

The PAQ questionnaire (Physical Activity Questionnaire - Kowalski, Crocker, Donen) is a self-administered 7-day recall validated questionnaire that measures physical activity levels in young people. A final activity score is obtained (1 indicates low and 5 indicates high physical activity level).
Our aim was to determine whether there was any difference between the level of physical activity of children with controlled allergic disease and healthy children.
Patients and methodsWe used the PAQ questionnaire with a group of asthmatic children attending hospital outpatient clinic and a group of healthy children matched for age.
Results155 children with allergic disease (median age of 11 years; 63% males) and 158 healthy controls (median age of 10 years; 46% males) answered the questionnaire.
There were no differences in the overall level of physical activity, estimated by PAQ score, between allergic and healthy children (2,40±0,7 vs 2,48±0,62; p=0,32). Performance in physical education classes and after school sports activity was found to be different between the study groups; healthy children were more active (p=0,011) and did more sports between 6 and 10 pm (p=0,036). No other statistically significant differences were found between the study groups.
ConclusionDespite the fact that a majority of the parents of allergic children stated that their child's disease was a barrier to physical activity, in our study there seems to be no difference between the level of physical activity of controlled asthmatic children and their healthy peers.
O questionário PAQ (Physical Activity Questionnaire - Kowalski, Crocker, Donen) é um questionário validado, que mede os níveis de atividade física em jovens através de perguntas referentes aos últimos 7 dias. É obtido um resultado final (1 indica um nível de atividade física baixo e 5 um nível elevado).
O nosso objetivo foi determinar se existe alguma diferença entre o nível de atividade física de crianças com doenças alérgicas controladas e em crianças saudáveis.
Doentes e métodosO questionário PAQ foi aplicado a um grupo de crianças asmáticas que frequentavam a consulta externa e a um grupo de crianças saudáveis, de idade equivalente.
ResultadosCento e cinquenta e cinco crianças com doenças alérgicas (idade média de 11 anos; 53% do sexo masculino) e 158 controlos saudáveis (idade média de 10 anos; 46% do sexo masculino) responderam ao questionário.
Não se verificaram diferenças no nível global de atividade física estimado pelo score PAQ entre crianças asmáticas e saudáveis (2,40±0,7 vs 2,48±0,62; p=0,32). Verificou-se que o desempenho nas aulas de educação física e que a atividade desportiva depois das aulas era diferente entre os grupos de estudo: as crianças saudáveis eram mais participativas nas aulas (p=0,011) e faziam mais desporto entre as 18-22 horas (p=0,036). Não foram verificadas quaisquer outras diferenças significativas entre os grupos.
ConclusãoApesar do facto da maioria dos pais de crianças asmáticas afirmar que a doença dos seus filhos era uma barreira à atividade física, no nosso estudo não parece haver diferenças entre o nível de atividade física das crianças asmáticas controladas e dos seus pares.
Exercise tolerance and potential reduced work capacity in children with asthma are still a subject of debate. Results from trials with regard to the possible benefits and risks of exercise in asthmatic children and adolescents have shown contradictory results because exercise may trigger allergic systemic, cutaneous and respiratory symptoms, such as exercise-induced asthma.
However, on the other hand, regular exercise and participation in sports are considered useful in the management of asthma, since physical training improves cardiopulmonary fitness, neuromuscular coordination, self confidence and health-related quality of life.1,2 Regular physical activity appears to induce beneficial immunological changes, thereby reducing allergic inflammation.3 Oxygen consumption, maximum heart rate and work capacity are all increased significantly during exercise4 and asthmatics, during exercise, present higher tidal volumes and lower respiratory rates compared to healthy controls.5 In addition, physical training leads to significant reductions in the use of both inhaled and oral steroids.6
There was also found an association between asthma and both obesity and low levels of physical activity.7 Moreover, asthma impacts negatively on mental health, while higher levels of physical activity improves it.7 There is solid evidence to reassure physicians on the work capacity of asthmatics and to encourage them to take up sports.5
Data about limited physical fitness in asthmatic children and adolescents are contradictory. The aim of this study was to determine any differences between the level of physical activity of controlled allergic patients and their healthy peers.
