

While adult chronic cough has high burden, its phenotypes, particularly those without aetiologically related underlying conditions, are understudied. We investigated the prevalence, lung function and comorbidities of adult chronic cough phenotypes.
MethodsData from 3608 participants aged 53 years from the Tasmanian Longitudinal Health Study (TAHS) were included. Chronic cough was defined as cough on most days for >3 months in a year. Chronic cough was classified into “explained cough” if there were any one of four major cough-associated conditions (asthma, COPD, gastroesophageal reflux disease or rhinosinusitis) or “unexplained cough” if none were present. Adjusted regression analyses investigated associations between these chronic cough phenotypes, lung function and non-respiratory comorbidities at 53 years.
ResultsThe prevalence of chronic cough was 10% (95%CI 9.1,11.0%) with 46.4% being “unexplained”. Participants with unexplained chronic cough had lower FEV1/FVC (coefficient: -1.2% [95%CI:-2,3, -0.1]) and increased odds of comorbidities including obesity (OR=1.6 [95%CI: 1.2, 2.3]), depression (OR=1.4 [95%CI: 1.0, 2.1]), hypertension (OR=1.7 [95%CI: 1.2, 2.4]) and angina, heart attack or myocardial infarction to a lesser extent, compared to those without chronic cough. Participants with explained chronic cough also had lower lung function than both those with unexplained chronic cough and those without chronic cough.
ConclusionsChronic cough is prevalent in middle-age and a high proportion is unexplained. Unexplained cough contributes to poor lung function and increased comorbidities. Given unexplained chronic cough is not a symptom of major underlying respiratory conditions it should be targeted for better understanding in both clinical settings and research.
Chronic cough is associated with adverse physical and psychosocial effects.1 In adults, cough is typically classified as acute (<3 weeks), subacute (3–8 weeks), or chronic (duration of >8 consecutive weeks).2 However, a duration of ≥ 3 consecutive months has been utilised as the definition for chronic cough in 55 studies included in a systematic review by Song et al., 2016.3 Global prevalence estimates for adult chronic cough, defined as cough ≥ 3 consecutive months at least for one year, range from 9% to 33%.2,4-6 A meta-analysis of over 70 studies estimated the mean global prevalence of chronic cough to be 9.6% and noted that Oceania had the highest regional prevalence (18.1%), followed by Europe (12.7%) and America (11.0%).7 Given the adult chronic cough prevalence is continuing to increase, this has become a significant public health issue.8
Chronic cough can be “explained” as a symptom of common conditions such as chronic rhinosinusitis, chronic obstructive pulmonary disease (COPD), asthma and gastro-oesophageal reflux disease (GERD). Less common causes of chronic cough include bronchiectasis, tuberculosis and pulmonary fibrosis.2,4 In American clinics, Irwin et al. estimated that chronic rhinosinusitis (20–80%), asthma (30–40%), COPD (11%) and GERD (10–60%) together account for up to 85% of those with chronic cough.2 In fact, these four major conditions are widely assessed as part of the clinical management of chronic cough.3,8 Chronic cough that is not a symptom of any of these recognised underlying conditions is often referred as “unexplained” chronic cough and is now receiving increasing interest. It is possible that smokers make up a proportion of individuals with unexplained chronic cough.4,7 However, some authors have suggested that ‘unexplained cough’ is regarded as distinct clinical entity, separate from smoking.6,9
While the heterogeneity of chronic cough is recognised, there are limited studies estimating the prevalence and clinical characteristics of various phenotypes/variants of cough.3 In particular, focused population-based research into “unexplained” chronic cough remains a major unmet need.5,9 Moreover, to our knowledge, no studies to date have investigated clinical or lung function parameters in chronic cough, especially in those of the unexplained variant in the general population (as opposed to a clinic setting). Research into possible associated comorbidities of chronic cough phenotypes is limited. Thus, it remains unclear whether and to what extent adults with unexplained or explained chronic cough suffer from poorer lung function and general health/comorbidities, who thus may benefit from specific clinical follow up and management.
Given the above knowledge gaps, we aimed to investigate the prevalence, and any associated lung function deficits and comorbidities of chronic cough phenotypes (both explained and unexplained cough) in a population-based sample of middle-aged Australians.
