



Lung cancer (LC) is a leading cause of cancer-related mortality worldwide. Lung Cancer Screening (LCS) programs that use low-dose computed tomography (LDCT) have been shown to reduce LC mortality by up to 25 % and are considered cost-effective. The European Health Union has encouraged its Member States to explore the feasibility of LCS implementation in their respective countries.
The task force conducted a comprehensive literature review and engaged in extensive discussions to provide recommendations.
These recommendations encompass the essential components required to initiate pilot LCS programs following the guidelines established by the World Health Organization. They were tailored to align with the specific context of the Portuguese healthcare system. The document addresses critical aspects, including the eligible population, methods for issuing invitations, radiological prerequisites, procedures for reporting results, referral processes, diagnostic strategies, program implementation, and ongoing monitoring. Furthermore, the task force emphasized that pairing LCS with evidence-based smoking cessation should be the standard of care for a high-quality screening program. This document also identifies areas for further research.
These recommendations aim to guarantee that the implementation of a Portuguese LCS program ensures high-quality standards, consistency, and uniformity across centres.
Lung cancer (LC) is the second most common cancer worldwide and has the highest mortality rate.1 Updated predictions of cancer mortality suggest a declining trend for most cancers across Europe owing to advances in prevention, screening, and treatment. However, LC mortality is expected to increase, particularly among women.2 In 2019, Portugal recorded 5923 new LC cases, with a crude incidence rate of 57.5 per 100,000 inhabitants.3 It is the second most common cancer in men, following prostate cancer, and the fourth most common cancer among women, after breast, colorectal, and thyroid cancers. Lung cancer is the leading cause of cancer-related deaths in Portugal, accounting for 15.4 % of all cancer-related fatalities. In 2019, it accounted for 4391 deaths in Portugal, with a crude mortality rate of 42.7 deaths per 100,000 inhabitants.4 Patients with LC often seek healthcare services at an advanced stage, resulting in delayed diagnosis and a less favourable prognosis. Therefore, early diagnosis is of paramount importance. The 5-year survival rate varies significantly depending on the stage at diagnosis, ranging from 57 % for localised-stage disease to 5 % for patients with metastatic disease.5 Notably, the incidence of LC continues to increase in Portugal in both sexes, representing the only cause of death that did not decrease during the recent COVID-19 pandemic.6
The two most efficient strategies for reducing LC mortality are i) decreasing tobacco consumption and exposure to second-hand tobacco smoke by implementing comprehensive tobacco control policies7 and ii) early diagnosis through Lung Cancer Screening (LCS) programs.8–10
As tobacco use remains the leading risk factor for LC, smoking cessation is a key strategy for preventing and managing LC.11 Tobacco control policies, such as raising tobacco taxes, creating comprehensive smoke-free environments, implementing large pictorial health warnings and plain packaging, running health campaigns, and providing a real and accessible offer of smoking cessation consultations are expected to have a significant population impact. This is especially relevant considering that 18.4 % of the European Union (EU)12 and 17.0 % of the Portuguese population are smokers.13 Tobacco control policies and LCS are synergistic and should be implemented together to maximise their population impact.
