

The most recent guidelines on asthma and rhinitis management recommend the optimal control of both diseases as the primary goal of treatment. CARAT10 is a recently developed and validated Portuguese questionnaire, which permits the simultaneous assessment of allergic rhinitis and asthma (ARA) control. There is no published data about the use of this tool.
AimsTo assess ARA control using CARAT10 in an Immunoallergology hospital setting.
MethodsPatients with diagnosis of allergic rhinitis with or without asthma (positive aeroallergens prick-tests and/or positive specific IgE) were sequentially enrolled and asked to fill in CARAT10 questionnaire at their first appointment.
ResultsTwo hundred patients were included, mostly female (n=142) with an average age of 33.6±12.3 years. ARA was present in 86 patients while 114 had isolated allergic rhinitis. In ARA group, 86% scored CARATtotal ≤24, meaning poor control. Subscores revealed that 83% had poorly controlled rhinitis (CARATr ≤8) and 74% had poorly controlled asthma (CARATa <16). There were no age or gender related differences in ARA control. In allergic rhinitis group (n=114), 89% were poorly controlled.
ConclusionsOnly 14% of patients presenting rhinitis and asthma had both diseases controlled.
As últimas guidelines para o tratamento da asma e rinite recomendam o controlo otimizado de ambas as doenças como objetivo primário da terapêutica. O questionário CARAT10 foi recentemente desenvolvido e validado em Portugal e permite a avaliação simultânea do controlo da rinite e da asma alérgicas (RAA). Não existem estudos previamente publicados sobre a utilização deste instrumento de avaliação.
ObjetivoAvaliar o controlo da RAA usando o questionário CARAT10 em consulta hospitalar de Imunoalergologia.
MétodosDoentes com o diagnóstico médico de rinite com ou sem asma alérgica (testes cutâneos para aeroalergénios e/ou IgE específicas positivas) foram sequencialmente incluídos e preencheram o questionário CARAT10 na primeira consulta hospitalar de Imunoalergologia.
ResultadosForam incluídos 200 doentes, a maioria do sexo feminino (n=142) com uma idade média de 33,6±12,3 anos, 86 apresentavam RAA e 114 rinite alérgica isolada. No grupo de doentes com RAA, 86% obtiveram uma pontuação no CARATtotal ≤ 24, significando mau controlo. As pontuações parciais do CARAT revelaram que 83% apresentavam rinite não controlada (CARATr ≤ 8) e 74% asma não controlada (CARATa < 16). Relativamente ao escalão etário e ao género, não se verificaram diferenças significativas no que diz respeito ao controlo da RAA. No grupo com rinite alérgica isolada (n=114), 89% apresentavam mau controlo da doença.
ConclusãoApenas 14% dos doentes apresentaram rinite e asma alérgicas controladas.
Allergic rhinitis and asthma are both immunologically mediated diseases.1 Their burden is high, having a strong impact on the individual life quality and in society.2 Approximately 80% of asthmatic patients have rhinitis and about 10–40% of patients with rhinitis have asthma.3 In the natural evolution of respiratory allergic disease, rhinitis often precedes the development of asthma,4 strengthening the theory “one airway, one disease”.3 Allergic rhinitis (AR) and allergic asthma (AA) may be seen as two presentations or phenotypes of the same disease sharing common physiopathological mechanisms. The guidelines on the management of Allergic Rhinitis and its Impact on Asthma (ARIA 2008) recommend the optimal control of both diseases as the primary goal of treatment.5 The Global Initiative for Asthma (GINA 2011) reinforces therapy guidance according to disease control.6 Consequently, the need for tools that simultaneously assess the control of both diseases becomes increasingly relevant.
The first tool created for rhinitis and asthma was RINASTHMA, a quality of life questionnaire.7 Recently, a symptom questionnaire named CARAT10 (Control of Allergic Rhinitis and Asthma Test) was created and validated in Portugal.8 This questionnaire (available online at www.caratnetwork.org) is simple and self-administered by the patient taking into account the previous 4 weeks. To the best of our knowledge there is no published data regarding the use of this tool in the assessment of allergic rhinitis and asthma (ARA) control.
Our aim was to determine ARA control in patients referred to an Allergy outpatient hospital clinic setting using CARAT10.