Materials and methodsStudy typeDescriptive comparative study. Participants were divided into two groups: a group of children with asthma and a control group of healthy children. PAQ questionnaire was applied to both groups and results were compared. The evaluation took place during school time (November 2011) in an urban area in the north of Portugal.
Physical activity questionnaire (PAQ Family)The “PAQ family” (Physical Activity Questionnaire for Older Children – PAQ-C and Physical Activity Questionnaire for Adolescents – PAQ-A)8 are a family of self-administered 7-day recall questionnaires designed by the Canadian University of Saskatchewan to provide a general measurement of physical activity in youth. The PAQ-C is appropriate for elementary school aged children (approximately ages 8–14) and the PAQ-A is appropriate for high school students (approximately ages 14–20).
The PAQ-A is made up of nine questions that assess different aspects of physical activity on a 5-point scale. It includes questions about the physical activity of the children in the previous 7 days, during their spare time and physical education classes and at different times during school day (afternoon, lunch and evening) and at weekends. Physical activity during weekdays is addressed in the last two questions. Any circumstance (such as illness) that had prevented them from doing any normal physical activity during the previous week is addressed in question 9.
The final score (the average of individual questions) establishes a graduated level of physical activity performed by each child (a score of 1 indicates low physical activity, whereas a score of 5 indicates high physical activity).8 The only difference between the PAQ-C and PAQ-A is that the former has an extra question about physical activity during recess (10 questions in total compared to 9 questions in the PAQ-A).
Physical activity measured by PAQ finds associations with indicators of adiposity, bone mineral density, heart rate variability and certain physiological indicators (sports competition, body satisfaction, anxiety). PAQ identifies at what time of the day and the week that children are most active.8
The questionnaire was translated into Portuguese by members of the research team. Since the only difference between questionnaires PAQ-A and PAQ-C is the question about activity during recess, it was decided for the sake of convenience to use the PAQ-A questionnaire for the entire sample.
ParticipantsParticipants were divided into two groups: a group of children with controlled asthma and a group of healthy children matched for age. Children in the allergic group were attending outpatient hospital (Centro Hospitalar Médio Ave – Vila Nova de Famalicão, Portugal), had a confirmed clinical diagnosis of asthma and had been asymptomatic for the previous six months. Participants on the control group were recruited from a local public high school.
Permission was obtained from the Hospital Ethics Committee, the board of the school and written informed consent was signed by all parents.
MethodsThe answers in both groups were compared. Children with uncontrolled asthma and those who had answered “yes” to question 9 were excluded from the study.
Statistical analysisData was processed with SPSS® 17.0. Chi-square and Pearson's Exact Test were used for categorical variables and T-student test for independent samples. It was considered a significance level <0,05.
ResultsA total of 323 questionnaires were collected. After using exclusion criteria, a final sample of 155 controlled asthmatic and 158 healthy controls was obtained (313 valid questionnaires).
The median age of allergic patients was 11 years (5–18) and 62.6% (97) were male. Healthy controls had a median age of 10 years (8–18) and 46% (73) were males.
