



There is a lack of information regarding bronchoscopy practice in adults in Portugal. Our objective was to obtain an overview of the characteristics, resources, techniques and behaviors in national interventional pulmonology (IP) units, before and after SARS-CoV-2 outbreak.
Materials and MethodsAn online survey was developed by an expert panel with a total of 46 questions comprising the specifications of each unit, namely physical space, equipment, staff, procedure planning, monitoring, technical differentiation, and numbers pre- and post-COVID-19. Forty-one interventional pulmonology centers were invited to participate between April and May 2021.
Results37 units (90.2%) responded to the survey. The majority (64.9%) have a fully dedicated space with a weekly presence of ≥3 chest physicians (82.1%) and support of an anesthesiologist on specific days (48.6%). There is marked heterogeneity in the IP unit's equipment, and 56.8% acquired disposable bronchoscopes after COVID-19 pandemics. Pre-bronchoscopy hemogram, platelet count and coagulation tests are regularly asked by more than 90% of the units, even when deep sedation or biopsies are not planned. In 97.3% of cases, topical anesthesia and midazolam are utilized. Propofol (21.6%) and fentanyl (29.7%) are occasionally employed in some institutions. Most units use ancillary sampling techniques to diagnose central or peripheral lesions, with radial EBUS being used for guidance of distal procedures in 37.8% of centers, linear EBUS and EUS-B-FNA for mediastinal diagnosis and/or staging in 45.9% and 27.0% of units, respectively. Cryobiopsies are used by 21.6% of respondents to diagnose diffuse lung diseases. Rigid bronchoscopy is performed in 37.8% of centers. There was a decrease in the number of flexible (p < 0.001) and rigid (p = 0.005) bronchoscopies and an upscale of personal protective equipment (PPE) during the COVID-19 outbreak.
ConclusionsIP units have variable bronchoscopic practices, but during the COVID-19 pandemic, they complied with most international recommendations, as elective procedures were postponed and PPE levels increased.
Bronchology and Interventional Pulmonology (IP) has evolved significantly in the last 20 years, with the development of technologies and practices. Despite the existence of several guidelines from international associations and institutions, most are recommendations set by experts in this field and more focused on safety and functional aspects than in robust scientific evidence, so procedures are usually not standardised.1–7
Considering the existing variance of methods and the little knowledge about bronchoscopy practices, several countries undertook national surveys to characterize the availability of resources, the clinical application of techniques, and its specificities.8–15 In 2018, a national study was published evaluating, specifically, the use of pleuroscopy in Portuguese pulmonology departments, considering availability, professionals’ experience and training, number of procedures and its characteristics.16
Recently, because of the Coronavirus Disease 2019 (COVID-19) pandemic outbreak, the Portuguese Pulmonology Society published a consensus statement aiming at the safety of both patients, medical practitioners and other health professionals during bronchoscopy and pleural procedures.17 Based on current knowledge, all patients should be assumed as potentially infected with the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2); therefore, specific measures must be implemented, including organizational issues, physical space and material preparation, and personal protection equipment (PPE) of all professionals involved.17
These recent changes in the bronchology field were expected to have a major impact on national interventional pulmonology units, so the Committee on Endoscopic Techniques of the Portuguese Pulmonology Society nominated a working group to conduct a national survey, to accurately characterize the Portuguese panorama. Specifically, this survey aimed to quantify and qualify the human and technical resources of the Portuguese Pulmonology Departments, the specificities of the bronchoscopic procedures performed, and compare the reality before and after the COVID-19 pandemic.
MethodsThe expert panel developed a structured questionnaire in Google Forms, and the link was e-mailed to the Bronchology Units or Pulmonology Departments of all Portuguese public hospitals and some private institutions/hospitals considering their representativeness (Supplementary Table 1). Respondents had one month to reply and send the completed form; one reminder was sent to all, and those who did not answer were further contacted by phone. The survey occurred between 22nd April and 31st May 2021.