Several clinical trials have demonstrated that low-dose computed tomography (LDCT)for LCS effectively reduces LC mortality.8,10 This strategy can shift LC detection towards earlier stages, improving the survival rates and quality of life of participants diagnosed with LC through screening.16 In the National Lung Screening Trial (NLST), which enrolled 53,454 ever-smokers, LDCT was found to reduce LC mortality by 20 % and the all-cause mortality rate by 6.7 % compared to chest radiography.10 The Nederland–Leuven Longkanker Screenings Onderzoek (NELSON) trial, involving 13,195 men (primary analysis) and 2594 women (subgroup analyses) at high risk for LC, showed a 24 % cumulative reduction in 10-year LC mortality among the male screening group and a more significant cumulative risk reduction of 33 % among women when compared to the control group.8 In the most recent meta-analysis encompassing 94,837 participants from nine randomised controlled trials, LDCT screening showed a 16 % relative reduction in cancer mortality and a 3 % relative reduction in all-cause mortality.14
Furthermore, LCS has proven to be cost-effective in the European population, with an incremental cost-effectiveness ratio ranging between approximately €14,000 and €17,000 per additional quality-adjusted life years (QALY),15 a value lower than the Portuguese willingness to pay (€22,907/QALY, corresponding to Portuguese gross domestic product in 2022, according to Statistics Portugal).6
In 2022, the Council of the EU issued a press release regarding the European Program to Combat Cancer with a focus on early cancer detection. These recommendations aimed to increase the number of screenings and cover more target groups and cancers. Concerning LC, screening is recommended for individuals aged 50–75 years who are smokers and ex-smokers with a heavy smoking history. This recommendation emphasizes the importance of providing equal access to screening, timely diagnostic procedures, treatment, psychological support, and aftercare. To support this implementation, EU guidelines on cancer screening and treatment will be developed using financial support from EU4Health for lung, prostate, and stomach cancer.16
This position statement, developed by a comprehensive group of national medical experts, defined the requirements for LCS implementation in Portugal.
MethodsAfter the Council of the EU recommended that Member States explore the feasibility of LDCT for screening individuals at high risk for LC,16 the Portuguese Society of Pulmonology (SPP), in collaboration with the Portuguese Society of Radiology and Nuclear Medicine (SPRMN), the Portuguese Society of Oncology (SPO), the Group of Respiratory Diseases of the Portuguese Family Medicine Association (GRESP of APMGF), the Portuguese Society of Pathology (SPAP), and the Portuguese Society of Cardiac, Thoracic and Vascular Surgery (SPCCTV), has formed a task force. This task force includes pulmonologists, radiologists, oncologists, thoracic surgeons, public health experts, and family doctors. The initiative and the resulting document have received scientific endorsements from the aforementioned societies, as well as from the APMG, the Portuguese Lung Association (FFP), and the Portuguese Association of Persons with COPD (RESPIRA).
First, a comprehensive literature review was conducted. The Pubmed database was searched using the following keywords: (“LC screening” OR “LC early detection”) AND (“implementation LC screening” OR “LC screening programs” OR “adherence to LC screening” OR “effectiveness of LC screening”). This review included randomised controlled trials, clinical trials, meta-analyses, and systematic reviews written in English and published from 2010 until 2023. Two reviewers screened the titles and abstracts to determine their eligibility (further details are provided in Appendix A). The bibliography was completed using the articles suggested by experts in their respective fields. Of the 203 initially identified articles, 146 met the inclusion criteria. Subsequently, two independent reviewers read the full text of all articles and determined that 77 articles were relevant to this initiative. These relevant articles were then shared with all the task force members.
The WHO recommendations for screening programs were considered during the first task force meeting. Subsequently, a list of the core steps to be addressed in the implementation of a pilot LCS was created: Step 1 – Eligibility (identifying the eligible population for screening); Step 2 – Invitation (inform and invite the eligible population for screening; Step 3 – Testing (requirements and radiological protocol for low LDCT); Step 4 – Results (reporting screening results and appropriate referral of the cases); Step 5 – Diagnosis (diagnosis of positive screening test); Step 6 – Treatment (treatment of positive screening cases); Step 7 – Implementation (pilot testing, monitoring and evaluation of the program) and a transversal approach to all steps for Smoking Cessation Intervention.17 These steps are outlined in the headers below.
All members analysed the core steps. Topics without clear scientific evidence in the literature or cases of divergence were individually discussed and a consensus was reached within the panel of experts. The final recommendation was unanimously reached. All task force members have reviewed and approved the final version of this manuscript.
ResultsA description of the consensus reached by the task force for the core steps is provided below.
