


Chronic obstructive pulmonary disease (COPD) has been a leading cause of morbidity and mortality worldwide, over the years. In 1995, the implementation of a respiratory function survey seemed to be an adequate way to draw attention to neglected respiratory symptoms and increase the awareness of spirometry surveys. By 2002 there were new consensual guidelines in place and the awareness that prevalence of COPD depended on the criteria used for airway obstruction definition. The purpose of this study is to revisit the two studies and to turn public some of the data and respective methodologies.
MethodsFrom Pneumobil Study database of 12,684 subjects, only the individuals with 40+ years old (n=9.061) were selected. The 2002 Study included a randomized representative sample of 1384 individuals with 35–69 years old.
ResultsThe prevalence of COPD was 8.96% in Pneumobil and 5.34% in the 2002 Study. In both studies, presence of COPD was greater in males and there was a positive association between presence of COPD and older age groups. Smokers and ex-smokers showed a higher proportion of cases of COPD.
ConclusionsPrevalence in Portugal is lower than in other European countries. This may be related to lower smokers’ prevalence. Globally, the most important risk factors associated with COPD were age over 60 years, male gender and smoking exposure. All aspects and limitations regarding different recruitment methodologies and different criteria for defining COPD cases highlight the need of a standardized method to evaluate COPD prevalence and associated risks factors, whose results can be compared across countries, as it is the case of BOLD project.
A doença pulmonar obstrutiva crónica (DPOC) tem sido, ao longo dos anos, uma importante causa de morbilidade e mortalidade no mundo. Em 1995, a implementação de um rastreio da função respiratória pareceu a forma mais adequada para alertar para os sintomas respiratórios negligenciados e sensibilizar para os rastreios espirométricos. Em 2002, foram criadas novas normas consensuais de diagnóstico e o reconhecimento de que a prevalência da DPOC depende dos critérios de definição de obstrução das vias aéreas. O objetivo deste estudo foi revisitar estes 2 estudos e publicar alguns dos resultados e respetivas metodologias.
MétodosDos 12,684 indivíduos que constavam da base de dados do Pneumobil, apenas os indivíduos com 40 e mais anos (n=9061) foram considerados para esta análise. No estudo de 2002 foi incluída uma amostra aleatorizada e representativa de 1384 indivíduos, com idades entre os 35 e os 69 anos.
ResultadosA prevalência da DPOC foi de 8.96% no estudo Pneumobil e de 5.34% no estudo de 2002. Em ambos os estudos, a presença da DPOC foi superior no sexo masculino, tendo-se verificado uma associação positiva entre a presença da DPOC e os grupos etários mais velhos. Nos fumadores e ex-fumadores encontrou-se maior proporção de casos com DPOC.
ConclusõesA prevalência em Portugal é mais baixa do que noutros países europeus, o que pode estar relacionado com uma menor prevalência de tabagismo. De um modo geral, os fatores de risco mais importantes que mostraram a associação com a DPOC foram a idade maior do que 60 anos, o sexo masculino e a exposição tabágica. Todos os aspetos e as limitações que se referem a diferentes critérios de definição e a metodologias de recrutamento realçam a necessidade de métodos padronizados para determinar a prevalência da DPOC e os fatores de risco associados, cujos resultados possam ser comparados entre países, como acontece no projeto BOLD.
Chronic obstructive pulmonary disease (COPD) is a rising cause of morbidity and mortality worldwide,1,2 and Portugal is no exception.3
In 1990 COPD was the sixth most common cause of death worldwide and was ranked 12th for DALYs (disability-adjusted life years).4,5 It has been projected that by 2020 it will have risen to 5th rank, and be the third most common cause of death.5–7
This situation has led to the development of the Global Initiative for COPD (GOLD)7 of which the primary goal is to control and invert the burden of COPD.