MethodsStudy design and populationWe used data from the Tasmanian Longitudinal Health Study (TAHS), collected from participants at both 7 and 53 years of age. The study has been reported in detail elsewhere.10 In brief, the TAHS commenced in 1968 involving a cohort of 8583 children born in 1961 and attending schools in Tasmania. The parents of the participants completed a questionnaire on the respiratory health of their children. The children underwent medical examinations and lung function testing. Since then, several follow-up studies have been conducted. In the most recent 6th decade follow-up in 2012, surviving participants from the original cohort with contact details (n = 6128, 71%) were invited to participate in a further clinical study. Between 2012 and 2016 (mean age of 53 years), 3608 participated in the study. These participants formed the sample for this analysis.
The study was approved by the Human Ethics Review Committees of all relevant institutions. Written informed consent was obtained from all participants.
Data collectionAt 53 years, all participants (3608) completed a questionnaire and of these, 2689 performed lung function tests (75%). Pre and post bronchodilator (BD) spirometry was performed according to the joint American Thoracic Society and European Respiratory Society guidelines, using an EasyOne ultrasonic spirometer (ndd Medizintechnik AG, Zürich, Switzerland).11 Participants were asked not to smoke for 4–6 h prior to testing. At least three manoeuvres per participant were attempted to obtain three acceptable blows and the best was recorded. Gas transfer for CO (TLCO) was also measured according to ATS/ERS guidelines.12 Multi-ethnic predicted spirometry values were derived from reference equations published by the Global Lung Initiative.13,14
Definitions of variablesChronic cough was defined as cough most days for ≥ 3 consecutive months in the past year. Those with chronic cough were then divided into those with (explained) or without (unexplained) one or more of the four major cough-associated conditions (asthma, COPD, GERD or rhinosinusitis).
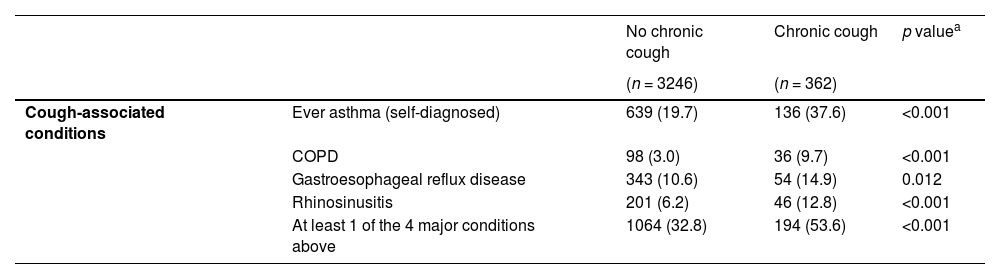
Ever asthma was defined by the question “have you ever had asthma”. COPD was defined based on spirometry as post-BD FEV1/FVC less than the lower limit of normal and/or self-reported doctor's diagnosis of COPD. The diagnoses of GERD and rhinosinusitis were based on responses to the question "Has a doctor ever told you that you have/had any of the following conditions?”.
Smoking was defined as current, past or never. Current or past smokers answered yes to the question “in your lifetime, have you smoked at least 100 cigarettes or equal amounts of cigars, pipes, or any other tobacco product?”. Current smokers additionally answered yes to the question “do you currently smoke [within the last four weeks].” Never smoking was defined by an answer of no to these questions.
Selected childhood characteristics (childhood cough, parental smoking and pneumonia/pleurisy) were taken from the 1968 baseline survey when participants were seven years of age.
Non-respiratory comorbidities were defined using elicited and spontaneous self-reports of doctor-diagnosed conditions by/at 53 years. These specifically included: angina, hypertension, obstructive sleep apnoea, depression and anxiety. These comorbidities were chosen after a careful review of the literature on cough-associated conditions. Obesity was also considered a non-respiratory comorbidity and defined as BMI>30 kg/m2.
Statistical analysesDescriptive characteristics of chronic cough and non-cough groups were reported. For categorical data, chi-squared tests were used to compare between groups. Mean values with standard deviation (SD) were reported for continuous data and two-tailed t-tests were used for comparison between groups. Multiple linear and logistic regression models were used to assess associations between chronic cough and lung function and comorbidities. The analyses were stratified by the presence/absence of the four major conditions known to explain chronic cough i.e. chronic rhinosinusitis, asthma, COPD and GERD. Two chronic cough groups, i.e. explained and unexplained, were also compared. Diagnostics of the model fits for the linear models were assessed. We identified potential confounders based on a review of the literature. A Directed Acyclic Graph (DAG) was then used to assist in the selection of a minimum set of confounders. The final confounders adjusted for in the regression models were childhood asthma, childhood cough, childhood pneumonia/pleurisy, parental smoking and personal smoking. The DAG was drawn in Dagitty, an online tool.15 All analyses were performed using STATA 15.1 (Stata Corp LP, College Station, TX, USA).