Step 1 – Identifying the eligible population for screening
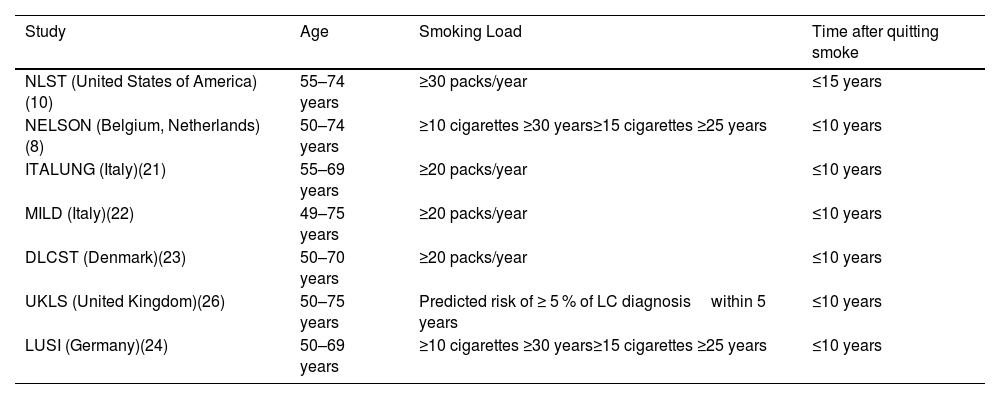
The eligibility criteria for screening were based on the previously published LCS clinical trials (Table 1).8,10,18–23
Inclusion criteria for large-scale randomized controlled lung cancer screening trials. LC – Lung cancer.
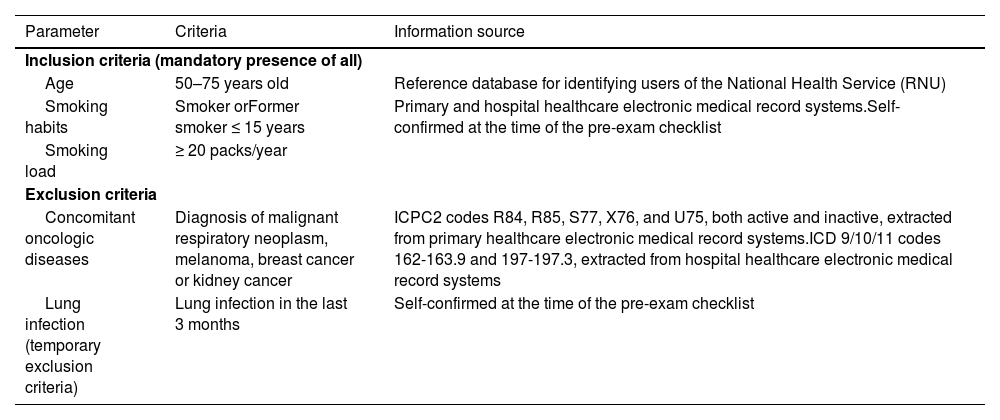
The inclusion and exclusion criteria for the Portuguese LCS and its source of information are described in Table 2.
Inclusion and exclusion criteria for the Portuguese lung cancer screening program and their respective sources of information. ICD – International Statistical Classification of Diseases and Related Health Problems; ICPC- International Classification of Primary Care; RNU – National Patient Registry.
The proposed screening age was inconsistent across published clinical trials (Table 1), with starting ages ranging from 49 to 55 years and the end of screening ranging from 69 to 75 years. Although a recent economic evaluation of the implementation of LCS showed that screening patients aged 50 years and older is cost-effective,15 a higher cost-effectiveness ratio is obtained as the maximum age decreases. Additionally, most European trials begin screening at 50 years of age. Therefore, the task force proposes a screening age group between 50 and 75 years.
Smoking statusA smoking load ≥20 pack years was chosen for tobacco consumption. Most European and worldwide studies have selected this cutoff value. However, it is worth noting that the NELSON trial did not use the terminology of pack years and defined different smoking loads according to the duration of smoking habits. This methodology is not compatible with the population-based LCS in Portugal, as the required information cannot be automatically retrieved from national data sources. Regarding ex-smokers, while the relative risk of LC decreases with the years since quitting, the risk of LC among those who have quit in the last 15 years remains high compared with never-smokers.24Therefore, the task force recommends screening smokers with a smoking history of ≥20 pack years and ex-smokers of less than 15 years with the same smoking history.