Historical backgroundIn 1995, both the American Thoracic Society (ATS) and the European Respiratory Society (ERS) published data about the prevalence of airways obstruction in a general population as a plan to standardize the diagnosis of COPD.8,9
At that time, in Portugal, the information on the prevalence of respiratory diseases was scarce and pulmonary function evaluation and screening was not a regular practice in the diagnosis workup.10
For many years, early manifestations of COPD were unnoticed and undetectable, both by patients and physicians, because the respiratory function characterization of the inflammatory airway pathology was rarely requested.10
The implementation of a pulmonary function survey seemed to be an appropriate way of drawing attention to unknown symptoms and to measure disturbances, and at the same time to alert both population and practitioners to this health problem.
The first Pneumobil Study took place in Portugal from 1995 to 1997 with the goal of estimating the prevalence of COPD, asthma and respiratory symptoms and characterizing the associated risk factors in the Portuguese population, including population above 18 years old.
In 1998 the Global Initiative for Chronic Obstructive Lung Disease (GOLD) was launched11 and in 2001 the guidelines7 for the classification of COPD were published. The main goals of GOLD are to increase awareness of COPD, decrease morbidity and mortality, and to improve prevention and management of COPD through a concerted worldwide effort by people involved in health care and health care policy-making, as well as to encourage a renewed research interest in this highly prevalent disease.7
One major problem that GOLD came up with was the incomplete information in many countries about the prevalence and causes of COPD.7
By that time there were new consensual guidelines and the awareness that prevalence of COPD in a general population depended very much on the criteria used for airway obstruction definition, and data showed wide prevalence rates across countries.12
Considering these new aspects highlighted by GOLD, a new Prevalence Study was implemented, 2002 Prevalence Study, which aimed to estimate the prevalence rates of COPD and evaluate the severity of obstruction, smoking habits, and other risk factors in Portugal. GOLD
Despite the implementation of GOLD, COPD is nowadays ranked fourth in developed countries, with approximately 2.75 million deaths per year, representing 4.8% of deaths.11 It still is an under-recognized, under-diagnosed and under-treated disease, and is frequently diagnosed too late.13–15 GOLD's approach appears to overestimate
COPD in older individuals and to underestimate it in younger adults. This raises questions about which criteria should be used for the definition of obstruction and which reference equations are appropriate for the populations.16
In 2004, the international Burden of Obstructive Lung Disease (BOLD) initiative developed standardized methods for estimating prevalence and economic burden of population-based COPD.15 These methods can be used in countries at all levels of development. The aim of BOLD is to measure the worldwide prevalence of COPD and its risk factors in adults aged 40 years and older and to investigate variation in prevalence across countries by age, gender, and smoking status.15
The BOLD Study has also been implemented in Portugal, during 2008 and published results are awaited.
The purpose of this study is to revisit those two studies done in Portugal some years ago, in order to make public some of the data and respective methodologies, since data from both studies are dispersed in communications, posters, partial data published in books, oral communications with no abstracts and publications in non-available journals, which make searching of data very difficult.10,12,17,18 Moreover, we present here, for the first time, the analysis of the fraction of the population older than 40 years of the Pneumobil Study.
Material and methodsThe two studies had different methodology.
Pneumobil Study methodologyThis survey was carried out between September 1995 and December 1997 in 17 of the 18 districts of continental Portugal.
This was a survey of volunteer individuals who attended the study collection sites, mostly located on public places and who agreed to answer a questionnaire and perform a spirometry.
The population included was 14,002 individuals but only 12,684 adults over 18 years of age were considered eligible (completed questionnaire and acceptable spirometry).
For this analysis we have selected from the database only the individuals older than 40 years (n=9061).
The questionnaire, based on ATS Respiratory Questionnaire, included demographic parameters, smoking habits, professional activity, physical activity, exposure to dust and chemical smoke, history of pathology with effect on respiratory function and medication use.
Pre and post-bronchodilator spirometry was performed according to ATS guidelines19, using electronic spirometers Masterscreen IOS (Jaeger), version 4.3, with a Silverman pneumotachograph.
