


A cross-sectional study was carried out with the objective of identifying nutrition habits and housing conditions as risk factors for respiratory problems in schoolchildren in Lisbon.
Material and methodsBetween October and December 2008, parents of 900 students of the elementary schools of Lisbon were invited to answer a questionnaire of the International Study of Asthma and Allergies in Childhood Program (ISAAC). The response rate was 40 %. Logistic regression was used in the analysis of results.
ResultsThe prevalence of asthma, allergic rhinitis and wheeze was 5.6 %, 43.0 % and 43.3 %, respectively. Risk factors independently associated with asthma were wheezing attacks, and dry cough at night not related to common cold in the last 12 months. Wheezing crises were found to affect children daily activities. Risk factors for wheeze were hay fever and the presence of a pet at home. A risk factor for rhinitis was cough at night. The frequent consumption of egg was also associated with increased risk of rhinitis.
ConclusionContrarily to asthma, the prevalence of allergic rhinitis and wheeze increased in comparison with previous ISAAC studies. Wheezing attacks were associated with asthma and hay fever was identified as a risk factor of manifesting wheezing symptoms. Having pets at home was pointed out as a significant risk factor for rhinitis, but not smoking exposure, mould, plush toys, diet (except egg consumption), breastfeeding or other conditions.
Com o objectivo de identificar hábitos alimentares e características habitacionais como factores de risco para a prevalência de problemas respiratórios na população escolar do 1.° ciclo da cidade de Lisboa foi realizado um estudo transversal.
Material e métodosDe Outubro a Dezembro de 2008, os pais de 900 alunos das escolas do 1° ciclo de Lisboa foram convidados a responder a um questionário similar ao do Programa Internacional de Estudo de Asma e Alergias na Infância (International Study of Asthma and Allergies in Childhood Program [ISAAC]). A taxa de resposta foi de 40 %. Aos resultados foi aplicada análise de regressão logística.
ResultadosA prevalência de asma, rinite alérgica e sibilância foi de 5,6 %, 43,0 % e 43,3 %, respectivamente. Os factores de risco independentemente associados à asma foram a sibilância e a tosse seca à noite, não relacionadas com sintomas de constipação comum nos últimos 12 meses. As crises de pieira foram consideradas susceptíveis de afectar as actividades diárias das crianças. Os factores de risco para sibilância foram a febre dos fenos e a presença de um animal de estimação em casa. A tosse durante a noite foi identificada como um factor de risco para a rinite. O consumo frequente de ovo foi também associado a um maior risco de manifestar rinite.
ConclusõesAo contrário da asma, a prevalência de rinite alérgica e sibilância aumentou em comparação com estudos anteriores ISAAC. Os ataques de pieira foram associados com os episódios asmáticos, e a febre dos fenos foi identificada como um factor de risco para a pieira. Ter animais de estimação em casa foi apontado como um factor de risco para a rinite, enquanto a exposição ao fumo, mofo, artigos de peluche, alimentação (excepto o consumo de ovos), amamentação ou outros parâmetros não representaram um factor de risco para a doença.
Asthma and allergic diseases are the leading cause of chronic illness in children and, for unknown reasons, are progressively increasing. 1–6 Although recent studies have shown that the genetic factors predispose people to allergic diseases, 7–9 the environmental factors have a significant influence on their occurrence and progression. Such factors include air pollution and several domestic triggers.10–13 The lifestyle, including the type of diet in early childhood, also plays an utmost role.14–16 As a consequence of diverse interactions between genetic and environmental risk factors, the prevalence rates show inconsistent results around the world.17–30 Written respiratory symptom questionnaires intended to determine the prevalence of asthma and allergies in children have been extensively used in epidemiological studies.31–35 The International Study of Asthma and Allergies in Childhood (ISAAC) was the first investigation carried out worldwide using standardised questionnaires in order to generate a consistent global map of childhood allergy.22,23,36 Portugal joined the ISAAC in 1993 with 5 local study centres (Lisbon, Oporto, Coimbra, Portimao and Funchal) questioning 13–14 year old children. In 3 of these centres (Lisbon, Portimao and Funchal), 6–7 year old children were also studied. 37,38 Besides the current trends in the prevalence of childhood asthma and asthma-like symptoms, the ISAAC program concluded that further population studies are urgently needed to discover more about the underlying mechanisms and the burden of these conditions.