The questionnaire comprised 46 questions, either of quantitative or multiple option answer, considering the following sections: 1) respondent and hospital identification; 2) Interventional Pulmonology Unit characterization; 3) staff experience in bronchology; 4) nursing and 5) anesthesiology support; 6) equipment characterization; 7) planning and monitoring of the bronchoscopic procedures, including procedure specifications (e.g. complementary diagnostic tests before bronchoscopy, methods of sedation and patient monitoring); 8) endoscopist PPE pre and post the emergence of COVID-19 pandemic; 9) accessory diagnostic and therapy techniques by flexible bronchoscopy, including the number of procedures pre and post COVID-19; and 10) rigid bronchoscopy, comprising the number of procedures pre and post COVID-19.
Responses were downloaded as an Excel spreadsheet. Descriptive analysis was performed using the software SPSSv24®. The survey results were analyzed based on the total number of answers to each question and are presented as mean±standard deviation and median (range) for continuous variables, and as frequency and percentage for categorical variables. Paired samples t-student test was used to compare the means of two variables of the same sample measured in sequential years. A difference of at least 5% (two-tailed) was considered statistically significant.
ResultsA total of 41 eligible Portuguese interventional pulmonology centers were invited to participate (Supplementary table 1), and 37 (90.2%) answered the entire online questionnaire. The responders included in this analysis are listed by their district in Fig. 1 and represent almost all geographic locations in the country.
General characterization of the IP units
The units were located on nine university public hospitals, 23 tertiary public hospitals, and two private hospitals. In 24 cases (64.9%), the unit space was fully dedicated to bronchoscopy/pleural procedures; in 12 (32.4%), the physical location was shared with other specialties, and in one case, the procedures were performed in a hospital operating room.
Thirty IP units (81.1%) reported the weekly presence of three or more chest physicians performing the procedures, six (16.2%) had the regular presence of two pulmonologists, and one (2.7%) relied on one doctor.
Regarding the existence of dedicated nurses with specific IP training, three units (8.1%) stated the usual presence of one nurse, 13 (35.1%) referred two rotating nurses, ten units (27%) three nurses, and another 10 (27%), four or more nurses. One unit indicated the absence of trained nurses.
Eighteen units (48.6%) had the regular support of an anesthesiologist on specific weekdays. In 15 cases (40.5%), an anesthesiologist was present in the bronchoscopy suite-only upon request. This occurred on 1-2 days/week in 16 cases, 3-4 days/week in two cases and five days/week in other two units (totally dedicated to cancer patients). Four units (10.8%) had no assistance from an anesthesiologist.
On a regular year, the IP units reported an average of nearly 500 flexible bronchoscopies per year. However, great heterogeneity was observed with 14 centers (37.8%) registering 500 exams/year or more, 18 (48.6%) 200 to 499 exams/year and five (13,5%) less than 200 exams/year.
Overall, we were able to analyze the profile of 103 pulmonologists. Of these, 41 (39.8%) had over 15 years of experience in bronchoscopy, 23 (22.3%) had 10 to 14 years of previous experience, 25 (24.3%) had 5 to 9 years, and 14 (13.6%) had less than 5 five years of IP experience. Concerning the areas of expertise, all answering chest physicians had experience in flexible bronchoscopy, while 37 (35.9%) reported proficiency in rigid bronchoscopy and 37 (35.9%) in endobronchial ultrasound.
Pleuroscopy/medical thoracoscopy was performed by 46 (44.6%) of the respondents and was reported to be available in 20 centers.
