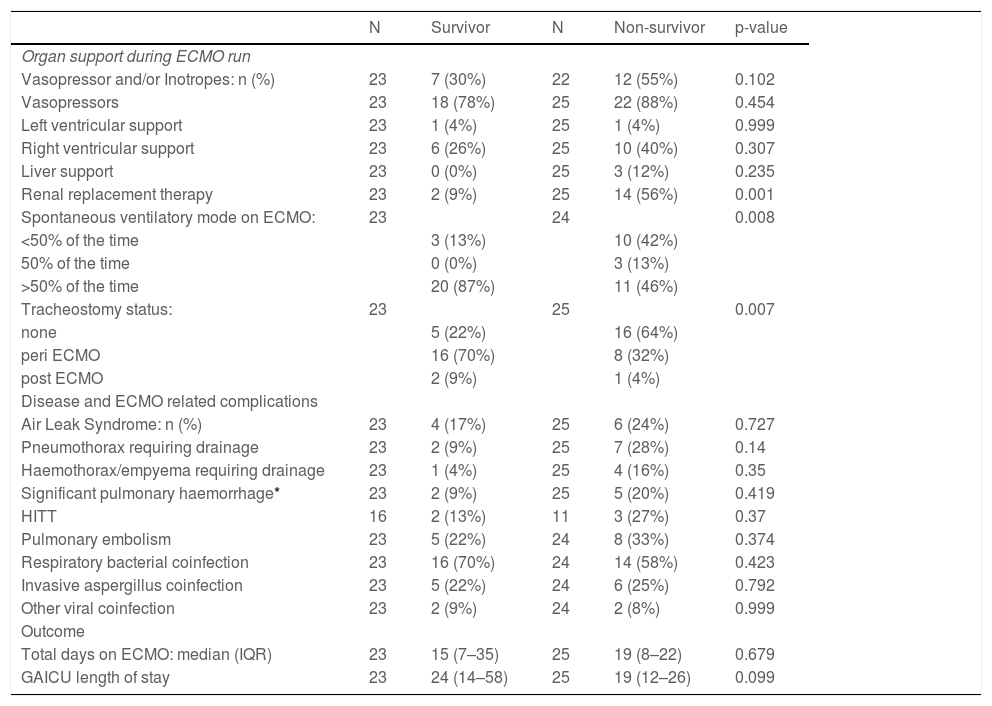
Differences in organ support, complications and outcomes between survivors (n=23) and non-survivors (n=25). Normally-distributed data was expressed as a mean and standard deviation, whilst non-normally distributed data as a median and interquartile range. Continuous variables were compared using the Student t-test or Mann-Whitney test as appropriate, and categorical variables were compared using the Chi-squared test. Statistical analysis was performed in SAS 9.4 (SAS Institute Inc., Bucks., UK: https://www.sas.com/en_gb/contact.html).
| N | Survivor | N | Non-survivor | p-value | |
|---|---|---|---|---|---|
| Organ support during ECMO run | |||||
| Vasopressor and/or Inotropes: n (%) | 23 | 7 (30%) | 22 | 12 (55%) | 0.102 |
| Vasopressors | 23 | 18 (78%) | 25 | 22 (88%) | 0.454 |
| Left ventricular support | 23 | 1 (4%) | 25 | 1 (4%) | 0.999 |
| Right ventricular support | 23 | 6 (26%) | 25 | 10 (40%) | 0.307 |
| Liver support | 23 | 0 (0%) | 25 | 3 (12%) | 0.235 |
| Renal replacement therapy | 23 | 2 (9%) | 25 | 14 (56%) | 0.001 |
| Spontaneous ventilatory mode on ECMO: | 23 | 24 | 0.008 | ||
| <50% of the time | 3 (13%) | 10 (42%) | |||
| 50% of the time | 0 (0%) | 3 (13%) | |||
| >50% of the time | 20 (87%) | 11 (46%) | |||
| Tracheostomy status: | 23 | 25 | 0.007 | ||
| none | 5 (22%) | 16 (64%) | |||
| peri ECMO | 16 (70%) | 8 (32%) | |||
| post ECMO | 2 (9%) | 1 (4%) | |||
| Disease and ECMO related complications | |||||
| Air Leak Syndrome: n (%) | 23 | 4 (17%) | 25 | 6 (24%) | 0.727 |
| Pneumothorax requiring drainage | 23 | 2 (9%) | 25 | 7 (28%) | 0.14 |
| Haemothorax/empyema requiring drainage | 23 | 1 (4%) | 25 | 4 (16%) | 0.35 |
| Significant pulmonary haemorrhage* | 23 | 2 (9%) | 25 | 5 (20%) | 0.419 |
| HITT | 16 | 2 (13%) | 11 | 3 (27%) | 0.37 |
| Pulmonary embolism | 23 | 5 (22%) | 24 | 8 (33%) | 0.374 |
| Respiratory bacterial coinfection | 23 | 16 (70%) | 24 | 14 (58%) | 0.423 |
| Invasive aspergillus coinfection | 23 | 5 (22%) | 24 | 6 (25%) | 0.792 |
| Other viral coinfection | 23 | 2 (9%) | 24 | 2 (8%) | 0.999 |
| Outcome | |||||
| Total days on ECMO: median (IQR) | 23 | 15 (7–35) | 25 | 19 (8–22) | 0.679 |
| GAICU length of stay | 23 | 24 (14–58) | 25 | 19 (12–26) | 0.099 |
N=number, HITT=heparin induced thrombotic thrombocytopenia, ECMO=extracorporeal membrane oxygenation, GAICU=Glenfield adult intensive care unit, IQR=interquartile range.