With the objective of determining prevalence and risk factors of asthma and allergic diseases in Lisbon schoolchildren, as well of comparing the results with previous data obtained through the same protocol, a questionnaire-based study was conducted in elementary schools of the Portuguese capital city. Research on potential risk factors of asthma and allergic diseases can enhance our understanding of geographic differences and inform decisions on preventive strategies.
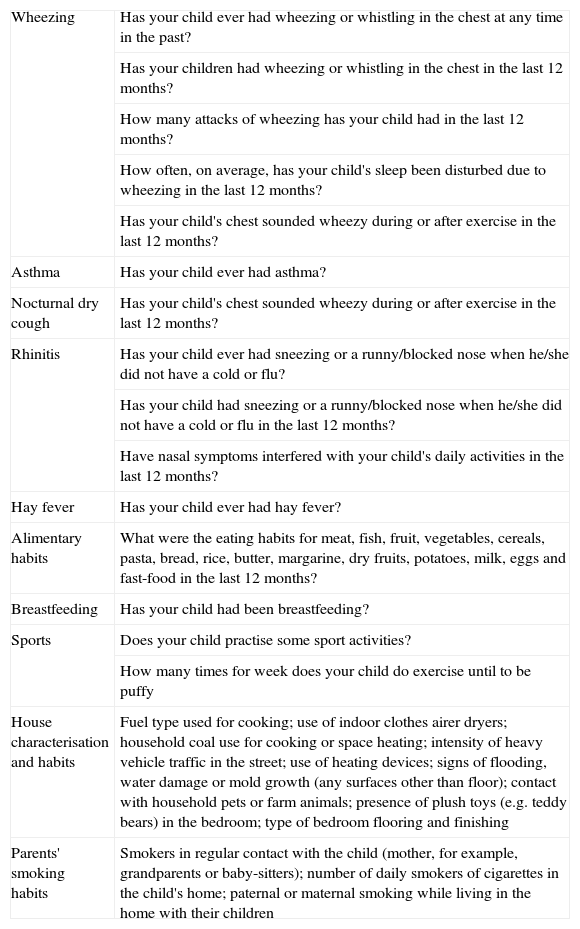
Material and methodsElementary school children were selected as the target population. Twenty two schools with a wide geographical coverage representing the Lisbon urban area were invited for participation in the study.39 Fourteen schools accepted to take part in the investigation. After obtaining consent from the school authorities, two classrooms from each school were selected for an indoor air quality monitoring program.40,41 A questionnaire, accompanied by an explanatory letter, was distributed to 900 children in every selected classroom. The questionnaire used in this study is the Portuguese version of the ISAAC program and had to be filled out by the parents. The questionnaire was adapted to facilitate the parents' responses, taking out some questions about medicine consumption, which did not constitute the objective of this study. The survey took place between October and December 2008 comprising children aged 5–12 years. A total of 342 questionnaires were returned. They included questions on the frequency of respiratory symptoms and allergy occurrence in the child, physical activity, socio-demographic characteristics, housing conditions, and other possible sources of indoor air pollution (Table 1). Among the factors related to lifestyle, particular attention was paid to the child's exposure to tobacco smoke, the way of feeding the child during the first months of its life (breast-feeding, artificial milk feeding), and the current type of diet. The manually written answers were transferred to a computer, codified, and confirmed by two independent persons. Multivariate logistic regression models controlling for possible confounders were used to evaluate variables associated with asthma and allergic symptoms, and adjusted odds ratios (ORs and 95 % confidence intervals, CI) were calculated.