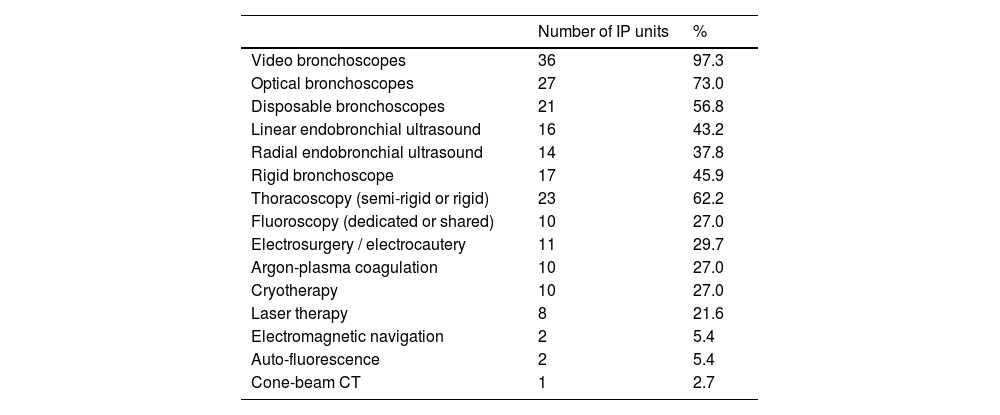
Table 1 shows the unit's equipment. Most units (56.8%) promoted the acquisition of disposable bronchoscopes after COVID-19 pandemics. Twenty-five health care facilities (67.6%) reported using automatic high-level disinfection to reprocess their reusable bronchoscopes and accessories. In 11 hospitals (29.7%), sterilization was the reported selected method, if available, because of its greater efficacy in reducing microorganism's contamination. In one unit (2.7%), the cleaning and disinfection of the equipment was entirely manual. After reprocessing, to minimize the likelihood of recontamination, the equipment was stored in ventilated cabinets in 19 units (51.4%) and in non-ventilated facilities in 18 units (48.6%).
IP units’ equipment.
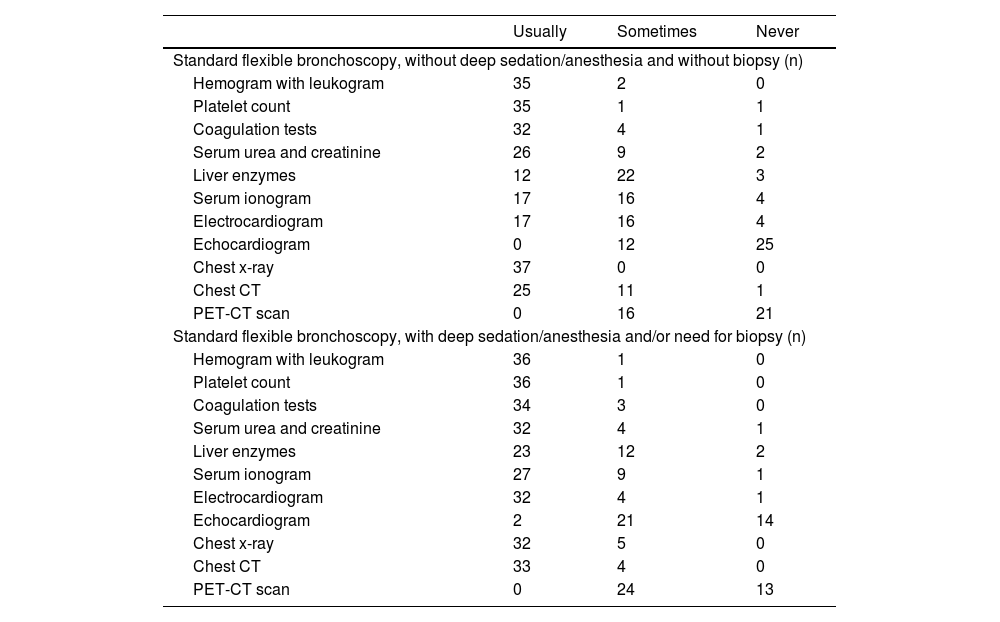
Most participants (86.5%) responded that they usually ask for at least one pre-procedural exam to evaluate each patient that is going to be submitted to a standard flexible bronchoscopy without deep sedation/anesthesia when the main purpose is the inspection of the airways and sample collection without the need for biopsies. Similarly, most proceduralists (89.2%) require more than one pre-procedure complimentary exam when sedation or biopsies are planned Table 2. presents the complementary exams asked in each situation.