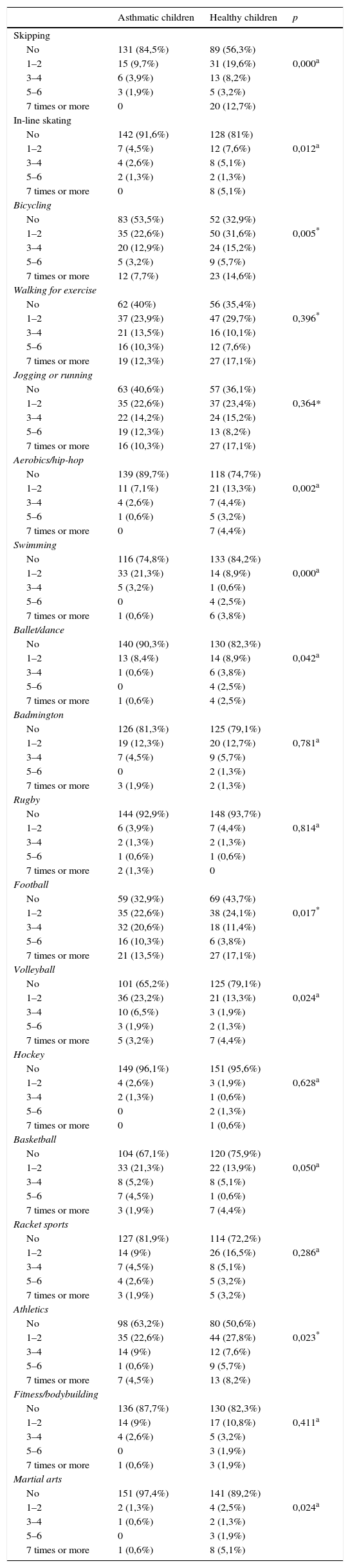
With regard to question 1 (how often the child had played each of the sports in the previous week), results are listed in Table 1. We found statistically significant differences in skipping (p=0,000), in-line skating (p=0,012), cycling (p=0,005), aerobics/hip-hop (p=0,002), swimming (p=0,000), ballet/dance (p=0,042), football (p=0,017), volleyball (p=0,024), athletics (p=0,023) and martial arts (p=0,024).
Modalities practiced. It shows how often the different modalities were practiced in the last 7 days (question 1): none, 1–2 times last week, 3–4 times, 5–6 times or more than 7 times (meaning every day).
| Asthmatic children | Healthy children | p | |
|---|---|---|---|
| Skipping | |||
| No | 131 (84,5%) | 89 (56,3%) | |
| 1–2 | 15 (9,7%) | 31 (19,6%) | 0,000a |
| 3–4 | 6 (3,9%) | 13 (8,2%) | |
| 5–6 | 3 (1,9%) | 5 (3,2%) | |
| 7 times or more | 0 | 20 (12,7%) | |
| In-line skating | |||
| No | 142 (91,6%) | 128 (81%) | |
| 1–2 | 7 (4,5%) | 12 (7,6%) | 0,012a |
| 3–4 | 4 (2,6%) | 8 (5,1%) | |
| 5–6 | 2 (1,3%) | 2 (1,3%) | |
| 7 times or more | 0 | 8 (5,1%) | |
| Bicycling | |||
| No | 83 (53,5%) | 52 (32,9%) | |
| 1–2 | 35 (22,6%) | 50 (31,6%) | 0,005* |
| 3–4 | 20 (12,9%) | 24 (15,2%) | |
| 5–6 | 5 (3,2%) | 9 (5,7%) | |
| 7 times or more | 12 (7,7%) | 23 (14,6%) | |
| Walking for exercise | |||
| No | 62 (40%) | 56 (35,4%) | |
| 1–2 | 37 (23,9%) | 47 (29,7%) | 0,396* |
| 3–4 | 21 (13,5%) | 16 (10,1%) | |
| 5–6 | 16 (10,3%) | 12 (7,6%) | |
| 7 times or more | 19 (12,3%) | 27 (17,1%) | |
| Jogging or running | |||