Questions in the questionnaire used in this study
| Wheezing | Has your child ever had wheezing or whistling in the chest at any time in the past? |
| Has your children had wheezing or whistling in the chest in the last 12 months? | |
| How many attacks of wheezing has your child had in the last 12 months? | |
| How often, on average, has your child's sleep been disturbed due to wheezing in the last 12 months? | |
| Has your child's chest sounded wheezy during or after exercise in the last 12 months? | |
| Asthma | Has your child ever had asthma? |
| Nocturnal dry cough | Has your child's chest sounded wheezy during or after exercise in the last 12 months? |
| Rhinitis | Has your child ever had sneezing or a runny/blocked nose when he/she did not have a cold or flu? |
| Has your child had sneezing or a runny/blocked nose when he/she did not have a cold or flu in the last 12 months? | |
| Have nasal symptoms interfered with your child's daily activities in the last 12 months? | |
| Hay fever | Has your child ever had hay fever? |
| Alimentary habits | What were the eating habits for meat, fish, fruit, vegetables, cereals, pasta, bread, rice, butter, margarine, dry fruits, potatoes, milk, eggs and fast-food in the last 12 months? |
| Breastfeeding | Has your child had been breastfeeding? |
| Sports | Does your child practise some sport activities? |
| How many times for week does your child do exercise until to be puffy | |
| House characterisation and habits | Fuel type used for cooking; use of indoor clothes airer dryers; household coal use for cooking or space heating; intensity of heavy vehicle traffic in the street; use of heating devices; signs of flooding, water damage or mold growth (any surfaces other than floor); contact with household pets or farm animals; presence of plush toys (e.g. teddy bears) in the bedroom; type of bedroom flooring and finishing |
| Parents' smoking habits | Smokers in regular contact with the child (mother, for example, grandparents or baby-sitters); number of daily smokers of cigarettes in the child's home; paternal or maternal smoking while living in the home with their children |
The sample population comprised 342 schoolchildren between 5 and 12 years, although 92 % of the total was included in the age group of 6–8 years. No dimorphic differences were found concerning the frequency of allergies, therefore no division by gender was applied in further analysis. The percentage of children with wheezing or whistling in the chest was 43.3 %. Asthma prevalence was 5.6 %. Symptoms of allergic rhinitis were reported for 42.9 % of children.
Almost 9.5 % of children were born abroad. The proportion of parents with elementary education degree was 20 %, 56 % reported having a secondary degree and 20 % were university graduates. Housing characteristics of respondents were evaluated (Table 2): about 33 % of the families lived near streets with heavy traffic, 23 % used drying clothes airers and indoor drying racks for the drying of washing and laundry, and only 3 % of children's bedrooms had carpeting. Gas use as a cooking fuel was asserted by 84 % of respondents. Almost 23 % of the families stated having a furry pet at home, whereas 62 % reported plush toys in the child's bedroom. The appearance or detection of moulds and water damage within the past 12 months occurred in 19 % of the homes, and 23 % of children had been exposed to environmental tobacco smoke during the first year of life. More than half of all children lived with one or more smokers in their homes.
Housing characteristics and environmental factor exposure in children living in Lisbon
| Housing characteristics | Definition | % |
| Cooking equipments | Cooking fuel type: | |
| - Electricity | 5.6 | |
| - Gas | 83.9 | |
| - Other | 0.0 | |
| Indoor laundry drying | The use of indoor clothes airer dryers | 22.8 |
| Indoor coal use | The use of coal in a household for cooking or space heating | 0.0 |
| Pollution source near the house | Heavy vehicle traffic in the street: | |
| - All day long | 9.6 | |
| - Frequently | 23.7 | |
| - Rarely | 47.9 | |
| - Never | 17.5 | |
| Use of home heating devices | The use of any of the following heating devices: | |
| - Electricity | 43.3 | |
| - Gas | 12.6 | |
| - Wood | 9.4 | |
| - Other | 1.7 | |
| Mould in the past 12 months | Signs of flooding, water damage or mold growth (any surfaces other than food) | 19.0 |
| Pet keeping | Refers to the feeding in a household dogs, cats or farm animals: | |
| - Cats in the past 12 months | 10.8 | |
| - Cats in the first year of life | 8.5 | |
| - Dogs in the past 12 months | 22.8 | |
| - Dogs in the first year of life | 9.3 | |
| - Contact during the first year of life with farm animals | 12.9 | |
| Plush toys | Presence of plush toys (e.g. teddy bears) in the bedrooms | 62.3 |
| Bedroom flooring | Types of bedroom flooring: | |
| - Carpet | 2.6 | |
| - Wooden | 70.5 | |
| - Tiled | 14.3 | |
| - Other | 8.2 | |
| Bedroom walls | Types of bedroom finishes: | |
| - Painting | 95.0 | |
| - Wallpaper | 0.6 | |
| Early-life exposure to tobacco smoke in the 1st year | Smokers in regular contact with the child (mother, for example, grandparents or baby-sitters) | 23.0 |
| Current smokers in the household | Number of daily smokers of cigarettes in the child's home: | |
| - None | 43.9 | |
| - One | 35.1 | |
| - Two | 15.8 | |
| - Three | 2.6 | |
| - Four or more | 2.0 | |
| Parents smoking | Paternal or maternal smoking while living in the home with their children: | |
| - Mother | 30.4 | |
| - Father | 36.5 | |
The results of the logistic regression analysis reveal that the questions “How many wheezing attacks did your child had during the past year?” and “Has your child had ever dry cough at night not associated with common cold in the last 12 months?” are statistically significant predictors of asthma. Concerning the first question, the estimate of the probability of occurrence of childhood asthma is 10 times superior for the answer category “1 to 3” (one to three wheezing attacks in the past year) than for those responding “none” (ODs = 10.07; CI = 2.98, 33.96). Children in the category “4 to 12” have approximately a 20 times higher chance of developing the disease compared with those in the category “none” (ODs = 19.88; CI = 4.22, 93.54). Occurrence of dry cough at night increases by almost 6 times the probability of asthma manifestation (ODs = 5.77; CI = 1.20, 27.70).