Pre-procedural complementary exams required when performing standard flexible bronchoscopy.
Most flexible bronchoscopies were reported to be performed with topical anesthesia (with or without conscious sedation) using lidocaine in the form of gel (“usually” n = 30, 81.1%; or “sometimes” n = 6, 16.2%), nebulized (“usually” n = 27, 73%; or “sometimes“ n = 7, 18.9%), and/or liquid in the tracheobronchial tree as “spray as you go” technique (“usually” n = 19, 51.4%; or “sometimes” n = 6, 16.2%). The most common drug used by the pulmonologists for sedation was midazolam in 97.3% of units (“usually” n = 25, or “sometimes” n = 11). Propofol and fentanyl were occasionally employed during bronchoscopy in 8 (21.6%) and 11 (29.7%) institutions, respectively.
Twenty-nine respondents (78.4%) affirmed that supplemental oxygen was routinely administered since the beginning of each flexible bronchoscopy. In contrast, the remaining eight (21.6%) participants showed a preference in administering supplemental oxygen only if required due to peripheral oxygen desaturation during the procedure.
When asked about the patient's monitoring during flexible bronchoscopy without deep sedation, all 37 participants referred to assessing heart rate and pulse oximetry throughout the procedure. Non-invasive blood pressure was measured by 33 respondents (89.2%), and ECG monitoring was monitored by 23 participants (62.2%).
When deep sedation was planned, end-tidal CO2 was evaluated by one participant unit (2.7%), monitor ECG was performed by 31 participants (83.8%), non-invasive blood pressure by 35 (94.6%), and all respondents referred to monitor heart rate and pulse oximetry. In both scenarios, one respondent added clinical observation, and another external pace defibrillator monitoring.
Bronchoscopy technical featuresRegarding the diagnosis of central/tracheobronchial lesions by flexible bronchoscopy, biopsy forceps were used by all 37 participant units; bronchial brushings by 36 (97.3%); and needle aspiration by 31 (83.8%). Bronchial cryobiopsies were reported by seven (18.9%) participants.
Cryobiopsies were also the least reported procedure in the diagnosis of peripheral lung lesions, used by six (16.2%) respondents. Peripheral biopsy forceps and brushing were among the most used procedures for diagnosing peripheral lesions, reported by 33 (89.1%) participants in both cases. Radial EBUS and fluoroscopy were used as guidance for distal procedures in 14 (37.8%) and 10 (27.0%) centers, respectively.
In diffuse lung diseases, bronchoalveolar lavage was the preferred method, reported by all 37 centers. Transbronchial forceps biopsies were used by 33 (89.2%) of the participants, while eight centers (21.6%) reported performing transbronchial lung cryobiopsies. Fluoroscopy was used by seven centers (18.9%) to guide the adjunctive procedures for the diagnosis of diffuse lung diseases.
In what concerns the diagnosis of mediastinal lesions, non-guided transbronchial needle aspiration (TBNA) was used by 32 centers (86.5%). In contrast, EBUS-TBNA was used by 17 centers (45.9%) and EUS-B-FNA in 10 centers (27.0%).
Concerning therapeutic techniques, 34 (91.9%) centers reported using flexible bronchoscopy to remove foreign bodies. Control of hemoptysis was attempted through balloon tamponade by 30 (81.0%) centers, whereas 31 (83.8%) units used some form of thermal energy, of which LASER was the preferred, employed by 14 (37.8%) centers, followed by argon-plasma coagulation, used by 10 (27.0%) centers. Airway repermeabilization through self-expandable stents placed through flexible bronchoscopy was reported by 7 (18.9%) centers.
Other endobronchial therapeutic maneuvers such as bronchial thermoplasty and bronchoscopic lung volume reduction (with one-way valves, coils or thermal ablation) were not reported by any center.
