

Pulmonologists are involved in the assessment of functional impairment in patients with occupational respiratory diseases.1–3 These patients often complain that dyspnea on exertion interferes with their ability to do their job and they may be legally compensated according to the functional deficit reported.4,5
Cardiopulmonary exercise testing (CPET) is a valuable clinical test for assessment of exercise intolerance and is taken into account when providing relevant information to assess functional impairment and disability. 6–15 Several researchers have demonstrated the utility of CPET in determining the functional deficit. 16–22 Of all parameters determined, maximal Oxygen consumption (VO2 max) is the one that reveals exercise limitation and is used in most guidelines for quantifying functional impairment.7–9 A normal VO2 max implies that respiratory function is preserved, showing no significant functional deficit. A decreased VO2 max may have several causes and the other parameters provide information to determine the factors that contribute to exercise intolerance (psychogenic, deconditioning, cardiovascular limitation, ventilatory limitation or limitation by gas exchange abnormalities). 16–19,23 The maximal oxygen consumption in office work is 5–7mL/kg/min, in moderate physical work about 15mL/kg/min and in physically demanding work 20 to 30mL/kg/min13, these are approximate figures.
In Portugal, respiratory disability is regulated by law, according to a scale of disability resulting from accidents at work and occupational diseases, the Tabela Nacional de Incapacidades por Acidentes de Trabalho e Doencas Profissionais (Decreto-Lei n.° 352/2007 de 23 de Outubro).24 It relies mainly on pulmonary function tests and the usefulness of the exercise test is also mentioned “if the lung function is normal at rest or whenever deemed clinically appropriate”.
Since the availability of CPET is limited to a few centers, it's not routinely used in the evaluation of the functional deficit and disability. In this context, the pulmonary function test performed at rest is used as an indirect estimation of exercise capacity.25 This is open to challenge, as there is little evidence, and what there is based, largely, on expert opinion. Some authors have criticized the lack of relationship between lung function at rest and results in exercise. 13,26–28 Besides that, there are practical difficulties and controversies in the use of this important tool for defining impairment and disability, when measured against the Portuguese scale with current scientific evidence and guidelines:
- 1.
The Portuguese scale considers disability “the values of PaO2 reached, being positive the fall of 10mmHg in PaO2”, instead of maximal oxygen consumption (VO2 max), used in current scientific evidence.
- 2.
By only considering PaO2 in exercise, we are only taking into account one of the factors that may be responsible for impairment and disability.
- 3.
A patient with a 10mmHg decrease in PaO2 does not necessarily have exercise intolerance; in fact, a drop from 90 to 80mmHg has different implications for exercise than a decrease from 75 to 65 or 65 to 55mmHg.
- 4.
Although arterial blood sample during exercise allows determination of PaO2 and is useful for the interpretation of the exercise test, it is not essential for a correct evaluation of disability when considering VO2 max as the main factor for rating disability.