2002 Epidemiological Study methodologyThis Epidemiological Study was carried out between October 2001 and March 2002 in all districts of continental Portugal, stratified by region, age and gender according to demographic data from INE (National Statistics Institute – census 2001).20
The sample was selected randomly from the telephone directory and for those who agreed to participate in the study a date and time was scheduled for questionnaire answering and spirometry measurements. Because telephonic answers were very scarce 11,500 individuals had to be contacted to obtain the planned sample size. It included 1475 individuals aged between 35 and 69 years old, with a participation rate of 12.8%. From these only 1384 individuals were considered eligible (having completed the questionnaire and acceptable spirometry); however this sample was representative of the Portuguese population. People over 70 years old were excluded as participation by the older individuals which could have resulted in bias, as happened in the case of the Iberpoc Study.21
The questionnaire was the same as in the previous study. Spirometry was performed according to ATS recommendations19, using a Vitalograph alpha III® spirometer, equipped with SafeTway® mouthpiece adaptors (Fleisch pneumotachograph). In this study, the reversibility test was not performed for ethical and operational reasons (for example, no physician was available during spirometry tests).
DefinitionsIn both studies COPD was defined as the presence of FEV1/FVC<70% (post-BD in Pneumobil Study and pre-BD in 2002 Study), with or without symptoms, and without asthma or other respiratory diseases, which were excluded by the questionnaire, according to the Global Initiative for COPD (GOLD) definition.7 Individuals with symptoms but FEV1/FVC>70% were excluded as non COPD cases.
The severity of COPD was based on GOLD criteria and the ECCS reference values for Pneumobil and adapted in the 2002 Study.22
The Pneumobil data was re-analysed according to GOLD criteria, which did not exist at the time.
Statistical analysisWithin the ambit of this publication only the most relevant results for the analysis are presented.