| No | 63 (40,6%) | 57 (36,1%) | |
| 1–2 | 35 (22,6%) | 37 (23,4%) | 0,364* |
| 3–4 | 22 (14,2%) | 24 (15,2%) | |
| 5–6 | 19 (12,3%) | 13 (8,2%) | |
| 7 times or more | 16 (10,3%) | 27 (17,1%) | |
| Aerobics/hip-hop | |||
| No | 139 (89,7%) | 118 (74,7%) | |
| 1–2 | 11 (7,1%) | 21 (13,3%) | 0,002a |
| 3–4 | 4 (2,6%) | 7 (4,4%) | |
| 5–6 | 1 (0,6%) | 5 (3,2%) | |
| 7 times or more | 0 | 7 (4,4%) | |
| Swimming | |||
| No | 116 (74,8%) | 133 (84,2%) | |
| 1–2 | 33 (21,3%) | 14 (8,9%) | 0,000a |
| 3–4 | 5 (3,2%) | 1 (0,6%) | |
| 5–6 | 0 | 4 (2,5%) | |
| 7 times or more | 1 (0,6%) | 6 (3,8%) | |
| Ballet/dance | |||
| No | 140 (90,3%) | 130 (82,3%) | |
| 1–2 | 13 (8,4%) | 14 (8,9%) | 0,042a |
| 3–4 | 1 (0,6%) | 6 (3,8%) | |
| 5–6 | 0 | 4 (2,5%) | |
| 7 times or more | 1 (0,6%) | 4 (2,5%) | |
| Badmington | |||
| No | 126 (81,3%) | 125 (79,1%) | |
| 1–2 | 19 (12,3%) | 20 (12,7%) | 0,781a |
| 3–4 | 7 (4,5%) | 9 (5,7%) | |
| 5–6 | 0 | 2 (1,3%) | |
| 7 times or more | 3 (1,9%) | 2 (1,3%) | |
| Rugby | |||
| No | 144 (92,9%) | 148 (93,7%) | |
| 1–2 | 6 (3,9%) | 7 (4,4%) | 0,814a |
| 3–4 | 2 (1,3%) | 2 (1,3%) | |
| 5–6 | 1 (0,6%) | 1 (0,6%) | |
| 7 times or more | 2 (1,3%) | 0 | |
| Football | |||
| No | 59 (32,9%) | 69 (43,7%) | |
| 1–2 | 35 (22,6%) | 38 (24,1%) | 0,017* |
| 3–4 | 32 (20,6%) | 18 (11,4%) | |
| 5–6 | 16 (10,3%) | 6 (3,8%) | |
| 7 times or more | 21 (13,5%) | 27 (17,1%) | |
| Volleyball | |||
| No | 101 (65,2%) | 125 (79,1%) | |
| 1–2 | 36 (23,2%) | 21 (13,3%) | 0,024a |
| 3–4 | 10 (6,5%) | 3 (1,9%) | |
| 5–6 | 3 (1,9%) | 2 (1,3%) | |
| 7 times or more | 5 (3,2%) | 7 (4,4%) | |
