


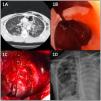
We present the clinical case of a 24-year-old patient diagnosed by computed tomography (CT) of an injury to the left bronchial tree following evidence at this level of reduction in caliber and loss of mural definition (Fig. 1A) after suffering a blunt chest trauma.
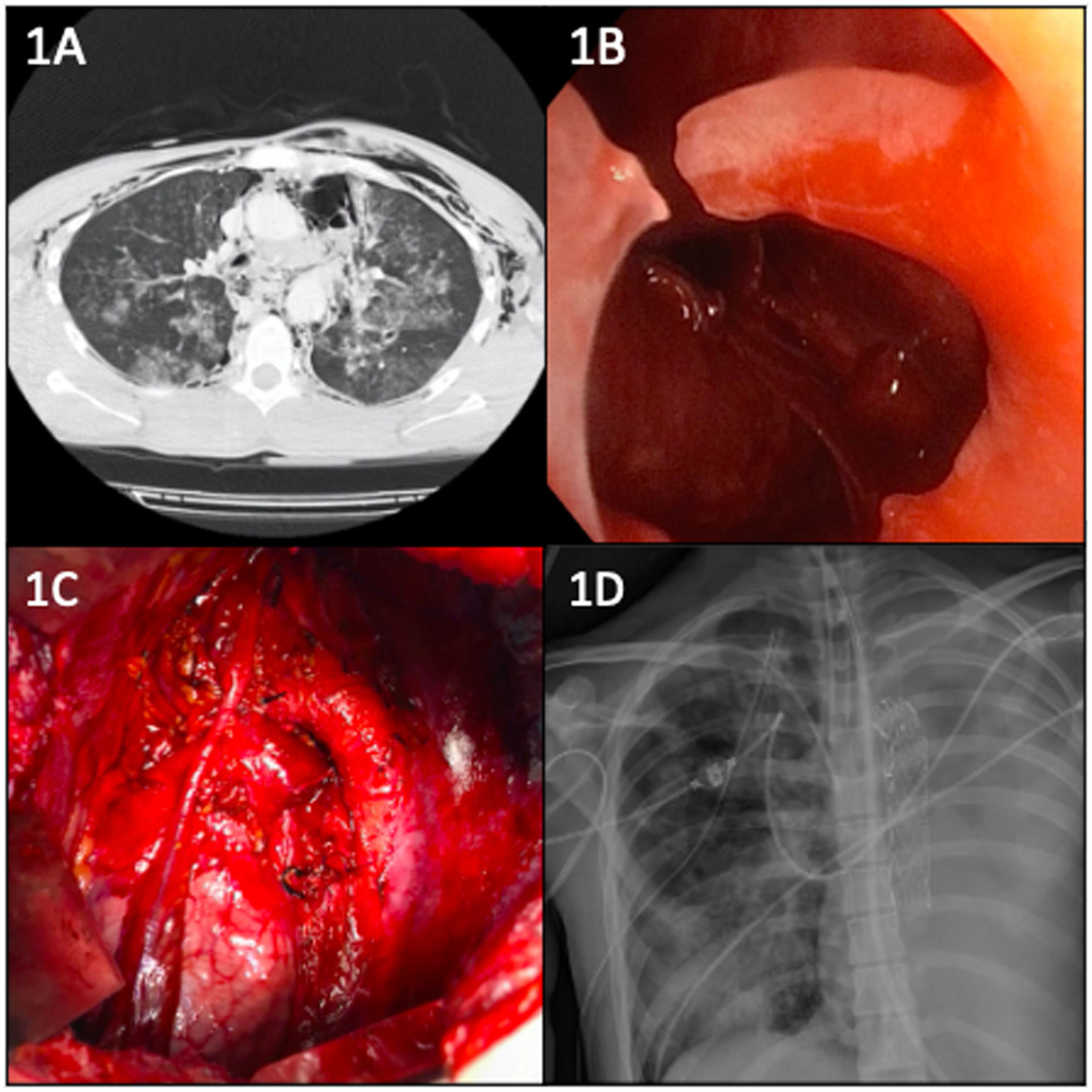
(A) Chest CT image: Subcutaneous emphysema. Pneumomediastinum. Diffuse bilateral pulmonary contusion. Reduction in caliber and loss of mural definition of the left main bronchus. (B) Endoscopic image: Complete amputation of the LMB with visualization of the left pleural cavity through it. (C) Intraoperative image: Extrapericardial left pneumonectomy after ligation of the ductus arteriosus and preservation of the phrenic nerve. (D) Postoperative chest X-ray. Valiant-type prosthesis is observed in the thoracic aorta distal to the left subclavian artery.
A diagnostic bronchoscopy was performed which confirmed loss of substance and complete amputation of the left main bronchus (Fig. 1B). At the same time, selective contralateral intubation guided by bronchoscopy was performed. The patient underwent emergency surgery by left anterolateral thoracotomy, revealing complete bronchial destruction, which made anastomosis impossible. Extrapericardial left pneumonectomy was performed (Fig. 1C). The patient underwent a complicated postoperative stage leading to a control CT scan which revealed pseudoaneurysm of the thoracic aorta; this was surgically excluded by endovascular placement of a prothesis (Fig. 1D). The patient presented slow improvement in respiratory function parameters, allowing discharge 64 days after hospital admission. After 2 years of follow-up, the patient has not presented any postoperative complications or hospital readmission.
The clinical picture of a patient with a bronchial rupture may initially be nonspecific, but there should be a high index of diagnostic suspicion in the presence of respiratory failure, subcutaneous emphysema, pneumomediastinum, pneumothorax with persistent air leak and/or failed lung reexpansion despite placement of a pleural drain.1
Once the condition is recognized, selective intubation, guided by fiberoptic bronchoscopy, of the bronchial tree contralateral to the lesion is recommended. Surgery should be immediate if the initial measures do not resolve a life-threatening condition. Surgical treatment of bronchial rupture is the early reestablishment of the anatomical continuity of the tracheobronchial tree by means of surgical repair of the lesion when possible,2 reserving pneumonectomy for those cases in which the bronchial tree cannot be reconstructed, as in the case described.
In conclusion, bronchial ruptures are infrequent entities with high mortality that occur mainly in polytraumatized patients, frequently associated with other serious concomitant injuries that can appear both initially and later.3