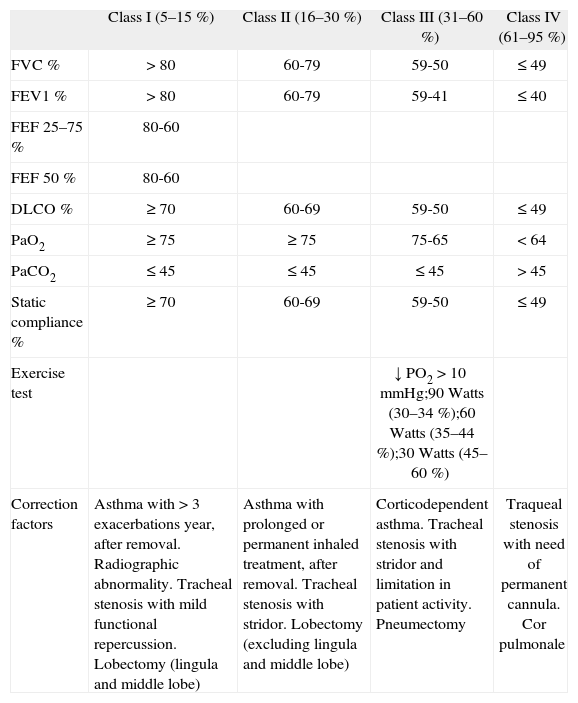
Scale of disability in Portugal 3
| Class I (5–15 %) | Class II (16–30 %) | Class III (31–60 %) | Class IV (61–95 %) | |
| FVC % | > 80 | 60-79 | 59-50 | ≤ 49 |
| FEV1 % | > 80 | 60-79 | 59-41 | ≤ 40 |
| FEF 25–75 % | 80-60 | |||
| FEF 50 % | 80-60 | |||
| DLCO % | ≥ 70 | 60-69 | 59-50 | ≤ 49 |
| PaO2 | ≥ 75 | ≥ 75 | 75-65 | < 64 |
| PaCO2 | ≤ 45 | ≤ 45 | ≤ 45 | > 45 |
| Static compliance % | ≥ 70 | 60-69 | 59-50 | ≤ 49 |
| Exercise test | ↓ PO2 > 10mmHg;90 Watts (30–34 %);60 Watts (35–44 %);30 Watts (45–60 %) | |||
| Correction factors | Asthma with > 3 exacerbations year, after removal. Radiographic abnormality. Tracheal stenosis with mild functional repercussion. Lobectomy (lingula and middle lobe) | Asthma with prolonged or permanent inhaled treatment, after removal. Tracheal stenosis with stridor. Lobectomy (excluding lingula and middle lobe) | Corticodependent asthma. Tracheal stenosis with stridor and limitation in patient activity. Pneumectomy | Traqueal stenosis with need of permanent cannula. Cor pulmonale |
Adapted from Tabela Nacional de Incapacidades por Acidentes de Trabalho e Doencas Profissionais 2007.
Also the proposed way of performing the CPET is questionable and not in accordance with the standardized ATS/ERS and ACCP 6,10,11 guidelines. In the Portuguese disability scale “the exercise testing is performed with successive loads of 30W, 60W and 90W (cycle ergometer or treadmill)”. Again, some doubts arise:
- 1.
The CPET can be performed on a cycle ergometer or treadmill, but only in the first is possible to accurately determine the load used.
- 2.
Both in the cycle ergometer and the treadmill, the best protocol to evaluate exercise limitation is the maximal incremental protocol, where the patient is evaluated continuously as the load (cycle ergometer) or speed / slope (on treadmill) is increased gradually.
- 3.
In incremental CPET the goal is to attain the maximum effort, assessed objectively by signs of exhaustion, depleted respiratory or cardiac reserve or respiratory exchange ratio (RER) ≥ 1.05. Functional capacity may be beyond the 90W, even if there is drop, at this load, of more than 10mmHg in PaO2.
- 4.
It is not clear whether what is required is an incremental CPET, passing through these three loads of 30, 60 and 90 Watts with determination of PaO2, or three constant CPET protocol for a load of 30, 60 and 90W with determination of arterial blood samples. Rather than evaluating disability or impairment, the constant work rate protocol is more appropriate for monitoring the clinical response after therapeutic intervention.
The CPET is, undoubtedly, the best test for an objective measurement of functional deficit in exercise, providing relevant information to assess disability in occupational respiratory diseases. The most pertinent parameter determined in incremental CPET is the VO2 max (maximum oxygen consumption) because it provides an objective measure of the patient functional capacity and it can be determined noninvasively in cycle ergometer or treadmill. The VO2 max is the parameter considered in disability evaluation by the American Thoracic Society, American Medical Association and the Spanish Secretaria de Estado de la Seguridad Social.
The current criteria used to rate disability in Portugal considers only a limited part of information given by CPET, a decrease of PaO2 equal or superior to 10mmHg in exercise, requiring arterial blood sample. Perhaps it is appropriate to reflect on these issues, so that we can use, more frequently and appropriately, the CPET to evaluate functional deficit and disability in Portugal.