| Hockey | |||
| No | 149 (96,1%) | 151 (95,6%) | |
| 1–2 | 4 (2,6%) | 3 (1,9%) | 0,628a |
| 3–4 | 2 (1,3%) | 1 (0,6%) | |
| 5–6 | 0 | 2 (1,3%) | |
| 7 times or more | 0 | 1 (0,6%) | |
| Basketball | |||
| No | 104 (67,1%) | 120 (75,9%) | |
| 1–2 | 33 (21,3%) | 22 (13,9%) | 0,050a |
| 3–4 | 8 (5,2%) | 8 (5,1%) | |
| 5–6 | 7 (4,5%) | 1 (0,6%) | |
| 7 times or more | 3 (1,9%) | 7 (4,4%) | |
| Racket sports | |||
| No | 127 (81,9%) | 114 (72,2%) | |
| 1–2 | 14 (9%) | 26 (16,5%) | 0,286a |
| 3–4 | 7 (4,5%) | 8 (5,1%) | |
| 5–6 | 4 (2,6%) | 5 (3,2%) | |
| 7 times or more | 3 (1,9%) | 5 (3,2%) | |
| Athletics | |||
| No | 98 (63,2%) | 80 (50,6%) | |
| 1–2 | 35 (22,6%) | 44 (27,8%) | 0,023* |
| 3–4 | 14 (9%) | 12 (7,6%) | |
| 5–6 | 1 (0,6%) | 9 (5,7%) | |
| 7 times or more | 7 (4,5%) | 13 (8,2%) | |
| Fitness/bodybuilding | |||
| No | 136 (87,7%) | 130 (82,3%) | |
| 1–2 | 14 (9%) | 17 (10,8%) | 0,411a |
| 3–4 | 4 (2,6%) | 5 (3,2%) | |
| 5–6 | 0 | 3 (1,9%) | |
| 7 times or more | 1 (0,6%) | 3 (1,9%) | |
| Martial arts | |||
| No | 151 (97,4%) | 141 (89,2%) | |
| 1–2 | 2 (1,3%) | 4 (2,5%) | 0,024a |
| 3–4 | 1 (0,6%) | 2 (1,3%) | |
| 5–6 | 0 | 3 (1,9%) | |
| 7 times or more | 1 (0,6%) | 8 (5,1%) | |
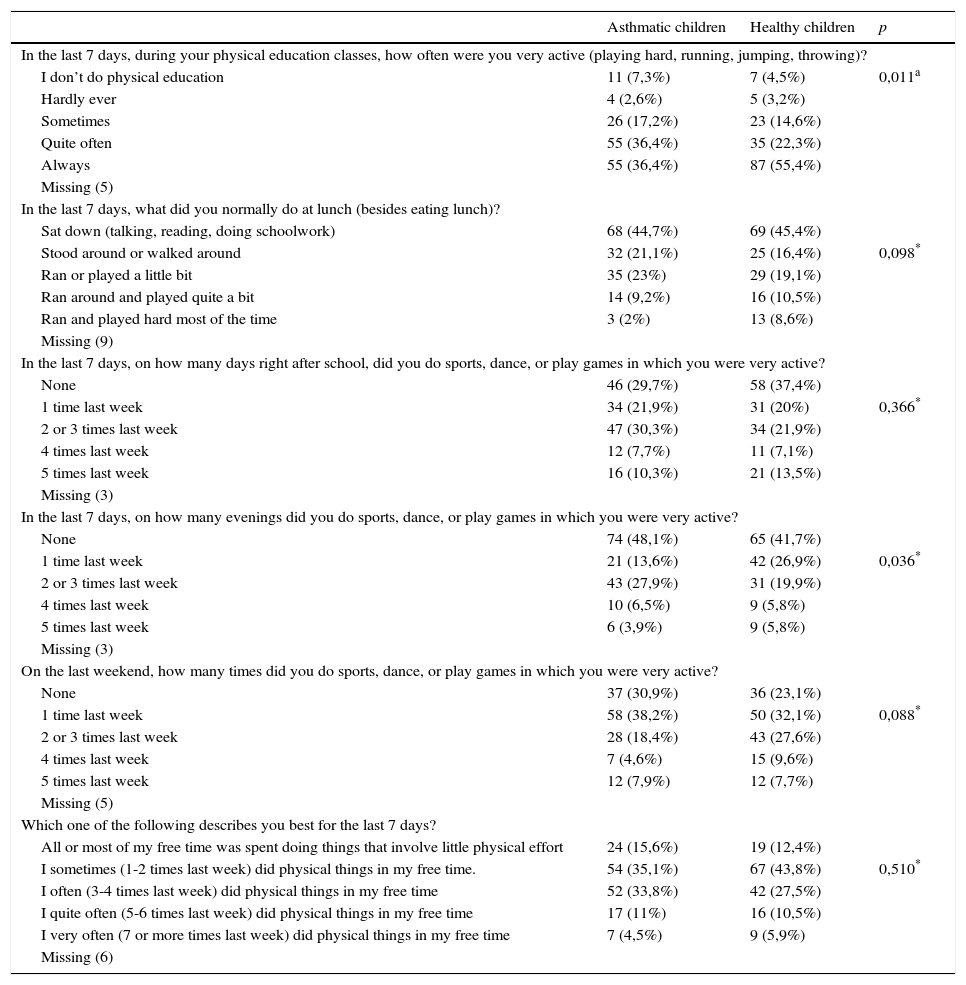
In relation to questions 2–7 (Table 2), which define the pattern of physical activity for these children, the only differences found concerned performance in physical education classes (healthy children tend to be more active; p=0,011) and in after-school sports activities (healthy children tend to play more sports between 6 and 10 p.m.; p=0,036).