Exclusion criteria (permanent and temporary)The task force recommends that individuals with current or recent (within 5 years) treatment of advanced-stage non-lung cancer should not be included in a national LCS process.25 These particular populations are already subject to specific monitoring and have an increased risk of LC compared with the defined eligible population. Those with comorbid conditions that substantially limit life expectancy and those incapable of giving informed consent should also be excluded. Furthermore, screening should be postponed for at least 3 months if the person has symptoms of an active respiratory infection or a recent history of respiratory infection (e.g. pneumonia, tuberculosis, or viral infection) to reduce false-positive LDCT results.26
Source of informationThe selected sources are the most robust available. It should be highlighted that they only identify persons with a valid Sistema Nacional de Saúde (SNS) number and with a General Practitioner or Family Doctor attributed. According to the Transparency Portal of the National Health Service, about 10 % of the population may not fulfil these requirements, which may be a limitation, similar to what happens with other screening programs; for this reason, self-identification should be accepted.27
Step 2 – Invitation and Information
The ideal recruitment method is a matter of debate and can be highly resource-consuming.28–31
There is robust evidence from other implemented population-based screening programs that customised invitation letters are more effective when they include the following information: i) the patient´s name; ii) a comprehensive description of the screening program; iii) details about the inclusion and exclusion criteria; iv) information about the risks and benefits of patient participation in the screening program; v) a brief intervention promoting smoking cessation and referral to cessation programs; vi) a predefined date, time, and location for the screening test; and vii) an informed consent form. All documents must display the identification of the promoting entities. The screening program should also include an opt-out mechanism that allows individuals who do not wish to participate to inform the organisers of their decision.32
After receiving the invitation letter, individual participants should receive a confirmatory phone call from a dedicated healthcare professional affiliated with the screening program. This professional should conduct an eligibility assessment by applying a checklist that includes all inclusion and exclusion criteria. Additionally, the first screening round should be scheduled. It is important to note that a brief intervention for smoking cessation should be included during the phone call as part of the transversal smoking cessation approach.
Step 3 – Testing: Radiological requirements and protocols
The LDCT Protocol should be consistent and standardized across institutions and through the screening rounds.
Requirements for low dose computed tomographyAlthough the risk of radiation-induced cancer and the resulting mortality are low compared to the benefits of LDCT, the radiation dose should not be ignored, as the risk of radiation-induced cancer increases with the radiation doses used.33,34 The reliability and reproducibility of volumetric measurements depend on the appropriate and consistent use of acquisition and reconstruction parameters.35
To ensure the implementation of a reproducible screening program with sufficient image quality for the detection of small nodules while minimizing radiation dose, the following requirements must be met:
- •
Centre-related requirements: An experienced radiologist should lead the implementation and monitor screening tests.33,34
- •
Scanner-related requirements: A multi-detector row tomography equipment with 64 or more detector rows is preferable. If this is not possible, a 32-multidetector row equipment can be used.36 Using a mobile unit is an innovative practice already implemented in some countries that can provide added value by promoting adherence and ensuring equitable access to hard-to-reach populations.37
- •
Technical standards for examination technique: The LDCT Protocol recommended by the European Society of Thoracic Imaging (ESTI) is described in Appendix B.38
The volume of the nodules, rather than their diameters, should be measured. Nodule volume is a more reliable predictor of early growth and plays a crucial role in reducing false-positive results, defining optimal management of patients with lung nodules, and improving outcomes.39 Nodule volume measurement is currently recommended by the British Thoracic Society Guidelines, Fleishner Society Guidelines, European Position Statement Expert Group, and the latest version of Lung-RADS.40–42 When applied to the NLST with a threshold of 6 mm, Lung-RADS allowed a 52 % reduction in false positives and a recall rate reduction to 12.8 % versus 26.3 % in round 1, and had good acceptance among radiologists.43
We recommend the use of a structured report and the Lung-RADS classification for the conclusion of the LCS report to standardise reporting and management of abnormal findings detected in LDCT.42 Board-certified radiologists with experience in pulmonary nodule imaging should be encouraged to pursue LCS Certification.34
Given that the implementation of an LCS program results in a significant increase in the workload of radiologists with the need for detailed nodule assessments, including volume duplication time, artificial intelligence (AI) solution aid is now widely recognised as beneficial for LCS programs.44
Frequency and end of screeningThe optimal interval between two screening CT scans remains a subject of debate. In the NELSON trial, incremental intervals between screening tests were used: 1, 2, and 2 ½ years.8 When compared with the first round of screening (with a 1-year interval), the examination at 2 and ½ years resulted in a significantly lower detection rate of stage IA cancers (60.9% vs. 75.9 %, p = 0.02), a higher rate of stage IIIB/IV cancers (17.3% vs. 6.8 %, p = 0.02), and an increase in the number of interval cancers.45 Thus, a 2.5-year interval does not seem to be the most appropriate. The analysis of the two-year interval did not show a significant increase in the incidence of advanced stages compared to the 1-year interval (p = 0.09). However, there is insufficient evidence to support a 2-year interval.45
Therefore, the task force proposes a 1-year interval between two CT scans. This screening interval should be re-evaluated based on the diagnostic yield and incidence of interval cancers during the screening program and on the results of other studies that are currently underway. The screening should be continued as long as individuals meet the inclusion criteria.