MethodsThis cross sectional study was conducted at the outpatients Allergy Unit of Hospital Pedro Hispano, in Matosinhos, over two periods, from May to July and from October to December 2011. Matosinhos is a seaside city with approximately 175478 inhabitants. The Allergy Unit is responsible for about 1024 appointments per year (41% of those are first appointments). Most patients are referred from primary care units; approximately one-third is referred from hospital specialties like Otorhinolaryngology, Pediatrics, Pneumology and Internal Medicine. Most often patients have suspected to have respiratory allergic disease, urticaria and angioedema, atopic eczema, food or drug allergy.
Patients over 15 years of age who were referred to the Allergy Unit during the study period with medical diagnosis of allergic rhinitis or allergic rhinitis and asthma were included. Exclusion criteria were subjects younger than 15 years of age, presence of other morbidities (diabetes mellitus, liver disease, cardiovascular disease) and pregnant women. Patients were sequentially included during the study period and asked to fill in CARAT10 questionnaire during their first appointment at the hospital. Primary outcome was the score of CARAT questionnaire; secondary outcomes were asthma severity and atopy status, differences in asthma control between gender and age classes.
CARAT questionnaire is composed of 10 questions; each question with 4 possible answers (scale 0–3) and the total score varies from 0 to 30. A CARATtotal ≤24 means poor disease control. The first four questions evaluate rhinitis (CARATr) and the last six questions evaluate asthma (CARATa). Scores CARATr ≤8 and CARATa <16 mean poorly controlled rhinitis and asthma, respectively. Allergic rhinitis diagnostic criteria were: ≥2 nasal symptoms (rhinorrea, nasal pruritus or congestion) when associated with specific precipitants and in the presence of atopy (positive prick-test wheal ≥3mm than negative control and/or IgE positive measurement). Asthma diagnostic criteria were based on suggestive clinical features (dyspnea, wheezing, chest tightness, cough), airway obstruction reversibility demonstrated by an increase of 12% and 200mL after the administration of a short-acting bronchodilator and/or positive metacoline bronchoprovocation test, according to American Thoracic Society guidelines.9 At the first appointment patients were diagnosed with rhinitis and/or allergic asthma, performed skin prick tests and filled in CARAT questionnaires. When necessary additional functional respiratory tests and bronchoprovocation were carried out a posteriori to confirm asthma diagnosis. The investigator determining rhinitis and asthma diagnosis was blinded to CARAT questionnaires results.
Asthma severity was classified according to previous GINA severity classification as intermittent, mild, moderate and severe persistent asthma.6
Questionnaires with missing data were excluded from the analysis.
Scores of CARATtotal, CARATr and CARATa were calculated in the group of patients with ARA and CARATr subscore was calculated in the group of patients with isolated allergic rhinitis. CARATtotal score was analyzed by gender (parametric t-test for independent samples) and age (non-parametric Kruskal–Wallis test for independent samples) using Statistical Package for Social Sciences 20.0. Statistical power was calculated based on test of one proportion with significance level of 0.05 using Lenth, R. V. (2006-9) Java Applets for Power and Sample Size software. Statistical power calculated based on an estimated proportion of 0.5 was 0.95.
ResultsDuring the study period 435 patients were observed at the Allergy Unit. From the 206 patients with medical diagnosis of allergic rhinitis and allergic rhinitis and asthma, 200 were included; one patient was excluded due to pregnancy; two patients were not able to fill in the questionnaire because of difficulty in interpreting the questions, and three had not filled in the questionnaire completely.