Exercise distribution during the day. It shows how the exercise was distributed during the day (question 2 to 7).
| Asthmatic children | Healthy children | p | |
|---|---|---|---|
| In the last 7 days, during your physical education classes, how often were you very active (playing hard, running, jumping, throwing)? | |||
| I don’t do physical education | 11 (7,3%) | 7 (4,5%) | 0,011a |
| Hardly ever | 4 (2,6%) | 5 (3,2%) | |
| Sometimes | 26 (17,2%) | 23 (14,6%) | |
| Quite often | 55 (36,4%) | 35 (22,3%) | |
| Always | 55 (36,4%) | 87 (55,4%) | |
| Missing (5) | |||
| In the last 7 days, what did you normally do at lunch (besides eating lunch)? | |||
| Sat down (talking, reading, doing schoolwork) | 68 (44,7%) | 69 (45,4%) | |
| Stood around or walked around | 32 (21,1%) | 25 (16,4%) | 0,098* |
| Ran or played a little bit | 35 (23%) | 29 (19,1%) | |
| Ran around and played quite a bit | 14 (9,2%) | 16 (10,5%) | |
| Ran and played hard most of the time | 3 (2%) | 13 (8,6%) | |
| Missing (9) | |||
| In the last 7 days, on how many days right after school, did you do sports, dance, or play games in which you were very active? | |||
| None | 46 (29,7%) | 58 (37,4%) | |
| 1 time last week | 34 (21,9%) | 31 (20%) | 0,366* |
| 2 or 3 times last week | 47 (30,3%) | 34 (21,9%) | |
| 4 times last week | 12 (7,7%) | 11 (7,1%) | |
| 5 times last week | 16 (10,3%) | 21 (13,5%) | |
| Missing (3) | |||
| In the last 7 days, on how many evenings did you do sports, dance, or play games in which you were very active? | |||
| None | 74 (48,1%) | 65 (41,7%) | |
| 1 time last week | 21 (13,6%) | 42 (26,9%) | 0,036* |
| 2 or 3 times last week | 43 (27,9%) | 31 (19,9%) | |
| 4 times last week | 10 (6,5%) | 9 (5,8%) | |
| 5 times last week | 6 (3,9%) | 9 (5,8%) | |
| Missing (3) | |||
| On the last weekend, how many times did you do sports, dance, or play games in which you were very active? | |||
| None | 37 (30,9%) | 36 (23,1%) | |
| 1 time last week | 58 (38,2%) | 50 (32,1%) | 0,088* |
| 2 or 3 times last week | 28 (18,4%) | 43 (27,6%) | |
| 4 times last week | 7 (4,6%) | 15 (9,6%) | |
| 5 times last week | 12 (7,9%) | 12 (7,7%) | |
| Missing (5) | |||
| Which one of the following describes you best for the last 7 days? | |||
| All or most of my free time was spent doing things that involve little physical effort | 24 (15,6%) | 19 (12,4%) | |
| I sometimes (1-2 times last week) did physical things in my free time. | 54 (35,1%) | 67 (43,8%) | 0,510* |
| I often (3-4 times last week) did physical things in my free time | 52 (33,8%) | 42 (27,5%) | |
| I quite often (5-6 times last week) did physical things in my free time | 17 (11%) | 16 (10,5%) | |
| I very often (7 or more times last week) did physical things in my free time | 7 (4,5%) | 9 (5,9%) | |
| Missing (6) | |||
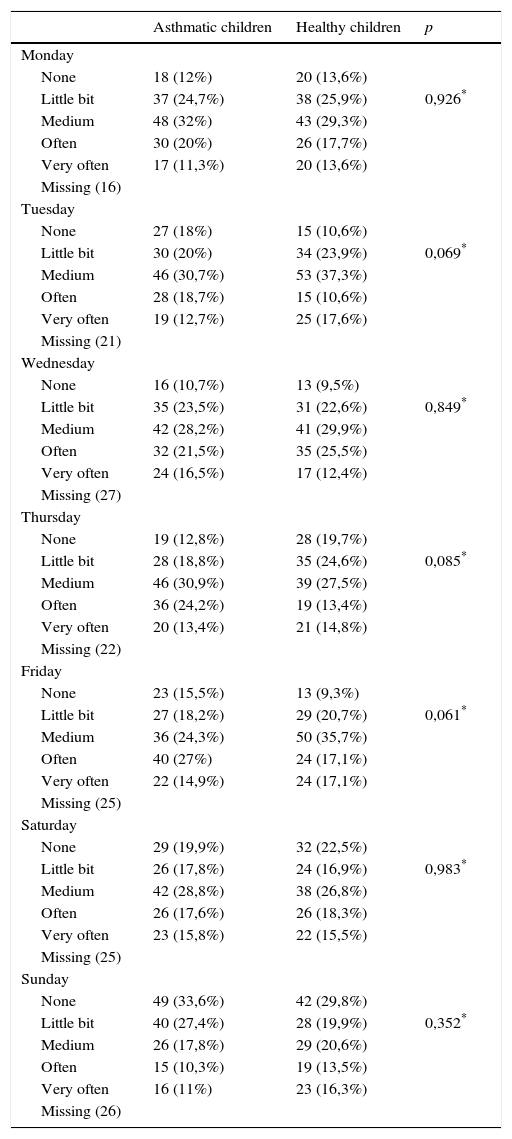
No significant differences were found regarding exercise distribution by days of the week (question 8; Table 3).