Step 4 – Reporting and Referral of screening results
Screening results should inform the Lung-RADS classification and provide follow-up recommendations (Fig. 1).
Lung-RADS 1 or 2: negative screening test. CT – computed tomography.")
Negative screening results should be communicated to the patient via text message and to the family doctor via national electronic medical records. The next screening round should be automatically scheduled.
Lung-RADS 3 or 4: positive screening testPositive screening test results should be communicated to patients via text messages and written letters explaining the results. The results should also be sent to family doctors via national electronic medical records. Scheduling of additional examinations should be determined based on the results of the diagnostic workup outlined in Step 5.
Lung RADS S: other clinically significant findingsOther clinically significant findings should be communicated to the patient via text messages and to the family doctor via national electronic medical records.
Step 5 – Diagnosis
Individuals with a positive screening test (Lung-RADS 3 or 4) should be promptly referred to a specialised pulmonology consultation.
Patients with a Lung-RADS score 3 should repeat the CT scan after 6 months. If the size of the nodule does not increase on the subsequent CT scan, the patient should be reintegrated into the regular screening program. However, if suspicious findings are detected, the management protocol should follow the Lung-RADS 4 protocol.
Patients with a Lung-RADS score of 4 should be referred to a Multidisciplinary Team that may include Pulmonologists, Radiologists, Interventional Radiologists, and Thoracic Surgeons. The team should discuss the appropriate management strategy for the patient and establish a follow-up plan (Fig. 1).
Diagnostic strategies for establishing the diagnosis of lung cancer usually include transthoracic biopsies and or bronchoscopy.
Pulmonary nodes, mainly if peripheral, can be diagnosed with a transthoracic pulmonary biopsy, which has a very high diagnostic yield for malignancy, although with an overall pooled incidence for pneumothorax of 25.9 % and chest drain insertion of 6.9 %.46 Currently, there is a trend to combine lung cancer diagnosis with lymph node endosonographic guided using endobronchial ultrasound (EBUS) ± endoscopic ultrasound (EUS) for mediastinal staging in an all-in-one procedure. Solitary pulmonary nodules constitute a challenge for the bronchoscopist. The sensitivity of bronchoscopy in detecting malignancy is highly variable, depending on factors such as nodule size, the nodule´s relation to the bronchial wall, the presence of CT- bronchus sign, complementary use of image systems, operator skills, and the prevalence of cancer in the population being screened.47 Image-guided techniques, such as EBUS with radial probe, fluoroscopy, cone-beam and electromagnetic navigation bronchoscopy, facilitate sampling peripheral lesions and improve the detection of such lesions. Moreover, a better yield can be achieved with combined modalities. Robotic bronchoscopy is also a promising developing technology.