For the variable represented by the question “During the last 12 months, have the wheezing problems affected your child's daily activities?”, the odds ratio between the category “did not affect daily activity” and the category “daily activity affected a little” is 2.55 (CI = 1.28, 5.08). This means that the point estimate of the probability of occurrence of wheezing is 2.55 higher for those responding “did not affect” than for those answering “affected a little”. The odds ratio between the categories “did not affect daily activity” and “daily activity affected moderately” is approximately 27 (CI = 6.17, 126.36). The point estimate of the probability of occurrence of wheezing is 13 times higher for positive answers to “Has your child ever had hay fever?” (ODs = 13.02; CI = 1.52, 109.5). (CI = 1.27, 10.57). Children who had a pet in their home during the last 12 months appear to have a higher risk of developing wheezing symptoms (ODs = 3.66; CI = 1.27, 10.57).
The occurrence of dry cough at night not associated with common cold in the last 12 months was also positively associated with rhinitis (ODs = 2.77; CI = 1.19, 6.44). The point estimate of the probability for allergic rhinitis is approximately 145 times higher among children with sneezing crisis, runny nose or nasal congestion not associated with common cold in relation to those without these symptoms (ODs = 145.47; CI = 53.53, 395.28). Among diet variables, the only statistical significant relationship found was for egg consumption, with frequent egg eaters having a 90 % higher risk for allergic rhinitis than those that were not (OR = 0.10, CI = 0.01, 0.54).
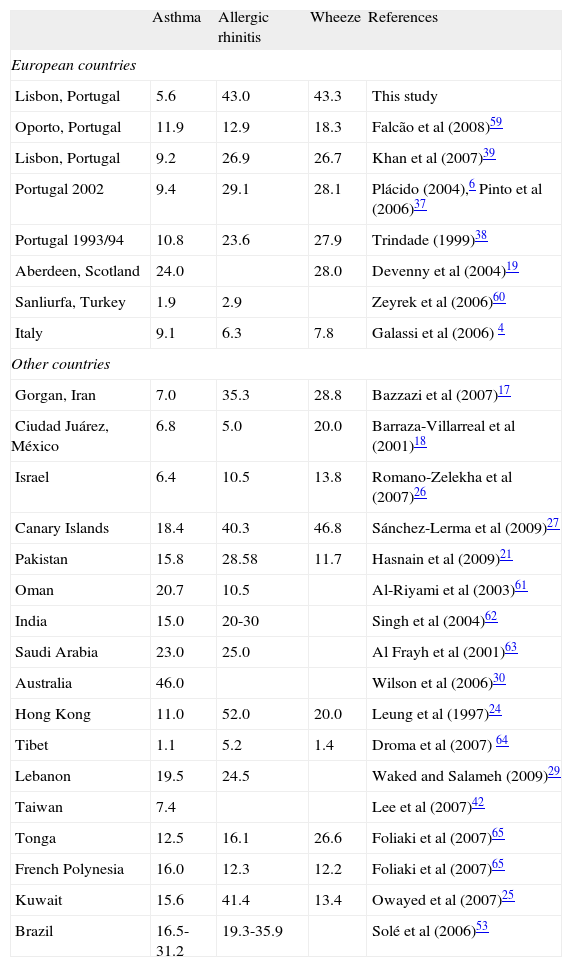
DiscussionThe male to female ratio for the diagnosis of asthma has narrowed considerably in the past 35 years, with almost complete disappearance of the previous male predominance. 19 In comparison with previous studies in Portugal, schoolchildren living in Lisbon show a trend to reduction in the current prevalence of asthma (Table 3). This might be explained by a better control of the disease through educational measures and improved preventive treatment to better control of the disease, taking into account that more children are now using inhaled corticosteroids. These findings are sustained by other studies that used the ISAAC questionnaire.26 The ISAAC found the greatest prevalence of asthma in Australia and New Zealand (29.7 %), followed by North America (24.4 %) and Latin America (17.0 %). 1 In contrast to our study, a trend towards an increase in asthma has been observed in other regions: Taiwan,42 United Kingdom,19 Hong Kong,24 US,43 Australia,30 Brasil,44 Austria,45 and Spain.46 However, signs indicative of a halt in the rising trend in asthma prevalence have been found in other recent investigations. 25,26,47–50 According to Bazzazi et al 17 it is unresolved why the disparities in the prevalence of asthma and allergic disorders are so large. Two overlapping though competing theories have related changes in environmental factors to observed trend profiles in asthma and allergy epidemiology. The oldest theory, the “hygiene hypothesis”, claims that modifications in the infectious environment and in the pattern of microbial exposure of children associated with westernisation are decisive factors contributing to the increasing severity and prevalence of atopic disorders. According to this theory, environmental exposures that promote a generalised suppression of Th2 cytokines and trigger strong Th1 responses are becoming progressively less common.51 The most recent theory, the “immunotolerance hypothesis”, claims that early high levels of exposure to allergens reduce risk by potentiating the regulatory capacity of the immune system.52