ResultsThis analysis included 3608 participants with mean age of 52.7 ± 0.8 years. Male participants comprised just under half (49.7%) of the sample. The prevalence of chronic cough was 10.0% (95%CI 9.1–11.0). Among those with chronic cough, 53.6% were “explained”.
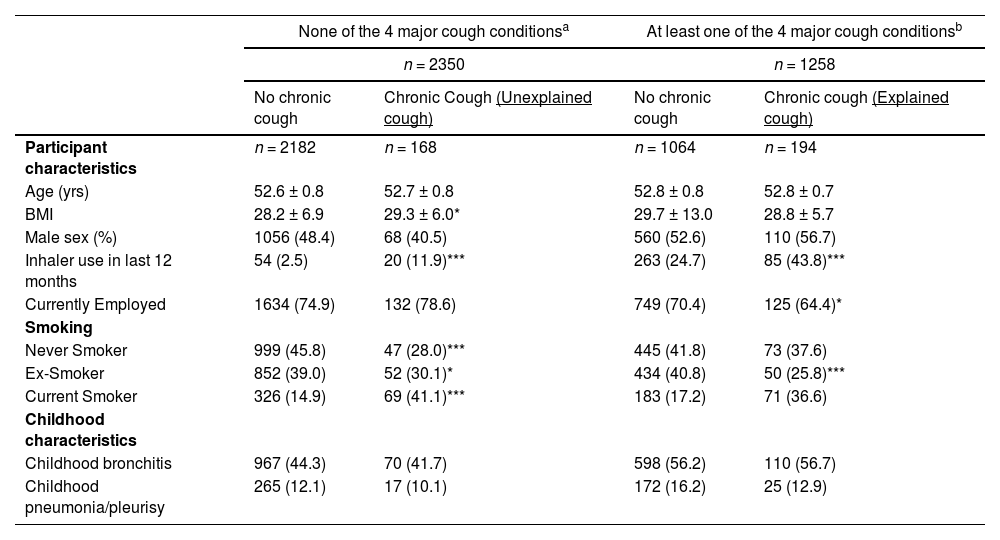
Tables 1, 2 and S1 show the demographic and, adult and childhood clinical characteristics of the participants by cough status. The prevalence of current smoking was 38.7% among those with chronic cough compared to 15.8% among those without chronic cough. The prevalence of the selected four major cough-associated conditions, namely, asthma, COPD, GERD and rhinosinusitis were significantly higher in those with chronic cough than those without chronic cough (Table 1). Those with unexplained chronic cough had higher BMI and higher prevalence of current smoking than those without chronic cough, but there were no significant differences in childhood characteristics including childhood cough, parental smoking and pneumonia/pleurisy (Table 2). Childhood bronchitis was more prevalent among those with explained cough than those with unexplained cough.
Relevant adult and childhood characteristics of chronic cough.
Relevant adult and childhood characteristics of chronic cough.
| None of the 4 major cough conditionsa | At least one of the 4 major cough conditionsb | |||
|---|---|---|---|---|
| n = 2350 | n = 1258 | |||
| No chronic cough | Chronic Cough (Unexplained cough) | No chronic cough | Chronic cough (Explained cough) | |
| Participant characteristics | n = 2182 | n = 168 | n = 1064 | n = 194 |
| Age (yrs) | 52.6 ± 0.8 | 52.7 ± 0.8 | 52.8 ± 0.8 | 52.8 ± 0.7 |
| BMI | 28.2 ± 6.9 | 29.3 ± 6.0* | 29.7 ± 13.0 | 28.8 ± 5.7 |
| Male sex (%) | 1056 (48.4) | 68 (40.5) | 560 (52.6) | 110 (56.7) |
| Inhaler use in last 12 months | 54 (2.5) | 20 (11.9)*** | 263 (24.7) | 85 (43.8)*** |
| Currently Employed | 1634 (74.9) | 132 (78.6) | 749 (70.4) | 125 (64.4)* |
| Smoking | ||||
| Never Smoker | 999 (45.8) | 47 (28.0)*** | 445 (41.8) | 73 (37.6) |
| Ex-Smoker | 852 (39.0) | 52 (30.1)* | 434 (40.8) | 50 (25.8)*** |
| Current Smoker | 326 (14.9) | 69 (41.1)*** | 183 (17.2) | 71 (36.6) |
| Childhood characteristics | ||||
| Childhood bronchitis | 967 (44.3) | 70 (41.7) | 598 (56.2) | 110 (56.7) |
| Childhood pneumonia/pleurisy | 265 (12.1) | 17 (10.1) | 172 (16.2) | 25 (12.9) |
Data presented as n (%).
