

Environmental tobacco smoke (ETS) is currently the main indoor pollutant and causes a high morbility and mortality. A partial restriction came into force in Portugal, in 2008, law 37/2007, trying to control, define and regulate smoke-free environments.
ObjectiveTo assess exposure and perceived impact of the law 37/2007 on exposure to ETS among adults attending to the two healthcare facilities of Chaves (Portugal).
MethodA cross-sectional survey on tobacco consumption and exposure to ETS was undertaken in Chaves (Northern Portugal) between November 2009 and February 2010. All the patients, over 17, attending to any of the Chaves Primary Care Facilities were interviewed. Patient enrolment was done on a rolling basis covering all days of the week. A face to face interview was carried out and a carbon monoxide was measured. Prevalence and means are shown with 95% confidence intervals.
Results287 patients participated in the survey, 56% were males and the mean age was 54 years. Smoking prevalence was 23.6%, significantly higher in males (31% vs. 17%). 46.2% reported exposure tobacco smoke elsewhere (53% in males vs. 40% in females). Smokers declared to be more exposed to ETS than non-smokers. 16.2% of the population declared to be exposed at home, 14% at work and 33% at leisure places. The highest decrease in perception of passive exposure was found for restaurants (95%). In nightclubs 68% of the participants stated that exposure has remained unchanged.
ConclusionThe tobacco control law offered protection against tobacco smoke in several closed public spaces. However, a significant proportion of the population remains exposed. This study highlights the ineffectiveness of a partial ban. A comprehensive law is, therefore, required in Portugal.
O fumo ambiental do tabaco (FAT) é atualmente o principal poluente do meio interior e responsável por uma elevada morbilidade e mortalidade. Uma restrição parcial foi introduzida em Portugal, em 2008, a Lei 37/2007, para tentar controlar, definir e regular ambientes livres de fumo.
ObjetivoAvaliar a exposição e a perceção do impacto da Lei 37/2007 sobre a exposição ao FAT em adultos atendidos em 2 centros de saúde em Chaves (Portugal).
MétodoUm estudo transversal sobre o consumo de tabaco e a exposição ao FAT foi realizado em Chaves (norte de Portugal) entre novembro de 2009 e fevereiro de 2010. Todos os pacientes, com mais de 17 anos, foram atendidos em um dos 2 Centros de Saúde de Chaves. A recolha de dados dos pacientes foi feita em uma base aleatória, abrangendo todos os dias da semana. Foi efetuada uma entrevista cara-a-cara e foi medido o monóxido de carbono exalado. Prevalências e médias foram analisadas para um intervalo de confiança de 95%.
ResultadosDos 187 pacientes participantes na pesquisa, 56% eram do sexo masculino e apresentavam uma média de idades de 54 anos. A prevalência de fumadores foi de 24%, significativamente maior nos homens (31 vs. 17%). 46,2% referiram estar expostos ao fumo de tabaco em todos os lugares estudados (53% nos homens vs. 40% nas mulheres). Os fumadores declararam estar mais expostos ao FAT em relação aos não fumadores. 16,2% da população estavam expostos em casa, 14% no trabalho e 33% nos lugares de lazer. A maior diminuição da perceção de exposição passiva encontrou-se nos restaurantes (95%). Nas discotecas, 68% dos participantes afirmaram que a exposição se manteve inalterada.
ConclusãoA lei antitabaco pretende oferecer proteção contra o fumo do tabaco em vários espaços públicos fechados. No entanto, uma percentagem significativa da população permanece exposta. Este estudo destaca os perigos de uma proibição parcial. Uma lei abrangente é, portanto, necessária em Portugal.
In 2006, the Surgeon General Report “The Health Consequences of Involuntary Exposure to Tobacco Smoke” concluded that there was a causal relationship between environmental tobacco smoke (ETS) exposure in non-smokers and several diseases such as lung cancer and coronary heart disease.1 Nowadays exposure to ETS is the 3rd cause of preventable death in some countries, after active smoking and alcohol consumption2 In Spain, López et al.3 estimated 1228 deaths attributable to ETS exposure among non-smokers in 2002. Nevertheless in several countries the burden of disease related to exposure to ETS remains unknown since the prevalence of exposure is unknown.