Qualitative variables were summarized through counts (n) and percentages (%). Prevalence of COPD was calculated based on the total of individuals and by gender and smoking habits.
Statistical analyses were carried out using SPSS® version 16.0.
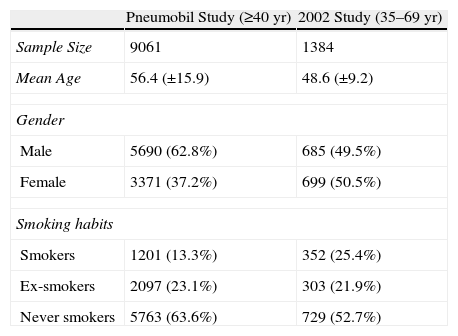
ResultsIn Table 1, sociodemographic characteristics of study samples for both studies are described. In the Pneumobil, out of 9061 individuals included, 62.8% were male, 13.3% were smokers and 63.6% were never smokers. In the 2002 Study, from the 1384 individuals included, 49.5% were male, 25.4% were smokers and 52.7% were never smokers.
Socio-demographic characteristics of study sample in Pneumobil and 2002 Study.*
| Pneumobil Study (≥40yr) | 2002 Study (35–69yr) | |
| Sample Size | 9061 | 1384 |
| Mean Age | 56.4 (±15.9) | 48.6 (±9.2) |
| Gender | ||
| Male | 5690 (62.8%) | 685 (49.5%) |
| Female | 3371 (37.2%) | 699 (50.5%) |
| Smoking habits | ||
| Smokers | 1201 (13.3%) | 352 (25.4%) |
| Ex-smokers | 2097 (23.1%) | 303 (21.9%) |
| Never smokers | 5763 (63.6%) | 729 (52.7%) |
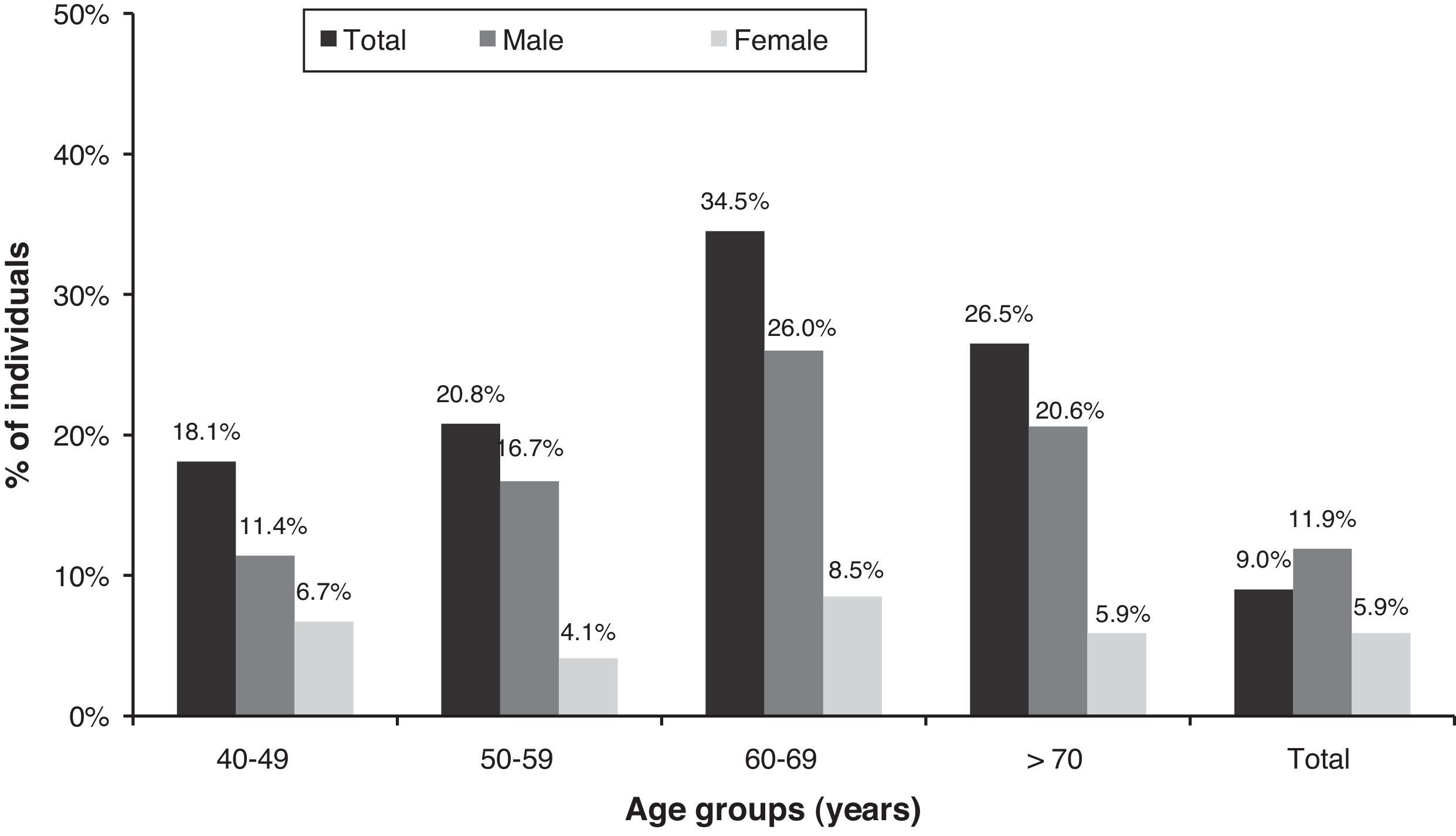
As shown in Fig. 1 and in Fig. 2, there was an overall COPD prevalence of 8.96% in the Pneumobil studied population (age range 40 years old), 11.9% in males and 5.9% in females. In the 2002 Study, 5.34% of COPD cases were identified (age range 35–69 years old), 6.3% in males and 4.5% in females.
.")
.")
In these two figures, the distribution of COPD cases by age and gender was also shown. More than 61% of cases were identified above 60 years old in Pneumobil Study vs. more than 32% in 2002 Study. Moreover, 26.5% of cases were identified above 70 years old in Pneumobil Study, an age range not studied in 2002. It should also be noted, that below 60 years old, a higher proportion of cases were females in the 2002 Study vs. Pneumobil (29.8% vs. 10.8%).
Regarding smoking habits for COPD cases found in both studies, in Pneumobil the prevalence in smokers was 15.4% and in never smokers it was 6.7%. In the 2002 Study the prevalence in smokers was 8.8% and in never smokers was 4.4%.