Bronchoscopic sampling methods can also be improved with the use of cryobiopsies, allowing for larger and better-preserved samples, alongside with conventional biopsies forceps, brushings, and washes.48
Step 6 – Treatment
It is crucial to ensure that all individuals who require treatment receive the best possible care within the specified timeframe, following the European Society for Medical Oncology guidelines adjusted to the National Authority of Medicines and Health Products (Infarmed) indications. Timely and equal access to thoracic surgery, radiotherapy, and systemic oncological treatments must be guaranteed.
Step 7 – Pilot Testing, Monitoring, and Evaluation
The task force recommends the implementation of a pilot LCS program in Portugal based on the established effectiveness and cost-effectiveness of LCS in populations with similar characteristics at an international level.
This pilot program is expected to be conducted in at least two distinct primary healthcare areas, following a population-based approach and the recommendations of this task force, as mentioned above. A random sample of the eligible population should be selected for this pilot study.
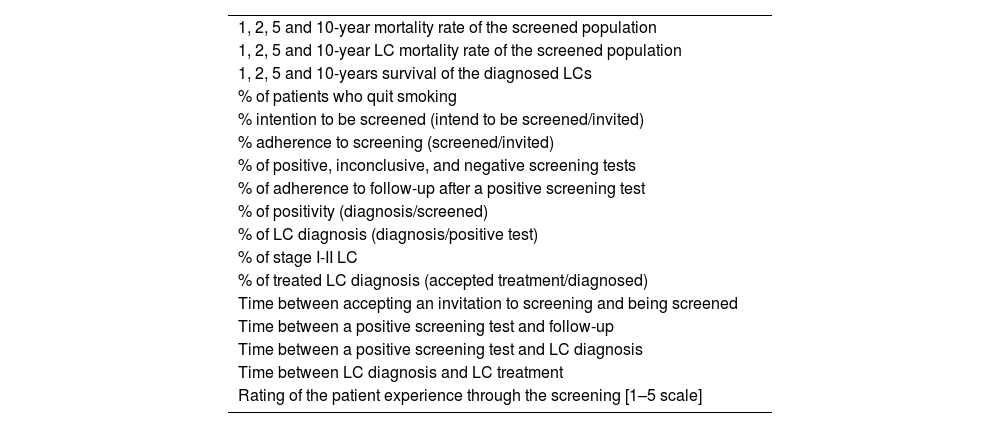
The monitoring strategy should include data collection on health outcomes and process indicators. Table 3 provides a brief overview of the indicators to be considered.
Proposed performance indicators. LC – lung cancer.
In a pilot screening program, it is advisable to compare the overall and the LC mortality rates of the screened population with the non-screened population in the same geographical area. Additionally, an economic evaluation of the screening project should be conducted using a decision-tree model to compare the cost-effectiveness of screening and non-screening in the Portuguese population, assuming high-quality patient-level data. The main outcome measures should be QALY and Disability-adjusted life-years (DALY) assessed for 5, 10, and lifelong years. Costs should be calculated from both the provider and societal perspectives.
Before the implementation of the screening in each centre, the designated interveners should be identified and trained for their respective tasks, including smoking cessation brief intervention. This training is essential to enhance the reproducibility and quality of the screening program.
The results of the pilot programs should guide the implementation of LCS at the national level, and any necessary adaptations of the proposed protocol should be made based on acquired knowledge.
Transversal approach – Smoking cessation intervention
Smoking cessation is the most cost-effective measure for reducing LC mortality7,49 and is associated with better therapeutic responses and fewer complications from chemotherapy, radiotherapy, and surgery.50
Around 40–60 % of individuals still smoke at enrolment, and many of them are highly nicotine-dependent,51 while ex-smokers undergoing LCS face a high risk of relapse.50,52 LCS programs offer a unique opportunity to promote motivation to quit, support quitting attempts, and prevent relapse toward sustained abstinence among high-risk smokers and ex-smokers.50,53 Pairing LCS with smoking cessation should be the standard of care in a high-quality screening program.50,54 as it can favour the balance between screening benefits and harm,55,56 promote participants' adherence to screening,60 and enhance its cost-effectiveness.56 Furthermore, smoking cessation interventions must be made available and encouraged at any time during screening programmes.