In response to the globalization of tobacco use and in recognition of its serious health effects on smokers and non-smokers, World Health Organization (WHO) conducted in February 2006 the first session of the Framework Convention on Tobacco Control, where the development of guidelines for protection against exposure to ETS was decided (Article 8).4,5 Ireland was the first European country to implement restrictions on tobacco consumption not only in public spaces such as nightclubs, bars and restaurants but also in workplaces. Since then, legislation banning smoking in indoor premises has been passed in Italy, Malta, Norway, Spain, Sweden and the United Kingdom. In January 2008 Portugal introduced law against ETS which was not comprehensive, law 37/2007 of 14 August.6 Some aspects regulated by this law include public awareness and health education, a ban on advertising tobacco products and prohibition of tobacco sales to minors. The law banned smoking in workplaces and in enclosed public places. But, against WHO recommendations’ of “100% smoke-free” policies, this “partial smoke-free law” allows the creation of identified smoking areas, mainly in recreational venues, separated by physical barriers from the non-smoking sections.
The aim of this study is to assess perceived exposure to ETS in Chaves (Portugal) after the ban implementation and to evaluate its impact on the self reported exposure to ETS.
Materials and methodsA cross-sectional survey on tobacco use and exposure to ETS was undertaken in Chaves between November 2009 and February 2010. Chaves is an inland region located at the North of Portugal, bordering Spain, with a population of 49,000 inhabitants, 9% younger than 15, and mainly agricultural workers. The reference population for this study was people attending to the Chaves Primary Health Care Facilities (Centro de Saúde de Chaves n° 1 e 2). Participants’ enrolment was consecutive; all the patients attending to the Cardiac-respiratory physiologist with an appointment in different days during the study period were selected. The patients were invited to participate on a rolling basis covering all days of the week in both Health Care Facilities. A face to face interview was completed prior to their visit with the general practitioner (GP). Inclusion criteria was being older than 17 and exclusion criteria was being unable to hold a conversation. A validated questionnaire7 derived from Spanish studies and adapted to the Portuguese context was used. The interviewee was asked about smoking history, tobacco labor consumption (cigars, cigarettes and pipes), nicotine dependence, change process, relapses or cessation motivation. They were also asked if they were current (daily or occasional), former or never smokers. Daily smokers were defined as individuals who smoke cigarettes regularly, i.e., at least one cigarette per day. In order to check self-declaration on tobacco consumption, a CO measure on expired air was performed, and a cut-off of 6ppm was established in order to distinguish smokers from non-smokers.8 Exposure to ETS (place and intensity of exposure) and perception of the impact of the law on exposure to ETS were also evaluated. To assess prevalence of exposure to ETS, several questions regarding frequency, place and timing were included. Prevalence of exposure during the previous week (from Monday to Sunday) was assessed by the question “how often do you think you have been exposed to smoke of smokers (in non-smokers) or of other smokers (in smokers) at (home/work/leisure time)”. Home and work exposure consisted of 3 possible answers: Daily, occasionally and never; and leisure time exposure included the option “Did not go out”. Exposure at work or school was ascertained only in workers or students. Length of exposure was assessed through the number of hours exposed per day (daily exposed) or per week (occasionally exposed). To ascertain a change in exposure to ETS as a consequence of the law, the following question was included: In comparison to 2007, previously to the smoke-free law, is your exposure to tobacco smoke at [home/work/bars or cafes/restaurants/discos] nowadays [higher than/similar to/less than] the pre law period? The options “I did not go out” and “I was not working” were included when questions were related to leisure places and work, respectively. Demographic characteristics, such as sex, age, labor situation, marital and educational status, were also collected. Education was classified in 4 categories according to the highest level completed by the participant. Basic level included population with less than 5 years of education, primary a minimum of 5 and a maximum of 9, secondary up till 12 or people that had completed a professional level and higher education included university degree.
Participants signed the informed written consent. The study was approved by the Ethics Committee of the Regional Health Administration from Portugal North (ARSN).
Quantitative and qualitative variables were described using means or prevalence and 95% confidence intervals (95% CI) were calculated. A bivariate analysis was performed and chi-square/exact fisher tests and t-student/Mann–Whitney U tests were applied to compare groups where appropriate. To validate the correlation between smoking and the concentration of CO the Cohen's Kappa was applied. For interpreting the results we used the Landis and Koch criteria.9 Data were analyzed with Stata version 10.0.