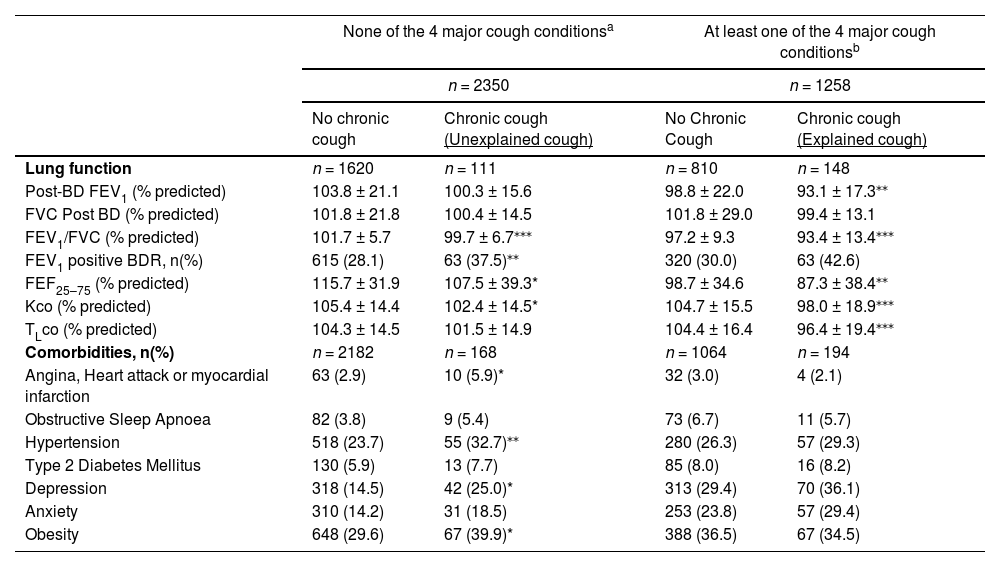
Post-BD lung function at 53 years according to explained and unexplained chronic cough are presented in Table 3. Those reporting unexplained chronic cough had significantly lower post-BD FEV1/FVC, FEF25–75, Kco and a higher proportion with a positive bronchodilator response in terms of significant FEV1 improvement than those without chronic cough and four major cough-associated conditions (asthma, COPD, GERD and rhinosinusitis). Those reporting explained chronic cough also had lower post-BD FEV1, FEV1/FVC, FEF25–75, Kco and TLco than those without chronic cough. When comparing two chronic cough groups, explained cough had lower post-BD FEV1, FVC, FEV1/FVC, EF25–75, Kco and TLco than unexplained cough.
Lung function and comorbidities at 53 years according to cough status stratified by the presence of four major cough-associated conditions.
| None of the 4 major cough conditionsa | At least one of the 4 major cough conditionsb | |||
|---|---|---|---|---|
| n = 2350 | n = 1258 | |||
| No chronic cough | Chronic cough (Unexplained cough) | No Chronic Cough | Chronic cough (Explained cough) | |
| Lung function | n = 1620 | n = 111 | n = 810 | n = 148 |
| Post-BD FEV1 (% predicted) | 103.8 ± 21.1 | 100.3 ± 15.6 | 98.8 ± 22.0 | 93.1 ± 17.3⁎⁎ |
| FVC Post BD (% predicted) | 101.8 ± 21.8 | 100.4 ± 14.5 | 101.8 ± 29.0 | 99.4 ± 13.1 |
| FEV1/FVC (% predicted) | 101.7 ± 5.7 | 99.7 ± 6.7⁎⁎⁎ | 97.2 ± 9.3 | 93.4 ± 13.4⁎⁎⁎ |
| FEV1 positive BDR, n(%) | 615 (28.1) | 63 (37.5)⁎⁎ | 320 (30.0) | 63 (42.6) |
| FEF25–75 (% predicted) | 115.7 ± 31.9 | 107.5 ± 39.3* | 98.7 ± 34.6 | 87.3 ± 38.4⁎⁎ |
| Kco (% predicted) | 105.4 ± 14.4 | 102.4 ± 14.5* | 104.7 ± 15.5 | 98.0 ± 18.9⁎⁎⁎ |
| TLco (% predicted) | 104.3 ± 14.5 | 101.5 ± 14.9 | 104.4 ± 16.4 | 96.4 ± 19.4⁎⁎⁎ |
| Comorbidities, n(%) | n = 2182 | n = 168 | n = 1064 | n = 194 |
| Angina, Heart attack or myocardial infarction | 63 (2.9) | 10 (5.9)* | 32 (3.0) | 4 (2.1) |
| Obstructive Sleep Apnoea | 82 (3.8) | 9 (5.4) | 73 (6.7) | 11 (5.7) |
| Hypertension | 518 (23.7) | 55 (32.7)⁎⁎ | 280 (26.3) | 57 (29.3) |
| Type 2 Diabetes Mellitus | 130 (5.9) | 13 (7.7) | 85 (8.0) | 16 (8.2) |
| Depression | 318 (14.5) | 42 (25.0)* | 313 (29.4) | 70 (36.1) |
| Anxiety | 310 (14.2) | 31 (18.5) | 253 (23.8) | 57 (29.4) |
| Obesity | 648 (29.6) | 67 (39.9)* | 388 (36.5) | 67 (34.5) |
Data are presented as mean ± SD or n(%) among those with and without one of the following cough-associated conditions: asthma, COPD, GERD or rhinosinusitis.