Tobacco and nicotine use are classified as chronic relapsing disorders that require a chronic disease approach involving diagnosis, evaluation, and repeated treatment until sustained abstinence is achieved. Therefore, it is crucial to provide training to healthcare providers (HCPs) to ensure a systematic approach to smoking cessation.57 Considering tobacco cessation guidelines, expert panel recommendations, and recent systematic reviews, subsequent strategies should incorporate LCS cessation interventions.50–53,55–60
- i)
All smokers and former smokers participating in the LCS should be strongly encouraged to quit or remain smoke-free at each visit, irrespective of their motivation to quit or screening results. It is essential to systematically record the patterns of tobacco/nicotine use and cessation advice.
- ii)
The LCS provider team should be trained to deliver brief evidence-based tobacco cessation advice (5 As/5 Rs model) and systematically emphasize the benefits of quitting. Advice should be tailored to age, sex, tobacco/nicotine use patterns, and specific clinical situations.
- iii)
For smokers unwilling to quit, motivational behavioural strategies, such as the 5Rs model, should be implemented during each visit to foster behavioural change.
- iv)
Smokers ready to quit should receive assistance or be referred to evidence-based cessation programmes. This can be done by the primary care team or other HCPs involved in LCS or by referral to external cessation programs, such as quit lines or intensive smoking cessation services.
- v)
Providing self-help leaflets or materials as a unique cessation strategy has limited efficacy in promoting abstinence.
- vi)
The most effective intervention, particularly for long-term and highly dependent smokers, involves intensive multicomponent treatment. This should encompass motivational strategies, high-intensity behaviour therapy with multiple counselling sessions, and pharmacologic treatment.
- vii)
The most effective pharmacotherapies are a combination of nicotine replacement therapy, varenicline or cytisine.
- viii)
Affordability of pharmacotherapy is mandatory to enhance treatment adherence and effectiveness.
- ix)
Treatment should include advice on exposure to second-hand smoke.
- x)
Regular follow-up to boost motivation and prevent relapse should be conducted systematically, and retreatment should be incorporated as needed.
This task force strongly recommends that LCS combined with evidence-based smoking cessation should be the standard care in a high-quality screening program.
Future research agendaFuture research projects should be designed to address knowledge gaps specific to the national context, including i) the development of predictive risk models for LC tailored to the Portuguese population; ii) exploration of biomarkers, with a preference for non-invasive options such as liquid biopsies; iii) investigation of recruitment strategies and screening intervals; iv) validation of deep learning algorithms in the application of AI to optimize screening classification; v) development of customized protocols for different types of nodules; vi) evaluation of the effectiveness of smoking cessation interventions and how to integrate smoking cessation in LCS settings/programs; vii) evaluation of LCS cost-effectiveness, viii) evaluation of the psychological and emotional impact of the screening on a sample of volunteers, their expectations of continuing to adhere to it, and the impact on their decision to keep/quit smoking and ix) to increase the health population's literacy
The role of AI in lung cancer screening has been a promising research area, with the potential to transform the effectiveness and efficiency of early detection processes significantly. The application of AI in lung cancer screening can occur at various stages, from identifying the target population, interpreting radiological images, analysing clinical data and personalizing screening strategies. However, the implementation of AI should be validated through robust clinical studies before becoming integrated into standard clinical practices, and always ensure data privacy.61
ConclusionsThere is an urgent need to implement the LCS in Portugal in accordance with European recommendations. This multidisciplinary task force has provided recommendations for the implementation of a national LCS program in Portugal. The target population for screening should include individuals aged 50–75 years with tobacco exposure of over 20 packs/year or those who have quit smoking for less than 15 years. Annual screening with LDCT is recommended if the inclusion criteria are met. Standardized LC reporting and use of the Lung-RADS classification for scoring pulmonary nodules are encouraged.
Combining LCS with evidence-based smoking cessation is crucial to increase adherence to screening and improve cost-effectiveness. This should be the standard of care in high-quality screening programmes. Prior to the implementation of screening at each centre, it is essential to identify and train all interveners in their respective roles, including brief interventions for smoking cessation. These recommendations are tailored to align the current clinical evidence with the Portuguese population and its healthcare system. The proactive adoption of these guidelines can significantly contribute to the success of a robust LCS program in Portugal.