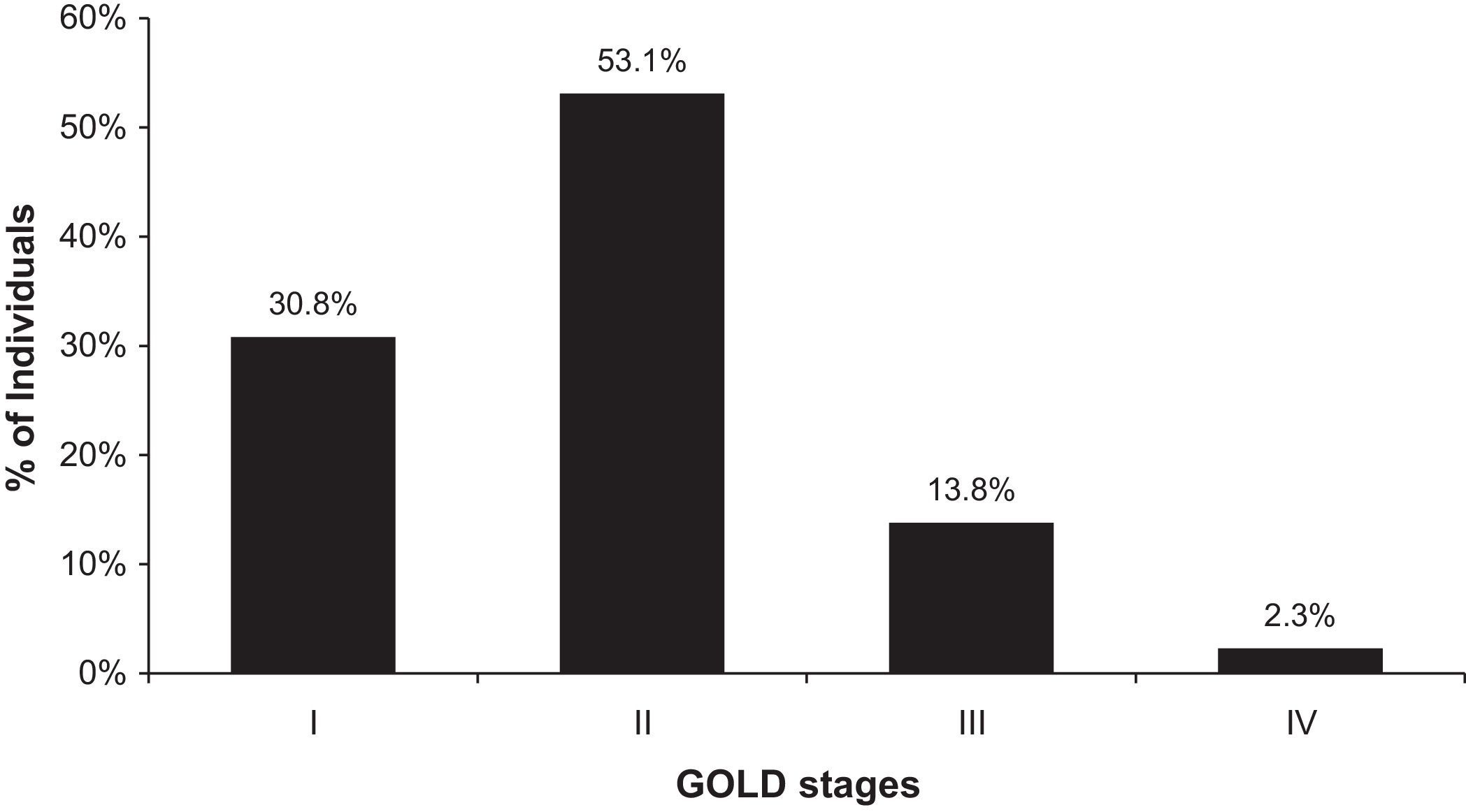
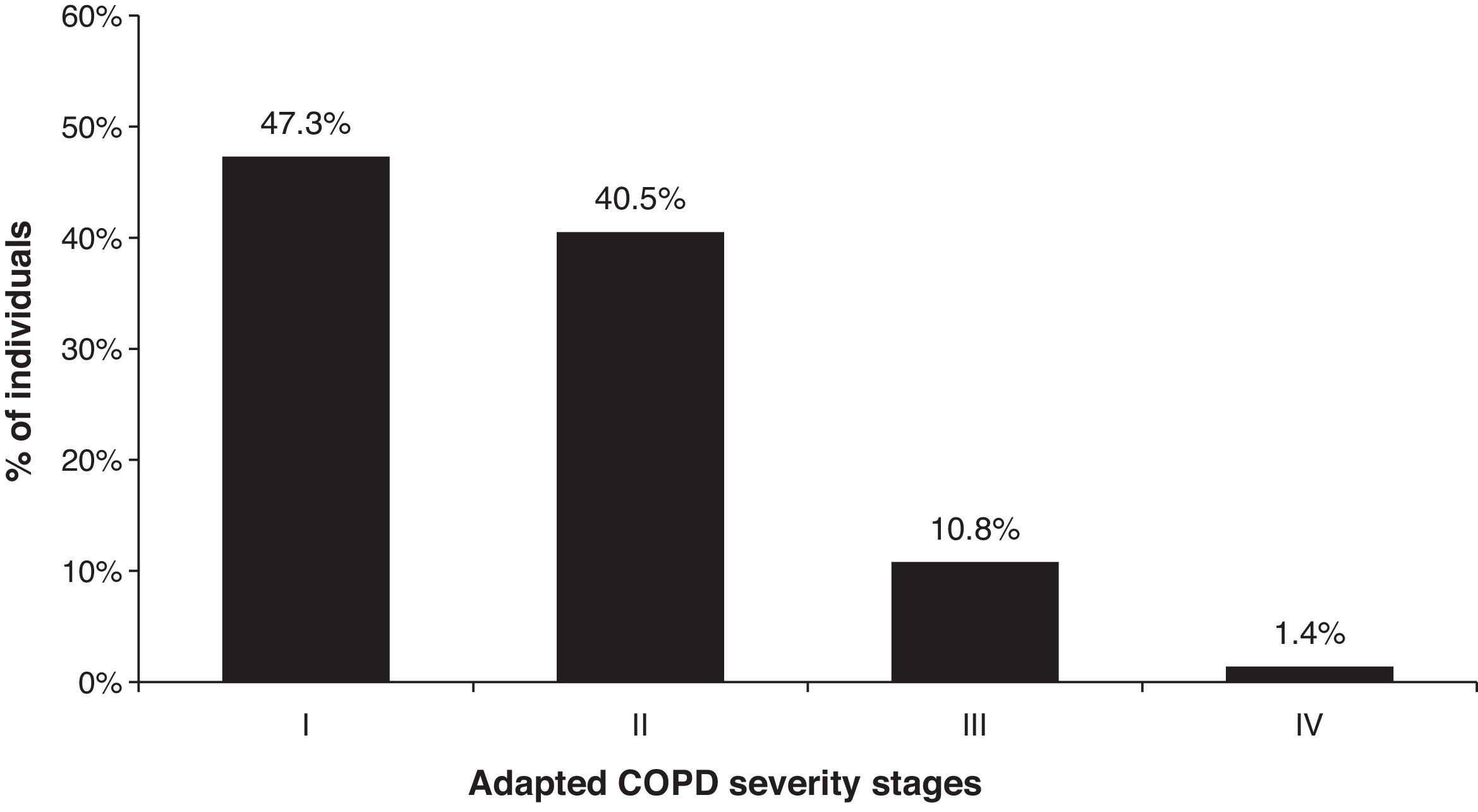
Figs. 3 and 4 show the distribution of COPD severity (GOLD in Pneumobil Study and adapted from GOLD in 2002 Study). In both studies, it can be seen that the proportion of the combination of stage I and II are similar, 83.9% in Pneumobil Study and 87.8% in 2002 Study. However, more cases were found in stage I in 2002 Study (47.3% vs. 30.8%). In addition, even with a cut-off of 69 years old in the 2002 Study, the proportion of combined stage III and IV is very similar in both studies, but higher in Pneumobil (16,1% vs. 12,2%).