Prevalence of allergy symptoms worldwide (values are given in %)
| Asthma | Allergic rhinitis | Wheeze | References | |
| European countries | ||||
| Lisbon, Portugal | 5.6 | 43.0 | 43.3 | This study |
| Oporto, Portugal | 11.9 | 12.9 | 18.3 | Falcão et al (2008)59 |
| Lisbon, Portugal | 9.2 | 26.9 | 26.7 | Khan et al (2007)39 |
| Portugal 2002 | 9.4 | 29.1 | 28.1 | Plácido (2004),6 Pinto et al (2006)37 |
| Portugal 1993/94 | 10.8 | 23.6 | 27.9 | Trindade (1999)38 |
| Aberdeen, Scotland | 24.0 | 28.0 | Devenny et al (2004)19 | |
| Sanliurfa, Turkey | 1.9 | 2.9 | Zeyrek et al (2006)60 | |
| Italy | 9.1 | 6.3 | 7.8 | Galassi et al (2006) 4 |
| Other countries | ||||
| Gorgan, Iran | 7.0 | 35.3 | 28.8 | Bazzazi et al (2007)17 |
| Ciudad Juárez, México | 6.8 | 5.0 | 20.0 | Barraza-Villarreal et al (2001)18 |
| Israel | 6.4 | 10.5 | 13.8 | Romano-Zelekha et al (2007)26 |
| Canary Islands | 18.4 | 40.3 | 46.8 | Sánchez-Lerma et al (2009)27 |
| Pakistan | 15.8 | 28.58 | 11.7 | Hasnain et al (2009)21 |
| Oman | 20.7 | 10.5 | Al-Riyami et al (2003)61 | |
| India | 15.0 | 20-30 | Singh et al (2004)62 | |
| Saudi Arabia | 23.0 | 25.0 | Al Frayh et al (2001)63 | |
| Australia | 46.0 | Wilson et al (2006)30 | ||
| Hong Kong | 11.0 | 52.0 | 20.0 | Leung et al (1997)24 |
| Tibet | 1.1 | 5.2 | 1.4 | Droma et al (2007) 64 |
| Lebanon | 19.5 | 24.5 | Waked and Salameh (2009)29 | |
| Taiwan | 7.4 | Lee et al (2007)42 | ||
| Tonga | 12.5 | 16.1 | 26.6 | Foliaki et al (2007)65 |
| French Polynesia | 16.0 | 12.3 | 12.2 | Foliaki et al (2007)65 |
| Kuwait | 15.6 | 41.4 | 13.4 | Owayed et al (2007)25 |
| Brazil | 16.5-31.2 | 19.3-35.9 | Solé et al (2006)53 | |
Children with sneezing crisis, runny nose or nasal congestion not associated with common cold were 43.0 %. Regarding the last year rhinitis prevalence in this age group, it was estimated to be 39.5 %. The prevalence of this allergic disease in Lisbon is greater than the mean estimated national prevalence. Since Portugal is a country with diverse geographic areas, the divergent prevalence ratios obtained in different cities can be explained by the type of weather, the level of air pollution and the diverse levels of contact to allergens. Lee et al42 surveyed an increased prevalence of allergic rhinitis among children in Hong Kong from 1995 to 2001. The same rising trend was observed among Israeli adolescents.26 In Brazil, last year rhinitis prevalence in schoolchildren and adolescents was found to fall in wide ranges: 1.5-41.8 % and 3.2-66.6 %, respectively. 53 In Italy, the prevalence of rhinitis symptoms in the past 12 months increased from 13.8 to 18.9 % and from 31.6 to 35.1 % among children (6–7 years old) and adolescents (13–14 years old), respectively, between 1994 and 2002.4
The proportion of children with respiratory symptoms reporting wheeze experienced a significant increase between 1993/94 and 2008 (Table 3). However, the prevalence of wheezing symptoms in the last 12 months was only 15 %. The worldwide prevalence of current wheeze studied in 155 centres ranged from 2.1 to 32.2 %.23 In Australia, a 26 % decrease in wheezing in the past 12 months was found in younger children between 1993 and 2002.54 In Spain, the prevalence of current wheeze in 13–14 year old children did not change from 1994–1995 to 2002–2003.46 In Belgium, there was no clear change in asthma, but wheeze decreased from 1996 to 2002. 16 Several other studies from Great Britain, Germany, Italy and Denmark conducted in the last decade reported dissimilar findings of an increase in the prevalence of asthma and of wheeze in the past 12 months.4,19,55,56