FundingNo funding.
CRediT authorship contribution statementM.G.O. Fernandes: Conceptualization, Methodology, Writing – review & editing, Validation. M. Dias: Conceptualization, Methodology, Writing – review & editing, Validation. R. Santos: Conceptualization, Methodology, Writing – review & editing, Validation. S. Ravara: Conceptualization, Methodology, Writing – review & editing, Validation. P. Fernandes: Conceptualization, Methodology, Writing – review & editing, Validation. J. Firmino-Machado: Conceptualization, Methodology, Writing – review & editing, Validation. J.P. Antunes: Conceptualization, Methodology, Writing – review & editing, Validation. O. Fernandes: Supervision, Validation. A. Madureira: Supervision, Validation. V. Hespanhol: Supervision, Validation. C. Rodrigues: Supervision, Validation. C.A. Vicente: Supervision, Validation. S. Alves: . G. Mendes: Supervision, Validation. R. Ilgenfritz: Supervision, Validation. B.S. Pinto: Supervision, Validation. J. Alves: Supervision, Validation. I. Saraiva: . C. Bárbara: Supervision, Validation. M.A. Cipriano: Supervision, Validation. A. Figueiredo: Supervision, Validation. M.S. Uva: Supervision, Validation. N. Jacinto: Supervision, Validation. L. Curvo-Semedo: Supervision, Validation. A. Morais: Conceptualization, Methodology, Writing – review & editing, Supervision, Validation.

- 1)
Participant-related requirements:
- •
Positioning: The chest must be in the centre of the gantry; table height and centring adjusted so that the midaxillary line is at the isocentre; arms overhead – supine.
- •
Training: Instructions regarding remaining still and breathing (inspiratory apnoea) should be provided.
- •
Localizer: restricted to the chest; Inspection for external objects.
- •
Anatomical coverage: It is recommended to limit coverage as much as possible to cover the entire lung volume from the apex through the lung base.
- •
Gantry tilt: none
- •
Scan duration: A shorter scan duration of less than 10 s is preferred within a single breath-hold at maximum inspiration (inspiratory apnoea).
- •
A display Field of View (FOV) of 1 cm beyond the rib cage is recommended; there is no need to include the entire chest wall thickness; a smaller FOV indicates a smaller voxel size and better volumetry.
- •
- 2)
Image acquisition-related requirements:
- •
Contrast: no IV or oral contrast.
- •
kVp: 100–120 acceptable for standard-sized participants, and 140 acceptable for obese participants. mAs should be reduced first, followed by kVp. Strong beam-hardening prefiltering (e.g. Sn filtering) is strongly recommended.
- •
Tube Current (mA) should be set in combination with kVp and pitch.
- •
Adjustment of scanner output for participant size: No fixed mAs setting unless at a very low dose (0.5 mGy).
- •
Therefore, tube current modulation is recommended. This should consider the participantʼs body habitus, age, slice width, kVp, and the unique attributes of the scanner and acquisition mode.
- •
Noise level should ensure the diagnostic quality of lung parenchyma and accurate volumetric measurement.
- •
Use of automatic exposure controls including tube current modulation and automated kV selection tools.
- •
Use of organ dose modulation, if available, is recommended.
- •
Maximum Tube Rotation Time should be ≤ 0.5 s.
- •
The pitch (IEC Definition) should be vendor-suggested and set with other technical parameters to achieve the CTDIvol specifications.
- •
Reconstructed image width (nominal width of the reconstructed image along the z-axis) is preferably ≤0.75 mm or smaller, or at least ≤1 mm. In very obese 1.25 mm may be necessary.
- •
Slice Interval should be at a maximum of 0.7 mm, ≤ slice width. Overlapping reconstructions are not mandatory. Reconstruction kernel: Standard body kernel. An additional lung kernel was also proposed.
- •
Reconstruction algorithm: iterative reconstruction or deep learning reconstruction is recommended.
- •
Use of filtered back projection reconstruction algorithms is strongly discouraged.
- •