.")
.")
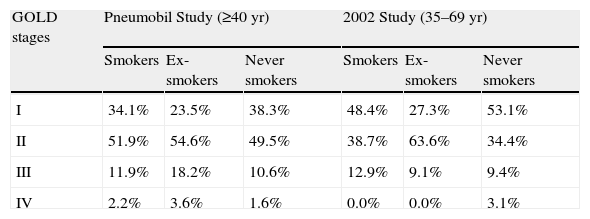
In Table 2 we present the distribution of COPD cases by smoking status and severity. In Pneumobil 21.2% of cases were found in smokers and in 2002 Study it doubled to 41.9%. As referred to above, there was a low prevalence of smokers in Pneumobil (13.3%) compared to 25.4% in the 2002 Study.
COPD prevalence by smoking habits and GOLD stages.
| GOLD stages | Pneumobil Study (≥40yr) | 2002 Study (35–69yr) | ||||
| Smokers | Ex-smokers | Never smokers | Smokers | Ex-smokers | Never smokers | |
| I | 34.1% | 23.5% | 38.3% | 48.4% | 27.3% | 53.1% |
| II | 51.9% | 54.6% | 49.5% | 38.7% | 63.6% | 34.4% |
| III | 11.9% | 18.2% | 10.6% | 12.9% | 9.1% | 9.4% |
| IV | 2.2% | 3.6% | 1.6% | 0.0% | 0.0% | 3.1% |
In both studies, the proportion of the never smokers class was very similar, i.e., around 44%. However, the prevalence of COPD in this class was higher in Pneumobil than in 2002 Study (6.7% vs. 4.4%).
In general, the distribution of the cases by smoking status and severity (Table 2) overlaps the general distribution of severity in both studies (Figs. 3 and 4), with around 85–90% of cases in stage I and II. In more severe stages, the trend is similar in both studies by smoking class, but for instance, in stage III the ex-smokers in 2002 are 9.1% of cases, while in Pneumobil we found 18.2% (Table 2).
The different age range and the higher fraction of ex-smokers in Pneumobil are possible reasons to account for these findings.
DiscussionThree major and important limitations are present in these studies: (1) for Pneumobil, it is not a truly randomized study; (2) for 2002 Study, the criterion for COPD was not based on a post-bronchodilator spirometry; (3) criteria for obstruction is different in the two studies so the prevalence results cannot be compared. Nevertheless, some results are valid on their own.
Different figures for COPD prevalence were found in the two studies and diverse methodologies may explain these different values. In Pneumobil the age range was larger with individuals over 70 years being included. Even if the fixed ratio criteria for obstruction may overestimate the prevalence in this age range, it is possibly more real than the prevalence of the 2002 Study that excluded individuals of 70 and over. The COPD prevalence of the 2002 Study may be appropriate for the age range studied, but it is surely an underestimate for the general population.
The concern that older people could be missed because they might not come to centres (possible reason for the low overall prevalence in participants of 70 years and over in Pneumobil Study), was accounted for in the design of the 2002 Study that excluded this age range, but did not translate into significant different degrees of severity. Nevertheless, more severe stages of disease were found in Pneumobil (perhaps more severe cases volunteered to undergo testing) and this may have under-estimated the prevalence of COPD in 2002.
A different time frame is another reason for differences. The known prevalence of smoking habits in Portugal was not different in 1995 vs. 2002 (total 17.3% vs. 18.0%), except for a slight increase in female smokers (6.5% vs. 7.9%).23
The lack of randomization is a possible reason for the low prevalence of smokers and ex-smokers in Pneumobil Study.
The occurrence of more female cases at younger ages in 2002 Study is in line with this time frame difference.
Although the participation rate of the 2002 Study was very low, the representative and random selection procedure of the included sample was assured, which is an added value for this study.
The fact that Pneumobil was not a truly randomized study, as individuals volunteered for the survey, is a possible factor for discrepancies between the two studies (people living far away from the collection sites might have been excluded). But in a sample of 12,684 individuals this bias would have been minimized and the bringing of the vehicle to people, who were worried about having the disease, may explain more severe COPD cases reached.