The average number of flexible bronchoscopies reported to have been performed by all 37 participant centers in 2020 (amid the COVID-19 pandemic) was 345 (±249). When asked about the estimated annual number of flexible bronchoscopies performed during 2019 (before the pandemic), the reported average number was 500 (±346). There was a statistically significant decrease in the number of bronchoscopies performed due to the COVID-19 pandemic, which raised to an average of -155 (p < 0.001). The distribution of reported exams and the impact of the COVID-19 pandemic on the workload of flexible bronchoscopy is reported in detail in Table 3. In 2020, on average, 84% (±12.6%) of flexible bronchoscopy procedures were performed mainly with a diagnostic intent.
Seventeen IP units reported to have a rigid bronchoscope and 14 referred to perform the procedure. Proceduralists used rigid bronchoscopy to conduct one or more adjunctive procedures: 100% mechanical debulking (“usually” n = 12; or “sometimes” n = 2); 57.1% LASER ablation (“usually” n = 7; or “sometimes” n = 1); 57.1% argon-plasma coagulation (“usually” n = 6; or “sometimes” n = 2); 50% electrosurgery (“usually” n = 3; or “sometimes” n = 4); 50% cryoablation (“usually” n = 2; or “sometimes” n = 5).
Eleven centers (29.7%) reported airway stenting deployment by rigid bronchoscopy to maintain tracheobronchial patency. Between all commercially available, the Dumon (straight or Y) and Hood stents were the most frequently used in the Portuguese IP units (Dumon n = 11, Hood n = 8, Ultraflex n = 5, Polyflex n = 4, Silmet n = 4, Dynamic Y-stent n = 3, Montgomery T-tube n = 3, Aerstent n = 2, Micro-tech n = 1, Noppen n = 1 unit). Several airway stent complications were commonly reported by most centers, being the most frequent: stent migration (n = 11), obstruction by secretions (n = 10), obstruction by granulation tissue (n = 10), chronic cough (n = 5), and infection (n = 3).
Of these 14 units performing rigid bronchoscopy, 11 retrieved their estimated annual number of procedures performed both in 2020 and also on a regular year (before the COVID-19 pandemic). On average, IP units performed 96±99.3 (range 7-302) rigid bronchoscopies during 2019 (before the pandemic), whereas in 2020, the average number of reported rigid bronchoscopy was 70±81.2 (range 0-237). When assessing the impact of the COVID-19 pandemic on rigid bronchoscopy overall workload, a statistically significant average decrease of –26 procedures was observed (p = 0.005).
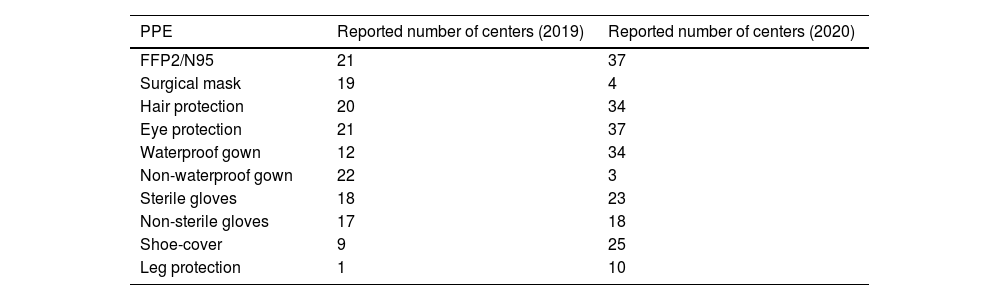
Health professionals' protectionWhen asked about the current use of personal protection equipment (PPE) during interventional bronchoscopy, all 37 units confirmed choosing FFP2/N95 single-use face masks (four in combination with a surgical face mask), some sort of eye protection, single-use gown and single-use waterproof gloves Table 4. presents the standard PPE reported to be used in 2019 (before the pandemic) and afterwards.