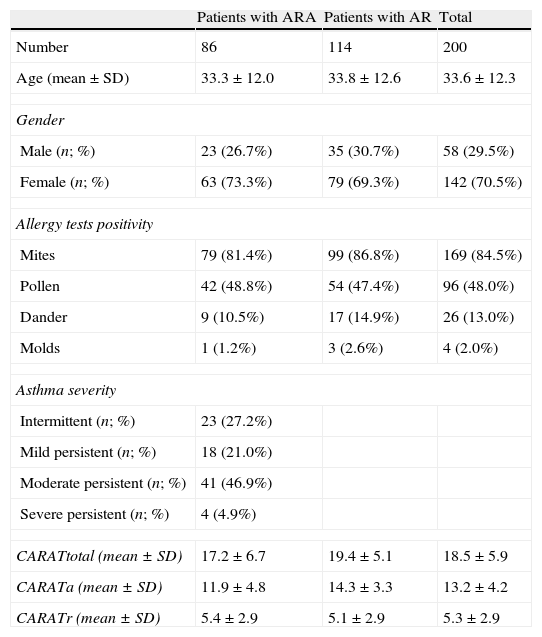
Out of the total of 200 patients included, 142 (71%) were female. The average age±SD was 33.6±12.3 years (minimum: 15; maximum 81). ARA was present in 43% (n=86) of the patients and the remaining 57% (n=114) had isolated allergic rhinitis. Asthma diagnosis was based on a suggestive clinical history in 20 patients with normal spirometry, on airway obstruction reversibility in 55 patients and on positive metacoline bronchoprovocation test in 11 patients. Patient characterization is displayed in Table 1.
Patients characterization (n=200).
| Patients with ARA | Patients with AR | Total | |
| Number | 86 | 114 | 200 |
| Age (mean±SD) | 33.3±12.0 | 33.8±12.6 | 33.6±12.3 |
| Gender | |||
| Male (n; %) | 23 (26.7%) | 35 (30.7%) | 58 (29.5%) |
| Female (n; %) | 63 (73.3%) | 79 (69.3%) | 142 (70.5%) |
| Allergy tests positivity | |||
| Mites | 79 (81.4%) | 99 (86.8%) | 169 (84.5%) |
| Pollen | 42 (48.8%) | 54 (47.4%) | 96 (48.0%) |
| Dander | 9 (10.5%) | 17 (14.9%) | 26 (13.0%) |
| Molds | 1 (1.2%) | 3 (2.6%) | 4 (2.0%) |
| Asthma severity | |||
| Intermittent (n; %) | 23 (27.2%) | ||
| Mild persistent (n; %) | 18 (21.0%) | ||
| Moderate persistent (n; %) | 41 (46.9%) | ||
| Severe persistent (n; %) | 4 (4.9%) | ||
| CARATtotal (mean±SD) | 17.2±6.7 | 19.4±5.1 | 18.5±5.9 |
| CARATa (mean±SD) | 11.9±4.8 | 14.3±3.3 | 13.2±4.2 |
| CARATr (mean±SD) | 5.4±2.9 | 5.1±2.9 | 5.3±2.9 |
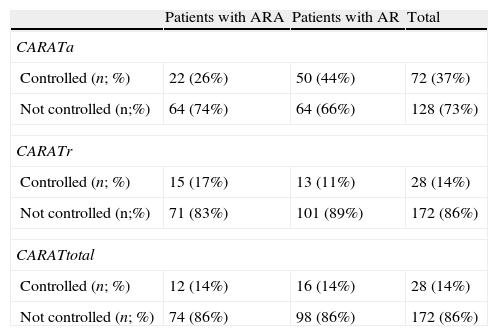
In the group of patients with ARA (n=86), CARAT total mean±SD was 17.2±6.7; CARATr was 5.4±2.9 and CARATa was 11.9±4.8. In this group, 14% (n=12) scored CARATtotal >24, meaning well-controlled disease while the remaining majority presented poorly controlled disease. These results and those related to CARATr and CARATa subscores are shown in Table 2.
Disease control in patients allergic rhinitis and asthma (n=86), allergic rhinitis (n=114) and in total sample (n=200).
| Patients with ARA | Patients with AR | Total | |
| CARATa | |||
| Controlled (n; %) | 22 (26%) | 50 (44%) | 72 (37%) |
| Not controlled (n;%) | 64 (74%) | 64 (66%) | 128 (73%) |
| CARATr | |||
| Controlled (n; %) | 15 (17%) | 13 (11%) | 28 (14%) |
| Not controlled (n;%) | 71 (83%) | 101 (89%) | 172 (86%) |
| CARATtotal | |||
| Controlled (n; %) | 12 (14%) | 16 (14%) | 28 (14%) |
| Not controlled (n; %) | 74 (86%) | 98 (86%) | 172 (86%) |
Asthma severity is displayed in Table 1. More than half of the patients had moderate or severe persistent asthma. Most patients were house dust mites sensitized, 70 patients were polysensitized to house dust mites and pollens.