Exercise distribution during the day. It shows how often they did physical activity for each day of the week (question 8).
| Asthmatic children | Healthy children | p | |
|---|---|---|---|
| Monday | |||
| None | 18 (12%) | 20 (13,6%) | |
| Little bit | 37 (24,7%) | 38 (25,9%) | 0,926* |
| Medium | 48 (32%) | 43 (29,3%) | |
| Often | 30 (20%) | 26 (17,7%) | |
| Very often | 17 (11,3%) | 20 (13,6%) | |
| Missing (16) | |||
| Tuesday | |||
| None | 27 (18%) | 15 (10,6%) | |
| Little bit | 30 (20%) | 34 (23,9%) | 0,069* |
| Medium | 46 (30,7%) | 53 (37,3%) | |
| Often | 28 (18,7%) | 15 (10,6%) | |
| Very often | 19 (12,7%) | 25 (17,6%) | |
| Missing (21) | |||
| Wednesday | |||
| None | 16 (10,7%) | 13 (9,5%) | |
| Little bit | 35 (23,5%) | 31 (22,6%) | 0,849* |
| Medium | 42 (28,2%) | 41 (29,9%) | |
| Often | 32 (21,5%) | 35 (25,5%) | |
| Very often | 24 (16,5%) | 17 (12,4%) | |
| Missing (27) | |||
| Thursday | |||
| None | 19 (12,8%) | 28 (19,7%) | |
| Little bit | 28 (18,8%) | 35 (24,6%) | 0,085* |
| Medium | 46 (30,9%) | 39 (27,5%) | |
| Often | 36 (24,2%) | 19 (13,4%) | |
| Very often | 20 (13,4%) | 21 (14,8%) | |
| Missing (22) | |||
| Friday | |||
| None | 23 (15,5%) | 13 (9,3%) | |
| Little bit | 27 (18,2%) | 29 (20,7%) | 0,061* |
| Medium | 36 (24,3%) | 50 (35,7%) | |
| Often | 40 (27%) | 24 (17,1%) | |
| Very often | 22 (14,9%) | 24 (17,1%) | |
| Missing (25) | |||
| Saturday | |||
| None | 29 (19,9%) | 32 (22,5%) | |
| Little bit | 26 (17,8%) | 24 (16,9%) | 0,983* |
| Medium | 42 (28,8%) | 38 (26,8%) | |
| Often | 26 (17,6%) | 26 (18,3%) | |
| Very often | 23 (15,8%) | 22 (15,5%) | |
| Missing (25) | |||
| Sunday | |||
| None | 49 (33,6%) | 42 (29,8%) | |
| Little bit | 40 (27,4%) | 28 (19,9%) | 0,352* |
| Medium | 26 (17,8%) | 29 (20,6%) | |
| Often | 15 (10,3%) | 19 (13,5%) | |
| Very often | 16 (11%) | 23 (16,3%) | |
| Missing (26) | |||
Asthmatic patients had an average final score of 2,40 (±0,7; 0,85–4,62) and healthy controls had a mean score of 2,48 (±0,62; 1,09–4,42). There were no differences in the overall level of physical activity, estimated by PAQ score, between asthma and healthy children (2,40 (±0,7) vs. 2,48 (±0,62); p=0,32).