A total of 48 patients received V-V ECMO for COVID-19 pneumonia over the 6 months of the second UK wave, and 25 (52%) of them died. Patients had a median age of 42 years, body mass index (BMI) 34.0 and were more likely to be male (71%) than female. No significant differences in baseline demographics existed (Table 1) and similarly there was no difference in APACHE2 score at the time of GAICU admission, nor in Murray score or RESP score at time of referral.
Ventilation parameters were associated with prognostic outcome, with a higher positive end expiratory pressure (PEEP), peak and plateau pressure, usually reflecting more severe lung disease, paradoxically showing increased likelihood of survival. This did not correspond to a significant difference in static (plateau pressure – PEEP) or dynamic (peak pressure – PEEP) driving pressure. Biochemically a higher creatinine (lower eGFR) and urea, a relative metabolic acidosis (failure to compensate for respiratory acidosis) at time of referral, alongside a requirement for renal replacement therapy (RRT) during the ECMO run were significantly associated with mortality. Multivariable logistic regression showed that peri-cannulated bicarbonate (odds ratio per unit increase (OR) =0.80, p=0.003) and peak pressure (OR=0.75, p=0.004) remained significantly associated with mortality. There were no significant differences in the rates of co-infection or other complications between groups (Table 2).
From a treatment perspective, all patients received RECOVERY dexamethasone,4 with no significant difference in timing of initiation relative to commencement of ECMO run, nor did there exist any differences in receipt of other COVID-19 specific therapies (tociluzimab, remdesivir etc). There was a trend towards increased survival in those receiving additional higher dose dexamethasone for treatment of ARDS, however this association may not be causally linked but rather reflect clinical opportunity, similar to that of the finding of increasing tracheostomy and spontaneous ventilation rates in the survivors.
Compared to the Murray (area under ROC curve (AUC)=0.58) and the RESP score (AUC=0.51), APACHE2 (AUC=0.65) was better able to discriminate survival from non-survival in patients undergoing V-V ECMO for COVID-19 SARF, though none of the scoring tools reached statistical significance (p value 0.577, 0.964 and 0.073 respectively).
From these data, acidemia pericannulation was associated with a poor prognosis. This failure to metabolically compensate for a respiratory acidosis (the degree of which was similar between groups) is predominantly attributable to renal failure with a small contribution from lactatemia. A requirement for RRT is well known to be associated with an increase in mortality in ICU5 however in the SARF group further consideration is needed. Firstly timing of initiation of RRT and/or ECMO referral may be earlier (significant acidemia occurs sooner with concomitant respiratory-metabolic acidosis) and secondly institutional RRT practices may not facilitate adequate generation of physiological levels of bicarbonate that are frequently taken advantage of to facilitate a lung protective ventilator (LPV) strategy.
From a ventilation perspective however, there was no significant difference in severity of hypoxaemia (as assessed by PaO2/FiO2 ratio) at time of referral, and we can infer no significant difference in dead space ventilation (PaCO2, adjusted tidal volume, respiratory rate, BMI and pulmonary embolism rates similar across groups). While both cohorts at referral generally had tidal volumes <8ml/kg/predicted body weight in keeping with a LPV strategy, the survivors had a significantly higher PEEP, plateau and peak pressures compared to non-survivors.
One possible explanation for these seemingly disparate findings is that patients being subjected to more injurious ventilation (whether or not that represents a cohort with more severe respiratory disease) have more to gain from the lung rest facilitated by V-V ECMO. Another possible explanation is that as lung injury reversibility forms a key part of eligibility criteria at the time of assessment of candidacy for V-V ECMO, SARF severity per se may no longer then be significantly discriminatory and systemic sequelae of disease and ECMO-related complications play a greater role in determining outcome.
A recent systematic review and meta-analysis of ECMO for COVID-19 found that, mortality has increased as the pandemic progressed, a finding that has been echoed in our experience also.6,7 This has been postulated to be due to multiple factors to include evolution in both the disease (increased virulence) and its therapeutic strategies (selecting out those with treatment failure), changes to patient selection more generally and resource availability. Recently Urner et al. used multinational data and statistical modelling to emulate a pragmatic randomized controlled trial, designed to estimate the effect of ECMO in severe respiratory failure from COVID-19. They found that ECMO was most effective in patients <65 years old, with PaO2/FiO2 < 10.7 kPa, driving pressures >15 cm.H2O within the first 10 days of mechanical ventilation8 – a cohort well represented in this study. Whilst mortality with ECMO in COVID-19 is high, a recent UK matched cohort study supports a survival benefit with ECMO in this population.9 Outcomes from ECMO in COVID-19 patients are particularly sensitive to individual patient parameters at the time of presentation. As both disease and treatments evolve, broad comparisons of clinical outcomes may be less relevant to the decision to admit a COVID-19 for ECMO therapy than the pattern of illness they have at that time.
None.