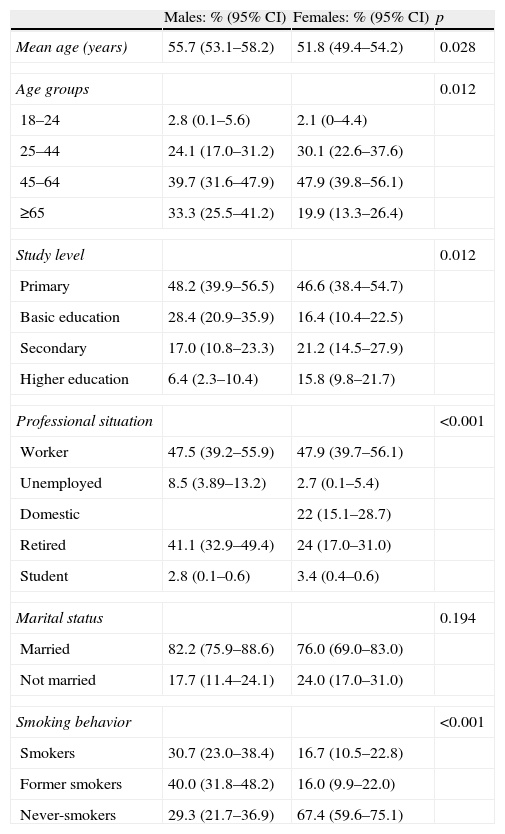
ResultsParticipants287 individuals were interviewed, 141 males and 146 females. Participant's characteristics are shown in Table 1. Population under 25 years accounts for only 2% of the interviewees and the age range was 19–86. Being retired was more frequent in males, and females had a higher educational level. Domestic work was exclusive among females.
Participant's sociodemographic characteristics and smoking status by sex.
| Males: % (95% CI) | Females: % (95% CI) | p | |
| Mean age (years) | 55.7 (53.1–58.2) | 51.8 (49.4–54.2) | 0.028 |
| Age groups | 0.012 | ||
| 18–24 | 2.8 (0.1–5.6) | 2.1 (0–4.4) | |
| 25–44 | 24.1 (17.0–31.2) | 30.1 (22.6–37.6) | |
| 45–64 | 39.7 (31.6–47.9) | 47.9 (39.8–56.1) | |
| ≥65 | 33.3 (25.5–41.2) | 19.9 (13.3–26.4) | |
| Study level | 0.012 | ||
| Primary | 48.2 (39.9–56.5) | 46.6 (38.4–54.7) | |
| Basic education | 28.4 (20.9–35.9) | 16.4 (10.4–22.5) | |
| Secondary | 17.0 (10.8–23.3) | 21.2 (14.5–27.9) | |
| Higher education | 6.4 (2.3–10.4) | 15.8 (9.8–21.7) | |
| Professional situation | <0.001 | ||
| Worker | 47.5 (39.2–55.9) | 47.9 (39.7–56.1) | |
| Unemployed | 8.5 (3.89–13.2) | 2.7 (0.1–5.4) | |
| Domestic | 22 (15.1–28.7) | ||
| Retired | 41.1 (32.9–49.4) | 24 (17.0–31.0) | |
| Student | 2.8 (0.1–0.6) | 3.4 (0.4–0.6) | |
| Marital status | 0.194 | ||
| Married | 82.2 (75.9–88.6) | 76.0 (69.0–83.0) | |
| Not married | 17.7 (11.4–24.1) | 24.0 (17.0–31.0) | |
| Smoking behavior | <0.001 | ||
| Smokers | 30.7 (23.0–38.4) | 16.7 (10.5–22.8) | |
| Former smokers | 40.0 (31.8–48.2) | 16.0 (9.9–22.0) | |
| Never-smokers | 29.3 (21.7–36.9) | 67.4 (59.6–75.1) | |
Prevalence of smokers was 23.6% (95% CI 18.6–28.6), 27.8% (95% CI 22.6–30.1) were former smokers and 48.6% (95% CI 42.7–54.4) declared that they never smoked. Prevalence of smokers was almost twice in males in comparison to females (31% vs. 17%) and the percentage of never smokers females was double than in males (Table 1).
There was a strong association between self-reported tobacco consumption and CO measures (k=0.89, 95% CI 0.83–0.95). Only 5 smokers, out of 216, had a CO concentration minor to 6 and 6, of 68 never or former, above 6.