DiscussionFor this particular sample, PAQ was a practical method of collecting activity data, mainly because it is based on the child's self-report of activities in the previous 7 days. Evidence was provided that supported PAQ as a reliable and valid measure of general physical activity levels in children during the school year.9 As a 7-day report, PAQ has shown to correlate better with objective measures of activity in children whose memories are often questionable.10
A limitation of this questionnaire is the fact that it was designed for the Canadian population, and so it includes some sports which are not common in Portugal, such as rugby or American football. This may have influenced the results to some extent. However, the most popular Portuguese sports (such as football, athletics or swimming) are included in this questionnaire.
Children were attending routine appointments rather than emergency visits and those who had had an exacerbation in the previous six months were excluded. Furthermore, all children who answered “yes” to question 9 (“Have you been ill or has anything prevented you from taking your normal exercise?”) were also excluded.
Despite the fact that the majority of parents of asthmatic children considered that their child's disease was a barrier to physical activity,11 our results suggest that well controlled asthmatic patients can achieve a similar level of exercise performance to that of healthy children. The literature tends to be in agreement with our outcome, with some reports saying that asthmatic children are as physically fit and as physically active as healthy children.2,5,12,13 However, a number of studies have found that asthmatic children and adolescents are significantly less likely to engage in vigorous physical activity and are less physically fit than healthy individuals.7,14–19 Our interpretation is that our study includes only those situations of controlled asthma, while some of the mentioned references also cover patients with uncontrolled asthma. We emphasize that, despite the fact that the overall level of physical activity was the same in asthmatic and non-asthmatic children, playing sports outside school and taking part in team sports was less common among asthmatics.
The level of physical conditioning was found to be the main determinant of exercise tolerance for children with controlled asthma.5 Although children with well controlled asthma can achieve a level of physical performance similar to that of healthy children, the fear of inducing dyspnea inhibits many of them from taking part in physical activity and a low level of regular physical activity in turn leads to a low level of physical fitness.1 The consensus in the literature suggests that both parents and children with asthma are concerned about the effects of exercise and perceive asthma as a barrier to sports participation.7 Reduced participation may be influenced by organizational policies, family illness beliefs, health care advice and inaccurate symptom perception. Schools and families are often reluctant to encourage children to take part in physical education or normal play activity as a result of ignorance or misunderstanding of medical advice.11 Many young people themselves appear to accept sub-optimal control of symptoms and frequently misinterpret healthy shortness of breath when exercising with the symptoms of an impending asthma attack.2,20
In our study, both groups showed a low overall physical activity level (average 2.4), when compared to other populations. For example, in an American study with almost 500 adolescents, the mean activity score for boys and girls combined was 3.2110 and another study estimated a mean activity score of 3.29 for boys and of 3.16 for girls.21 This has to do with cultural issues; without doubt there is less access to sport in Portugal than in many other countries.
In relation to the various types of physical activity (Table 1), we believe that the differences found can be explained by the small take up in either group. In our population, besides the low physical performance score presented, only a few children in either group played sports outside school. Lack of participation in physical activity by children and adolescents is not surprising given that physical activity levels are known to be falling among young people in most industrialized nations. These rates fall even further as children reach adolescence, particularly in teenage girls.20
ConclusionWe found no difference between the level of physical activity of children and adolescents with controlled asthma and their healthy peers. In both groups the physical performance level was low. We highlight the need to promote exercise within pediatric asthma care, in order to protect both mental and physical health. The families of asthmatic patients should be informed about the benefits of physical exercise in well-controlled asthma.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Work previously presented as a poster in the Congress of the European Academy of Allergy and Clinical Immunology (EAACI 2012), Geneva, Switzerland, 16-20 June 2012.