DiscussionThis survey identifies a marked heterogeneity of bronchoscopy practice and resources in adults IP units across Portugal's mainland. This was a comprehensive and extended questionnaire that was able to assess the prevalence of the practice in the country and the impact of COVID-19 at a national level. It is evident that the number and type of procedures performed decreased during the pandemic period; most units equipped themselves with disposable bronchoscopes, and there was a shift in the type and level of protective equipment used to increase safety for staff and patients.
Surveys in IP have been published since the 90s.10 When compared to some historical questionnaires that were able to provide the clinical picture of bronchoscopy in North America and in some European countries, much as evolved regarding practice and technical developments. The number and indications of rigid bronchoscopies have declined, new techniques have emerged (e.g., EBUS and cryobiopsies), sedation and anesthesia are now regarded as mandatory in most units and demanded by patients.
The survey response rate was very high, and the findings reveal, as expected, the national panorama, in which the majority of centers are based in Lisbon and Porto metropolitan areas and in the coastal region, where more than half of the Portuguese population lives.18
Most units (65%) are fully dedicated to bronchoscopy, more than 90% have two or more trained pulmonologists, and in 84% of cases, at least one has at least ten years of IP experience. In contrast, 46% of units have two or fewer nurses, and most of them are not fully dedicated to bronchoscopy. It is worth mentioning that there is no specific post-graduation education in IP for nurses in the country. We may speculate that the small number of nurses trained and committed to this area may impact the quality of the exams. The British Thoracic Society advised the presence of at least two qualified nurses during bronchoscopy.1 In contrast, the European Respiratory Society and the American Thoracic Society instruct on the need for one to two dedicated nurses during interventional pulmonology procedures without anesthesia (with a third nurse required to help the anesthesiologist in the procedures performed under deep sedation / general anesthesia).2 Therefore, efforts should be made to assure that nursing staff receives adequate standardized training in IP and that all units move on to comply with international recommendations and demand the regular presence of an adequate number of trained nurses. This number may vary depending on the workflow volume of the individual units. Still, it should not be less than two (with possible rotation) in low volume units, to at least three (non-rotating) in high volume units that perform advanced interventional bronchoscopy and have regular anesthesiology support.
There is great heterogeneity in technical resources and equipment between IP units, with more than half performing only basic exams. A third uses rigid bronchoscopy, which is sufficient for the country necessities, according to the number of habitants. In 2019, 16 centers performed linear EBUS, whereas in 2014 only six did it, as reported by the Survey of Pulmonology Services, prepared as part of the review of the Pulmonology Referral Network.19 This expansion follows the natural evolution of IP units worldwide since EBUS is an important tool for mediastinal staging in lung cancer patients and in diagnosing malignant or benign lesions adjacent to the tracheobronchial tree or the oesophagus.20 For the diagnosis of peripheral pulmonary nodules, 14 units have radial EBUS, ten fluoroscopy and two have electromagnetic navigation, which enables an increase in diagnostic accuracy. Regarding the COVID-19 pandemic, 56.8% of the units now have single-use bronchoscopes, which were not regularly utilized. This equipment will certainly have an increasing application in the near future due to its benefits regarding the risk of contamination, availability and preserved efficacy in most emergent clinical scenarios.21
Concerning the number of procedures per year, the present survey shows a clear negative impact of the COVID-19 pandemic period, with a decrease by 30% on the average number of flexible bronchoscopies and 27% on rigid bronchoscopies. This is in line with other published studies,22–24 where IP procedure work-load considerably decreased or was even abolished during the COVID-19 era. Elective procedures in COVID-19 negative patients were postponed and rescheduled as recommended by consensus guidelines.17,25
Some kind of sedation/anesthesia is required to reduce patient's discomfort, enhance safety6,26 reduce procedure duration and increase diagnostic accuracy. The preferred method for bronchoscopic diagnostic procedures is conscious sedation with antianxiety and/or analgesic medications, in combination with local anesthesia, titrated by bronchoscopists and supervised by the team. Most guidelines suggest the combination of a sedative agent with an opioid since it decreases cough and pain, improves patients’ tolerance, and reduces the total dose of sedative drugs.27 In the present assessment, more than 97% of the IP units in the country confirmed the use of midazolam. Still, only 29.7% associated an opioid, probably due to a reduced experience with this medication and fear of complications in patients with previous respiratory diseases. These results are in-line with other real-life studies.11,28
It is worth mentioning that conscious sedation has limitations, and prolonged, complex, and technically demanding bronchoscopies or therapeutic procedures usually require deeper sedation/general anesthesia with the support of an anesthesiologist, not involved in the intervention itself.29 The survey identified the lack of available anesthesiologists as a potential problem, with only 5% and 48.6% of the units having the collaboration of this specialty on a daily or regular basis, respectively.