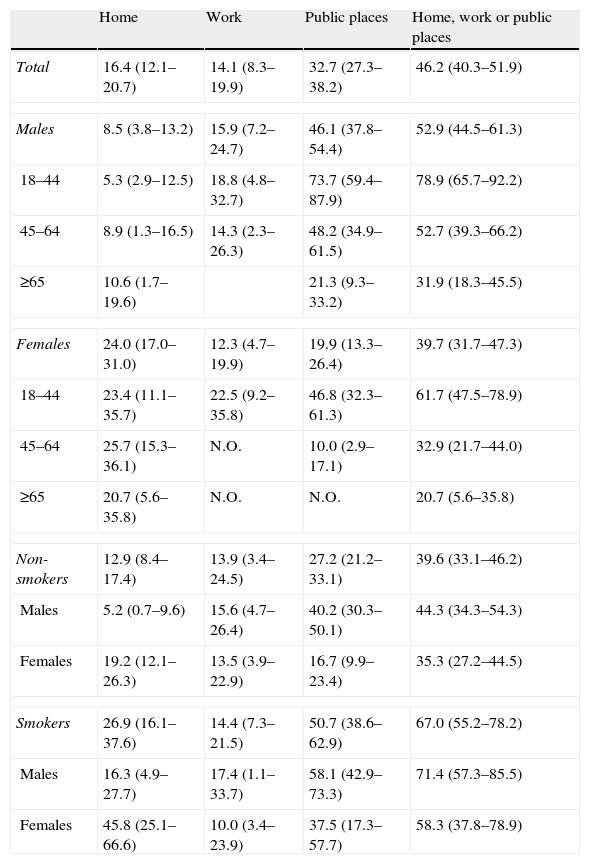
Prevalence of exposure to ETSResults indicate that 46.2% (95% CI 40.3–51.9) of the population were exposed to ETS, and the prevalence of exposure was highest in leisure time venues (as bars, pubs or discotheques). Males declared themselves to be more exposed than females (p=0.026) and smokers reported a higher passive exposure in relation to non-smokers (p<0.001). Prevalence of exposure decreased with age, so the population aged 18–44 declared themselves to be the most exposed (p<0.005) (Table 2). Prevalence of passive exposure at home was three times higher for females than for males (24% vs. 8.5%), p<0.001. Adults declared being exposed to ETS at home a mean of 20hours per week (95% CI 16.0–24.1) with no differences related to sex (p=0.45). Taking into account that during the month prior to the interview, 79 participants (mainly females and population over 64) did not go to leisure venues, the prevalence of exposure to ETS among males was higher than among females (46.1% vs. 19.9); p<0.001. Mean length of exposure at leisure time was 6.5hours (95% CI 3.5–9.5) per week without significant differences by sex (p=0.274).
Prevalence of exposure to ETS in three settings. Data are presented as % (95% confidence intervals). Exposure at work, only among workers.
| Home | Work | Public places | Home, work or public places | |
| Total | 16.4 (12.1–20.7) | 14.1 (8.3–19.9) | 32.7 (27.3–38.2) | 46.2 (40.3–51.9) |
| Males | 8.5 (3.8–13.2) | 15.9 (7.2–24.7) | 46.1 (37.8–54.4) | 52.9 (44.5–61.3) |
| 18–44 | 5.3 (2.9–12.5) | 18.8 (4.8–32.7) | 73.7 (59.4–87.9) | 78.9 (65.7–92.2) |
| 45–64 | 8.9 (1.3–16.5) | 14.3 (2.3–26.3) | 48.2 (34.9–61.5) | 52.7 (39.3–66.2) |
| ≥65 | 10.6 (1.7–19.6) | 21.3 (9.3–33.2) | 31.9 (18.3–45.5) | |
| Females | 24.0 (17.0–31.0) | 12.3 (4.7–19.9) | 19.9 (13.3–26.4) | 39.7 (31.7–47.3) |
| 18–44 | 23.4 (11.1–35.7) | 22.5 (9.2–35.8) | 46.8 (32.3–61.3) | 61.7 (47.5–78.9) |
| 45–64 | 25.7 (15.3–36.1) | N.O. | 10.0 (2.9–17.1) | 32.9 (21.7–44.0) |
| ≥65 | 20.7 (5.6–35.8) | N.O. | N.O. | 20.7 (5.6–35.8) |
| Non-smokers | 12.9 (8.4–17.4) | 13.9 (3.4–24.5) | 27.2 (21.2–33.1) | 39.6 (33.1–46.2) |
| Males | 5.2 (0.7–9.6) | 15.6 (4.7–26.4) | 40.2 (30.3–50.1) | 44.3 (34.3–54.3) |
| Females | 19.2 (12.1–26.3) | 13.5 (3.9–22.9) | 16.7 (9.9–23.4) | 35.3 (27.2–44.5) |
| Smokers | 26.9 (16.1–37.6) | 14.4 (7.3–21.5) | 50.7 (38.6–62.9) | 67.0 (55.2–78.2) |
| Males | 16.3 (4.9–27.7) | 17.4 (1.1–33.7) | 58.1 (42.9–73.3) | 71.4 (57.3–85.5) |
| Females | 45.8 (25.1–66.6) | 10.0 (3.4–23.9) | 37.5 (17.3–57.7) | 58.3 (37.8–78.9) |
N.O.: no observations.
