


Reported for the first time in 1996, aquagenic keratoderma is a rare condition which is characterized by edematous flat-topped papules appearing on palmar skin after water immersion. Multiple anecdotal associations have been described but, recently, the association with cystic fibrosis gene mutations (CFTR) has been highlighted.
The authors describe an 18-year-old female, with one-month complaints of pruritus and swelling of palmar skin after water immersion. On examination, palmar skin was unremarkable but, 5min after water immersion, multiple whitish papules became apparent. CFTR genotype study showed a F508del mutation in one allele (nonhomozygous). She had no other symptoms and no relevant family history.
Aquagenic keratoderma is probably an under-diagnosed entity that might represent a manifestation of CFTR mutations, making carrier state identification and genetic counseling possible.
Descrita em 1996, a acroqueratodermia aquagénica é uma entidade rara, caracterizada pelo aparecimento de pápulas edematosas palmares após contacto com água. Múltiplas associações foram enumeradas mas, recentemente, a associação a mutações do gene da fibrose quística foi demonstrada.
Descreve-se o caso de uma mulher de 18 anos, saudável, com prurido e edema palmar após imersão em água. O exame objetivo inicial não mostrava alterações mas, 5 min após imersão em água, observavam-se múltiplas pápulas esbranquiçadas palmares. O estudo do gene da fibrose quística (CFTR) revelou uma mutação F508del num dos alelos. A doente negava outras queixas ou história familiar relevante.
A acroqueratodermia aquagénica é uma entidade provavelmente subdiagnosticada que poderá constituir uma manifestação de mutações do gene CFTR, o que possibilitaria a identificação de portadores e aconselhamento genético.
Aquagenic wrinkling of the palms was first reported in 1996 by English and McCollough.1 Since then, different designations have been used in the literature: Transient Reactive Papulotranslucent Acrokeratoderma,1 Aquagenic Syringeal Acrokeratoderma,2 and Aquagenic Palmoplantar Keratoderma.3 It is characterized by thickening of the palms, and on rare occasions also the soles, after brief immersion in water. To date fewer than 50 cases have been reported in the literature.
Although multiple associations have been reported, recent papers highlight the connection with Cystic Fibrosis and Cystic Fibrosis gene (CFTR) mutations.
In this article the authors describe a patient with aquagenic keratoderma associated with a CFTR mutation.
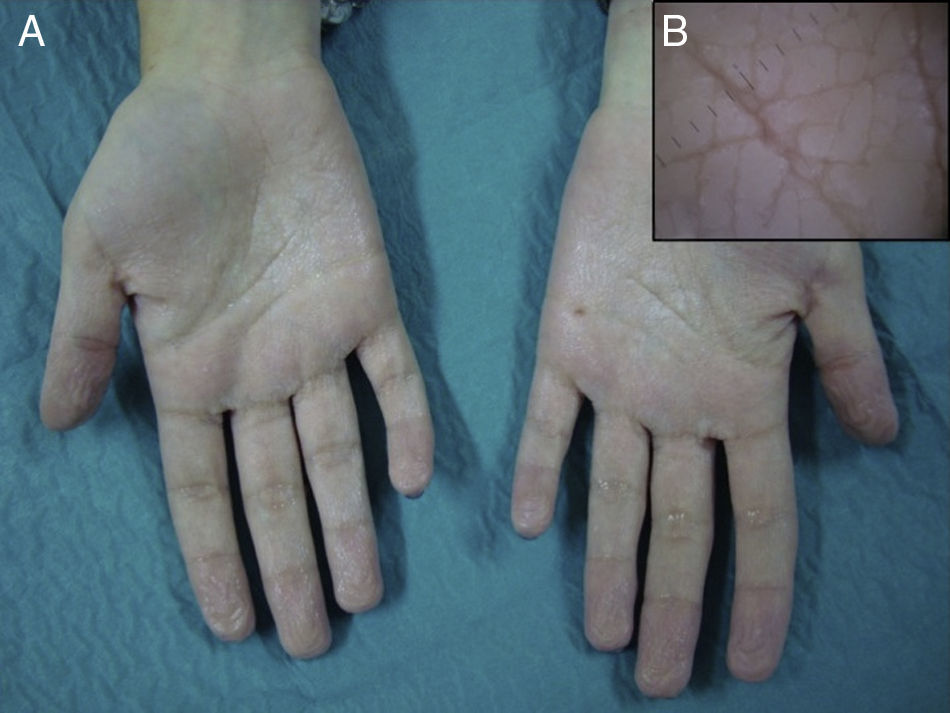
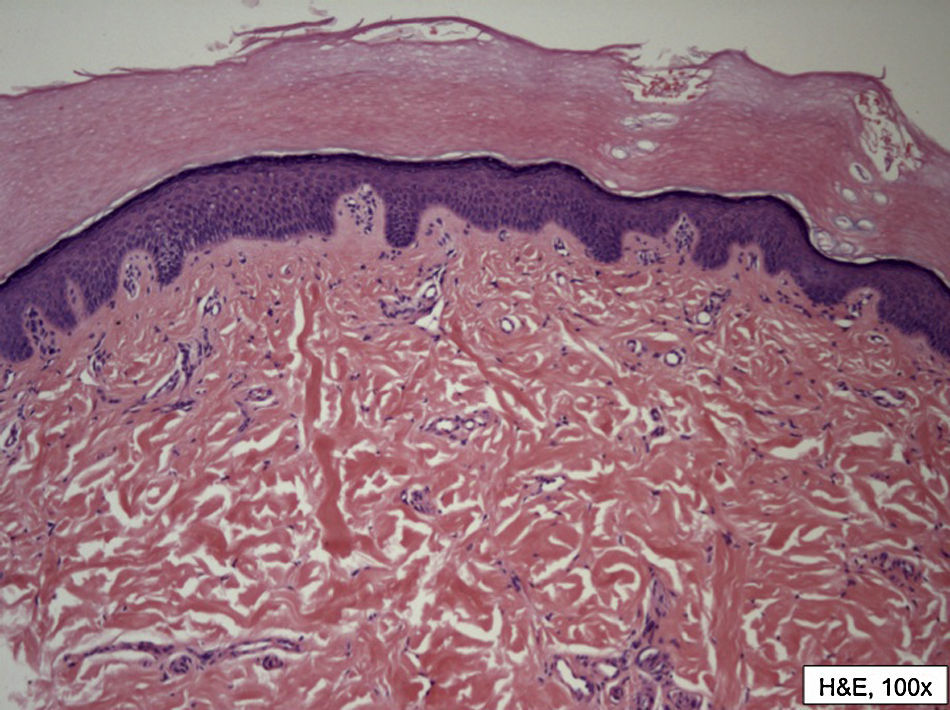
Case reportAn 18-year-old Caucasian female patient presented with a one-month history of pruritus and thickening of palmar skin, shortly after water immersion. Warm water triggered the symptoms more briefly and the dermatosis remitted 20min after water exposure ceased. Her soles were unaffected and she had no other medical complaints. Her personal and family medical histories were irrelevant. On physical examination, palmar skin was unremarkable (Fig. 1) but, 5min after water immersion, multiple small, edematous, whitish flat-topped papules were evident. Dermoscopy revealed edematous skin with dilated puncta (Fig. 2). Skin biopsy of palmar papule after water immersion showed orthohyperkeratosis, dermal swelling and dilation of acrosyringia and eccrine ostia (Fig. 3). Genetic study of the CFTR gene identified a single F508 mutation. No sweat chloride test was performed.