Frequent consumption of egg was also associated with increased risk of respiratory symptoms among schoolchildren in Taipei.57 Allergic reactions to food are either immunoglobulin (IgE) mediated or non-IgE-mediated. Persons who are hereditarily predisposed to atopy produce specific IgE antibodies to certain proteins to which they are exposed. These antibodies bind to mast cells and other cells in body tissues and to basophiles circulating in the blood stream. When a food protein is ingested, the IgE recognises it on the surface of these cells; mediators (e.g., histamine) are released, and symptoms arise. Besides the skin and gastrointestinal tract, the symptoms of IgE-mediated reactions usually involve the respiratory system.58 Eggs are among the food most commonly causing these allergic reactions in children.
No associations with any of the other dietary factors were found. A significant protective effect of breastfeeding against current respiratory allergies in children was not observed in this study. Besides pets, no statistically significant relationship was found with other housing conditions.
Our study had some limitations; namely recalling bias in cross-sectional questionnaires and the lack of objective laboratory measures. However, most estimates of asthma, wheeze and rhinitis have been based on data from questionnaires with questions concerning symptoms or preceding physician diagnosis.
ConclusionsContrarily to asthma, a statistically significant increase in the prevalence of rhinitis and wheeze was observed among primary schoolchildren in Lisbon. Differences in prevalence obtained in several studies may point out exposure to different risk factors, as well as variable racial, environmental, and socioeconomic conditions, heterogeneous diagnostic criteria, or a true increase in the prevalence of allergic diseases. In this study, wheezing attacks were associated with asthma and hay fever was identified as a risk factor of manifesting wheezing symptoms. Children with dry cough at night should be evaluated for both rhinitis and asthma, and a combined strategy should be ideally used to treat the upper and lower airway diseases in terms of efficacy and safety. Having pets at home was pointed out as a significant risk factor for rhinitis, but not smoking exposure, mould, plush toys, diet (except egg consumption), breastfeeding or other conditions. The results support the observation that deep changes in the epidemiologic dynamics of asthma and allergic diseases are occurring worldwide, demanding ample, continuous, epidemiologic monitoring. Future studies, such as birth cohorts, are warranted to evaluate risk and protective factors and to continue surveying the features of the prevalence of asthma and allergic diseases in Portugal. Research on potential risk factors of asthma and respiratory allergies can enhance our understanding of geographic differences and support decisions on preventive strategies.
Conflict of interestAuthors declare that they don't have any conflict of interest.
This study was supported by the project “Impact of indoor environment on human health” (PTDC/SAU-ESA/65597/2006). Priscilla Pegas acknowledges the Portuguese Science Foundation for the Ph.D. scholarship (SFRH/BD/45233/2008). The authors are also grateful to all schoolchildren and their parents for their participation and the teachers and principals for their helpful collaboration.