As a protocol option, in the 2002 Study no bronchodilator was administered to test reversibility, mainly for ethical and operational reasons. This was also a limitation of many other surveys at that time, like NHANES III.24
Although it was not possible to apply a true GOLD criteria (due to absence of reversibility test, which might overestimate COPD cases) data can be reasonably accepted, since most of asthma and other chronic airflow limitations were excluded by the questionnaire. This was also the opinion of Fukuchi et al.25 in a Japanese prevalence study.
Another important aspect is that the two studies were done with two different spirometers. If for the Pneumobil Study we think that there is no reason for suspecting errors, for the 2002 Study it may not be the case. A possible limitation of the FVC value (software cutting values of low flows) is suspected because the median of FEV1/FVC ratio was higher than expected (84.4%). So, the prevalence rate estimated using fixed ratio criteria can, in fact, be underestimated in 2002 Study.
Consistent with others,8,21,26 these studies also showed higher prevalence rates in men. Increasing age is a significant factor related to prevalence and the older population appears to have an increased risk for COPD, independent of their smoking history.
Globally, the most important risk factors associated with COPD in these studies were age over 60 years, male gender and smoking exposure.
Nevertheless, the presence of a significant proportion of COPD cases in never smokers may indicate that other risk factors may be present in the Portuguese population (e.g. biomass exposure, previous respiratory diseases, childhood infections).
Higher COPD prevalence values are expected in future prevalence studies as the major limitations of the two studies, that accounted for underestimation (age range, randomization, adequate spirometers, use of post-BD spirometry), should be corrected.
ConclusionsThese two studies contributed to our knowledge of COPD prevalence in Portugal, as they suggest a somewhat lower frequency of occurrence than in other European countries. This can be accepted as the consequence of lower percentage of smoking people and of smoking history.
Globally, the most important risk factors associated with COPD were age over 60 years, male gender and smoking exposure.
In these surveys, COPD severity stages I and II accounted for over 85% of the cases, and this fact indicates the need for special attention to spirometric approach, its quality and its abnormalities.
However more frequent in smokers and ex-smokers, COPD occurred also frequently in non-smoker men and women, and this fact justifies a closer attention to other causal factors in the future.
All aspects and limitations regarding methodology highlight the need for a standardized method to evaluate COPD prevalence and associated risks factors, so that results can be compared across countries, as is the case with BOLD project.15
It is believed that a concerted effort by everyone involved in health care, governments, public health officials, health care workers, and even the general public, is needed to control this still major public health problem.7
FundingBoth studies were conducted by the Respiratory Portuguese Society and funded by Boehringer Ingelheim and Pfizer.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank to: (a) Working Committee of Pneumobil and 2002 studies, under the scientific support of Respiratory Portuguese Society, in particular to Prof. J.H. Paiva de Carvalho, Prof. António Couto, Prof. Bensabat Rendas, Dr. J. Pontes da Mata, Dr. Isabel Melo, Dr. Paes Cardoso. Honour Committee: Prof. A.J. A. Robalo Cordeiro, Prof. M. Freitas e Costa, Prof. Ramiro Ávila e Prof. J. Agostinho Marques. (b) Escola Superior de Tecnologia da Saúde de Coimbra – Prof. Jorge Conde – and to Associação Portuguesa de Cardiopneumologistas – Luís Caldeira – and all the involved cardiopulmonology technicians, in particular Alexandra Guardado and Helena Pedrosa. (c) Prof. António Gouveia for the statistical support.
A special thank you to Prof. G. Viegi for all the sympathy and for the accurate and insightful revision of the 2002 Study data.
The investigators would also like to thank to Carlos Capela, as sponsor project leader, Ana Durão and José Antunes and everybody at Boehringer Ingelheim Portugal and Pfizer who were involved and collaborated in these two projects.
Please cite this article as: Cardoso, J; Doença Pulmonar Obstrutiva Crónica em Portugal: estudo Pneumobil (1995) e estudo de prevalência de 2002 revisitados. Rev Port Pneumol 2013. http://dx.doi.org/10.1016/j.rppneu.2012.11.005