 Palmar skin after 5min water immersion: subtle whitish, edematous and flat-topped papules became apparent. (B) Detail on dermoscopy.")

The patient was treated with topical 20% aluminum chloride with improvement of the lesions and complaints. Due to the Cystic Fibrosis carrier state of the patient, she and her family were referred for genetic counseling.
DiscussionAquagenic keratoderma is a rare condition characterized by symmetric, flesh-colored to white, edematous, flat-topped papules with dilated ostia located on the palms and finger margins. The soles are rarely involved. The skin lesions typically appear after brief exposure to hot3,4 or cold water,1,2,5,6 and usually disappear soon after being dried. When not exposed to water, the skin of affected patients either looks normal or there is hyperlinearity or multiple unremarkable translucent white papules on the palms or soles.5,7 The condition is usually asymptomatic but it can cause pain, pruritus, burning or tightness. Patients are predominantly female,3,8–10 especially among the younger ones (age of onset from 9 to 42 years).11,12 An autosomal recessive inheritance pattern was initially proposed,1 however more recent cases suggest an autosomal dominant pattern.13 Typically, histological examination (after water exposure) shows hyperkeratosis, orthokeratosis and dilation of acrosyringia and eccrine ostia.
Multiple anecdotal associations have been described in the past, namely, atopy,14 COX-2 inhibitors therapy,14,15 marasmus,14 palmar hyperhidrosis,14 Raynaud's phenomenon,14 malignant melanoma,1 Behçet disease16 and nail psoriasis.16 However recent studies tend to emphasize a possible relation between aquagenic keratoderma and cystic fibrosis. It is estimated that more than half the patients with aquagenic keratoderma (56.7%) have documented cystic fibrosis17. Although aquagenic keratoderma seems to be more prevalent in cystic fibrosis patients, Gild et al.14 reported the first case associated with a single mutation in the CFTR gene, suggesting that aquagenic keratoderma may be a sign of the cystic fibrosis carrier state.
The pathogenesis of aquagenic keratoderma remains unknown. Due to the increased sweat chloride concentration in Cystic Fibrosis patients, an increased water-binding capacity of epidermal keratinocytes has been suggested.18,19 Berk et al.,20 however, showed that there was no relationship between sweat chloride concentration and aquagenic wrinkling of the palms score. Several other hypotheses remain in debate, such as eccrine gland4,21 or nerve22 dysfunction, hyperhidrosis,21 defective barrier function of the stratum corneum,5,6 occlusion of eccrine duct ostia2 and weakness of the eccrine duct wall.4
Like the patient described, the ΔF508 is the most commonly reported mutation associated with aquagenic keratoderma in cystic fibrosis patients.17 Although this is the most common CFTR mutation (70% of cystic fibrosis mutations in north European Caucasian patients)17,23 some authors speculate that this particular mutation could represent a predisposing factor for aquagenic keratoderma.17,20
Multiple effective therapies have been reported, including aluminum chloride,3,17 antihistamines,5 botulinum toxin injections,7 iontophoresis4 with variable results. Spontaneous remission has also been described.2,3,5,17
In the present case, aquagenic keratoderma might represent the sole manifestation of the cystic fibrosis carrier state of the patient. This highlights the importance of considering and testing for this type of genetic abnormality in these patients. Similarly, this type of dermatologic condition should be looked for in both cystic fibrosis patients and known carriers, not only because there are available therapies but also due to the fact that new reports and studies could help clarify the pathogenesis of both conditions. The authors believe that aquagenic keratoderma is an under-diagnosed condition, which can be misdiagnosed as a physiologic whitish discoloration and wrinkling of the palms, a consequence of digit pulp vasoconstriction,24 normally associated with prolonged water exposure.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Coelho-Macias, V. Acroqueratodermia aquagénica associada a uma mutação do gene da fibrose quística. Rev Port Pneumol 2013. http://dx.doi.org/10.1016/j.rppneu.2012.10.005.