As pre-procedural requirements, nearly all responders ask routinely for a full blood count (97%), coagulation studies (92%), renal function (86%) and an electrocardiogram, even when there is no history of abnormal coagulation or cardiac risk. These numbers are much higher when compared to other published surveys. In 2002, in the United Kingdom, when performing bronchoscopy without transbronchial biopsy, physicians routinely asked for a full blood count in 57%, blood urea and electrolytes in 43% and clotting function in 18% of cases. When a transbronchial biopsy is needed, 91% asked for a full blood count and 88% asked for clotting tests.12 This highlights the deviation of real-life performance compared to international guidelines and current scientific literature, which states that the routine performance of coagulation studies, platelet counts, and hemoglobin levels before flexible bronchoscopy is not recommended, especially when there are no previous identifiable risk factors.26,30 On the other hand, a pre-procedural chest CT scan was not consistently required by 32,4% of participants. Though we acknowledge that a chest CT can be dismissed upon emergent situations (mainly emergent therapeutic bronchoscopy), the number of centers that reported inconsistent demand of this valuable exam was concerning. Again, we stress the need to standardize procedures and comply with international recommendations that underline the importance of CT in preparation for bronchoscopy.1,2,19 Clinical evaluation should dictate other pre-bronchoscopy investigations on an individual basis, and this should be stressed to avoid submitting the patients to unnecessary exams and increase healthcare costs.
According to the recommendations of a few guidelines,26,30 and good clinical practice, all Portuguese units monitor heart rate and oxygen saturation, and generally add non-invasive blood pressure and continuous ECG in patients undergoing flexible bronchoscopy, especially when deep sedation is planned. It is recognized that deficient monitoring in deep sedation may lead to unnoticed respiratory depression, changes in normal blood pressure and arrhythmia, which increase the probability of complications during bronchoscopy. This awareness was acquired especially in the last two decades, compared to the survey conducted by Smyth et al, where only 22% and 10% of physicians reported monitoring ECG and blood pressure, respectively.12 A recent systematic review by Strohleit et al,27 reinforces the idea that there is still the need for further research in this area due to the scarcity of evidence of published papers.
In the current study, most units combine biopsy, brushing and needle aspiration for the diagnosis of endobronchial lesions, to obtain the highest diagnostic yield.31 Compared to other published surveys that proved the underuse of TBNA,8 we highlight that 83.8% of centers are able to perform non-guided TBNA in central lesions and 86.5% in mediastinal lesions (including centers that also perform EBUS-TBNA). Interestingly, non-guided TBNA accuracy has been reported to benefit from previous EBUS training.32 Still, we believe that the overlap of both techniques in the same centers can be explained by the formers’ wider accessibility and lower costs. Although EBUS-TBNA is used in 45.9% of units, EUS-B-FNA is only performed in 27% of centers, probably related to the lack of specific training. This reinforces the need for educational programs in this area for both residents and senior chest physicians.
In this survey, transbronchial lung cryobiopsies were performed in a scarce number of hospitals (8 out of 37). This finding perhaps reflects the novelty of this procedure and the need to complete a high volume of procedures, which has been suggested as a requirement to gain and maintain adequate proficiency in this technique.33 Still, considering transbronchial lung cryobiopsies, we found some important deviations of the current guidelines34 and expert panel standardization recommendations35 concerning the utilization of fluoroscopic control, that according to our results, was not available in one center. This practice is not in line with the safety recommendations for this procedure. Though we could not assess other in-depth details, outcomes or complications, we strongly underline the need to comply with the currently available best practice recommendations34,35 to avoid unnecessary risks.