Among workers, prevalence of exposure at work was 14.1% (95% CI 8.3–19.9), without significant differences according to sex (p=0.536) or smoking status (p=0.940). Workers declared to be exposed a mean of 22.1hours (95% CI 8.2–36.0) without differences related to sex (p=0.114).
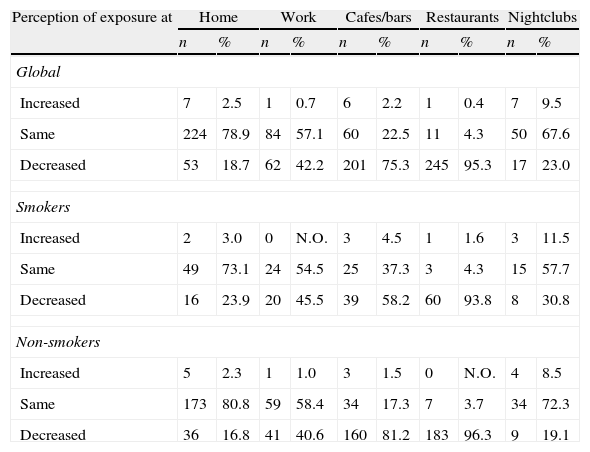
Comparison with the pre-law periodThe perceived exposure at home remained similar to the pre-law period, 79% stated that no changes had occurred. Approximately 4 out of 10 workers or students perceived a decrease in the exposure to smoke at work or school. The remaining 6/10 declared no modification. The highest perceived impact of the law was reported in relation to restaurants and cafes/bars, but remained unchanged for nightclubs (Table 3).
Perception of exposure in 2010 at home, work, cafes/bars, restaurants, nightclubs in comparison to 2007 in global and by smoking status.
| Perception of exposure at | Home | Work | Cafes/bars | Restaurants | Nightclubs | |||||
| n | % | n | % | n | % | n | % | n | % | |
| Global | ||||||||||
| Increased | 7 | 2.5 | 1 | 0.7 | 6 | 2.2 | 1 | 0.4 | 7 | 9.5 |
| Same | 224 | 78.9 | 84 | 57.1 | 60 | 22.5 | 11 | 4.3 | 50 | 67.6 |
| Decreased | 53 | 18.7 | 62 | 42.2 | 201 | 75.3 | 245 | 95.3 | 17 | 23.0 |
| Smokers | ||||||||||
| Increased | 2 | 3.0 | 0 | N.O. | 3 | 4.5 | 1 | 1.6 | 3 | 11.5 |
| Same | 49 | 73.1 | 24 | 54.5 | 25 | 37.3 | 3 | 4.3 | 15 | 57.7 |
| Decreased | 16 | 23.9 | 20 | 45.5 | 39 | 58.2 | 60 | 93.8 | 8 | 30.8 |
| Non-smokers | ||||||||||
| Increased | 5 | 2.3 | 1 | 1.0 | 3 | 1.5 | 0 | N.O. | 4 | 8.5 |
| Same | 173 | 80.8 | 59 | 58.4 | 34 | 17.3 | 7 | 3.7 | 34 | 72.3 |
| Decreased | 36 | 16.8 | 41 | 40.6 | 160 | 81.2 | 183 | 96.3 | 9 | 19.1 |
N.O.: no observations.
In Chaves, two years after the implementation of the Tobacco Control Law, almost 50% of the adults attending clinical settings still considered themselves to be exposed to ETS, mainly at leisure time. In those places where the law banned tobacco consumption, perceived exposure to ETS had dropped in comparison to the pre-law period, but the decrease was only relevant for restaurants. Perceived exposure at work remains mainly unchanged as well as exposure at nightclubs. These data confirm the necessity for a comprehensive law.
As in other studies,10–12 our results show that age is the main determinant of self-reported exposure to ETS with an inverse association in males and females. But this fact was not present when the setting of exposure was taken into account. So among females exposure at home remained unchanged, irrespective of age and this association only appeared in public places. As in other studies,7 smokers in Chaves declare to be more exposed to ETS in comparison to non-smokers.