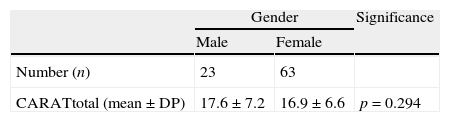
There were no gender or age related differences in the control of ARA (Table 3). CARATtotal score tended to be higher in men than in women (mean±SD, 17.6±7.2 and 16.9±6.6, respectively). CARATtotal score was not statistically different within age groups.
Gender and age differences in ARA control.
| Gender | Significance | ||
| Male | Female | ||
| Number (n) | 23 | 63 | |
| CARATtotal (mean±DP) | 17.6±7.2 | 16.9±6.6 | p=0.294 |
| Age groups (n) | CARATtotal (mean±SD) | |
| 15–19 (8) | 20.4±3.2 | p=0.306 |
| 20–24 (18) | 17.0±6.2 | |
| 25–29 (9) | 19.7±5.7 | |
| 30–34 (15) | 15.7±7.8 | |
| 35–39(13) | 17.5±6.7 | |
| 40–49 (15) | 15.7±5.8 | |
| >50 (8) | 17.9±9.5 |
Only 14% of patients of our sample had their rhinitis and asthma controlled. Most patients had persistent and severe asthma requiring daily medication. Although there are no published studies using CARAT, the low control rate is similar to those found in two unpublished studies. In one study, developed in three primary care units, only 3% of the patients with ARA (n=64) had both diseases controlled.10 Another study,11 performed in a community pharmacy involving patients (n=224) with specific prescriptions for asthma, showed a control rate of 13.4%, very similar to that found in our study. Nevertheless, this is the first study addressing CARAT results at the first appointment in a specialized Allergy Unit setting. The fact that it is a first time evaluation may explain the poor control results reflecting a previously non-optimized therapy or even because of more severe disease (according to asthma control national guidelines patients with more severe disease are recommended to be referred to specialized care units where complementary diagnostic and therapeutic options are available).12
When subscores are analyzed, asthma is better controlled than rhinitis with control rates of 26% and 17%, respectively. In addition, individual disease control is better than the overall control. According to Domingues,10 asthma control evaluated by other asthma control questionnaires such as Asthma Control Test tends to be higher than when evaluated by CARAT in the same population, though exhibiting high correlation. We may hypothesize that low overall control rates with CARAT10 may be due to the influence of CARATr subscore, emphasizing the fact that rhinitis control is of particular relevance. In relation to patients with isolated allergic rhinitis (n=114), only 11% were controlled. At present, there are some tools still in development to assess rhinitis control, so it is not possible to compare these results with other studies.
When compared with other national studies our sample has fewer asthmatic patients with intermittent disease and more patients with moderate-severe persistent asthma.13
Regarding atopy results most patients were house dust mites sensitized as described in the literature.14 There was a female dominance in the studied population; however these results are not in agreement with previous studies which show a similar asthma prevalence in the two genders.15,16 Some studies suggest that ARA control is superior in men than in women, though studies evaluating AR are lacking. The reasons for this difference are not fully understood, but disparities in dyspnea perception, with women being more aware of dyspnea than men, may explain the difference.15,16 However, our study like others17,18 showed up no gender related differences in ARA control. Despite the fact that several studies did show worse disease control in older patients,17–19 our study did not corroborate this trend, since CARATtotal scores presented no significant differences among the different age groups (p=0.306).
Other variables influencing asthma control such as smoking habits, obesity or ongoing therapy were not taken into account and could have contributed to a better interpretation of results.
In the future, it would be interesting to re-evaluate this group of patients after a follow-up period and prospectively compare CARAT scores.
ConclusionAllergic rhinitis and asthma control assessed by CARAT10 questionnaire was very poor in our sample.
The use of validated Portuguese tools to assess both rhinitis and asthma control should be encouraged since disease control is, according to recent guidelines, one of the most important factors for therapy guidance.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to acknowledge CARAT team (http://www.caratnetwork.org) for their support regarding CARAT questionnaire.
Please cite this article as: Pereira P. Ricardo, Lopes C. Estudo transversal da avaliac¸ão do controlo da rinite e asma alérgicas em consulta hospitalar de Imunoalergologia através do questionário CARAT10. Rev Port Pneumol. 2013. doi:10.1016/j.rppneu.2013.01.004.