Another important finding of our survey was the complete absence of offer, among all respondent centers, of two important and validated endobronchial therapies: bronchial thermoplasty (recommended for selected asthmatic patients in GINA grade 5 of symptomatic control, evidence B)36 and bronchoscopic lung volume reduction strategies (recommended for selected emphysematous COPD patients with significant lung hyperinflation despite optimal medical care)37. The reasons for this finding are out of the scope of this paper but may include national regulatory and reimbursement issues that deserve prompt elucidation.
They are crucial regarding infectious control measures, since it has been proved that not sufficiently protected healthcare workers attending or performing aerosol-generating procedures have a higher risk of infection.38 In 2002, in the UK, a national survey reported that only 9% of physicians used four protective items: face mask, gloves, eye protection, and gown.12 The recommendations of PPE during bronchoscopy have been upscaled since 2020 in the context of the COVID-19 pandemic and, again, most units comply with them. The awareness of safety issues of Portuguese bronchoscopists and staff attending the procedures increased noticeably after COVID-19, with 100% of centers using FFP2/N95 masks and eye protection. Recent studies have shown that most proceduralists understand the gravity of the situation and paid particular attention to the use of appropriate PPE,22 but in real clinical practice, and especially at the peak of the pandemic, some of the international recommendations were quite difficult to follow and implement.24,39
In recent articles, authors report that transmission of SARS-CoV-2 seems to be low with consistent use of appropriate personal protective equipment by healthcare workers when all the measures are followed.40,41
Meanwhile, on the 26th of November 2021, World Health Organization (WHO) designated the variant B.1.1.529 named Omicron as a variant of concern (VOC), with a considerable rise in cases of people testing positive for SARS-CoV-2 in South Africa in regions where the Omicron variant emerged.42.This variant, considered to be more contagious and associated with an increase in the risk of reinfection after a primary infection than the previous mutations, shows more than 30 mutations leading to amino-acid changes in the Spike sequence.43
The question of severity and this new variant is not clear yet. However, it is suggested to be less aggressive.44 Presently, there are too many confounding factors to compare patients with the Omicron variant with patients infected by other variants. In fact, COVID-19 severity and mortality vary enormously depending on the country, the prevalence of vaccination, the population's characteristics.
For these reasons, it is not expected that our level of care as healthcare workers will change in the near future.
There are some obvious limitations of our study and all surveys for that matter: answers rely on personal or unit databases and, in some instances, on the memory of participants (there is no national database); lack of objectivity of some responders; differences in question interpretation; replies could not be verified; some topics were simplified and others not covered, to reduce the overall length and avoid a reduced response rate. We also acknowledge that there were questions regarding duration of practice but non-related to training or competence maintenance, and the design questionnaire was not able to assess the quality of procedures which is at least as important as the numbers, equipment or techniques attributed to each unit.
ConclusionThe present survey assessed present trends and the impact of COVID-19 in bronchoscopy practices in Portugal. It does not provide any recommendations or IP standards as with other questionnaires. It suggests that IP units in the country have a wide range of characteristics and behaviors, but during the COVID-19 pandemic, they complied with most international recommendations, as elective procedures were postponed and PPE levels increased.
Practice in the bronchoscopy field was previously guided by personal experience, determined by the peculiarities of a particular unit as new members would mimic and adopt the attitudes of older practitioners. Nowadays, there is the need to standardize practice and enhance training and competence maintenance of IP physicians within the country. The current survey helps to understand the reality and may settle the foundations to improve the IP field in Portugal, with the development of a future national database, homogenize procedures and protocols, and even organize and design better training programs.
Supplementary MaterialSupplementary table 1. Pulmonology Departments invited to participate
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
We thank Prime Focus for providing language help and writing assistance to this article.