In the present study, 14% of the workers reported being exposed at work. This is a low percentage probably due to the high proportion of individuals that are agriculture workers. The percentage of white collar workers is lower than in an urban area, and this prevalence is conditioned by this fact.
When compared to the pre-law period, perceived exposure at home did not change. The data related to exposure at home are consistent with those of previous studies.13,14 Moreover two studies,15,16 also conducted in Portugal, reported that the percentage of smokers at home has not changed significantly before and after the law.
In cafes and bars the perceived reduction of exposure to ETS after the law enforcement was 75%. Reis and colleagues17 showed that almost 40% of cafes completely banned smoking inside the establishment, and in Porto, Precioso et al.18 estimates the percentage of cafes banning smoking inside was around 75%. In Portugal, the majority of restaurants decided to ban smoking inside with the largest percentage of adherence to the law in restaurants with more than one hundred square meters. But a recent study in several restaurants in Lisbon showed that levels of indoor ETS pollution at these locations is high.19 In our study 95% of subjects reported a lower passive exposure in these premises. As in Chaves, a lower adherence to the law in clubs was also found in Braga.20
In this study the prevalence of smokers (23.6%) was similar to that obtained in the Inquerito Nacional de Saude (20.8%) and in the Eurobarometer (24%).21 But differences arise when former smokers are taken into consideration. So in Chaves this group comprises 27.8% of the population compared to12% in Portugal.21 This large percentage of former smokers is likely to be related to the study setting, because ever smokers attend healthcare facilities more frequently.
A potential limitation of our study is that it was carried out in a clinical setting. Under representation of the young population is explained by the fact that recruitment was done at a GP facility. The population usually attending healthcare facilities is older and it is easier to get a representative number of that age group. It is probable that prevalence of exposure to ETS is underestimated because young individuals in this study comprised only 3% of the population, while in Chaves they account for 13%; and are the group declaring the higher exposure to ETS in this and in other studies.7,10
A possible selection bias could be present because this survey was limited to volunteers selected from patients attending to a healthcare center at a particular time. This bias could misrepresent the results, because tobacco consumption and ETS exposure are causally associated to several pathologies, increasing the probability of attending the healthcare facilities.
A problem that can occur when comparing pre-law and post-law periods is recall bias. But it is not possible to truly assess its impact since no background information is available regarding ETS exposure in the study area. Moreover, sample size does not guarantee statistical power to undertake the specific analysis.
Despite its limitations,22 self-reported information was the method used to assess exposure to ETS and tobacco consumption in this study. In relation to ETS exposure, a validated questionnaire derived from Spanish studies and adapted to Portuguese context was used. But due to the lack of consensus on how this exposure should be quantified, comparison with other studies should be treated with caution.
Nevertheless this study has also some advantages. It is the first one assessing the perceived exposure to ETS after the tobacco law enforcement in a general population context.
We have collected exhaustive information on different places where exposure can occur. This fact allows us to have quite a clear picture of ETS exposure after the enactment of the law. Due to the implementation of tobacco control legislation exposure profiles could change, and identifying the diverse settings where exposure to ETS may occur is essential to accurately assess the impact of different laws over time.
Finally, the fact of having assessed CO and the high correlation value obtained with self declared tobacco consumption means that misclassification of tobacco habit is probably negligible.
ConclusionsEven though this work was developed in a regional context, its findings especially those regarding the passive exposure in public places, can be considered as contributing an element of evaluation of the Portuguese smoking ban.
ETS exposure after the enforcement of the tobacco banning law in Portugal is still high, with great differences depending on different settings of exposure. ETS exposure is still high in nightclubs.
There are also substantial differences in exposure regarding age and sex, with younger population being more exposed. Finally, population perceived a reduction of ETS exposure after the law enactment but in settings such as work or nightclubs perceived exposure remains unchanged for more than 5 out of 10.
The ECOS Infotabaco20 and different studies developed in Portugal23,24 showed that the majority of the Portuguese population have a favorable opinion about smoke free places. Taking into consideration this favorable climate and the results of this study, a comprehensive strategy aimed at improving population protection against ETS exposure is feasible.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Paradela C, et al. Exposição ao fumo ambiental do tabaco em Chaves depois da implementação da Lei 37/2007. Estudo transversal em 2 centros de saúde. Rev Port Pneumol. 2013. http://dx.doi.org/10.1016/j.rppneu.2013.02.003.