Among those without cough-associated conditions, those with chronic cough (unexplained cough) were compared with those without chronic cough.
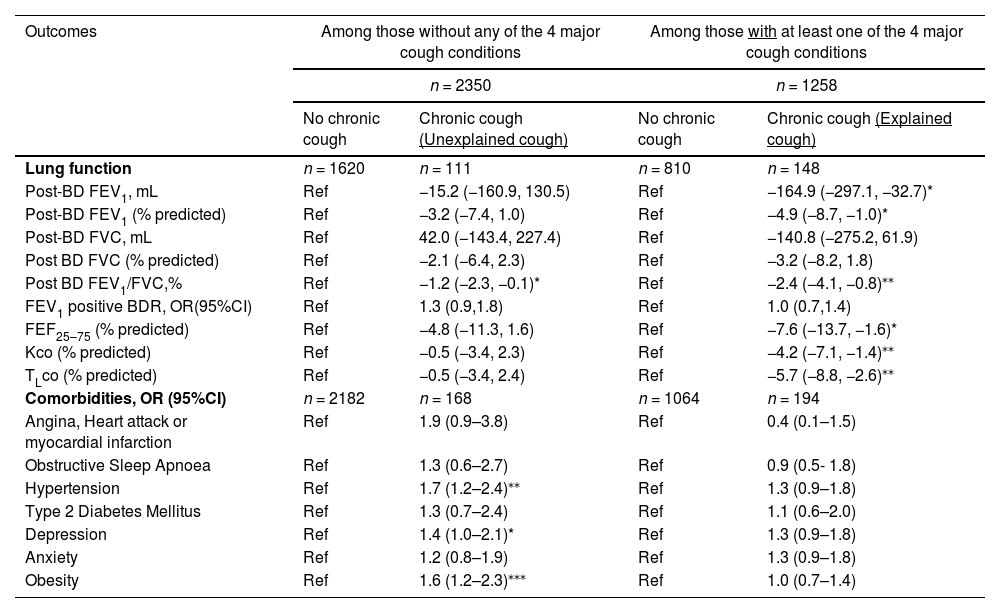
Adjusted associations between chronic cough and post-BD lung function stratified by the presence/absence of the four major cough-associated conditions (asthma, COPD, GERD and rhinosinusitis) are presented in Table 4. Unexplained chronic cough was significantly associated with reduced post-BD FEV1/FVC compared to those without cough and the four major cough-associated conditions. Explained chronic cough was associated with reduced post-BD FEV1, FEV1/FVC, FEF25–75, TLco and Kco compared to no chronic cough (Table 4). When comparing two cough groups, explained cough was associated with lower FEV1, FVC, FEV1/FVC, FEF25–75, TLco and Kco than unexplained cough (Table 5).
Adjusted associations between cough status and lung function and comorbidity.
| Outcomes | Among those without any of the 4 major cough conditions | Among those with at least one of the 4 major cough conditions | ||
|---|---|---|---|---|
| n = 2350 | n = 1258 | |||
| No chronic cough | Chronic cough (Unexplained cough) | No chronic cough | Chronic cough (Explained cough) | |
| Lung function | n = 1620 | n = 111 | n = 810 | n = 148 |
| Post-BD FEV1, mL | Ref | −15.2 (−160.9, 130.5) | Ref | −164.9 (−297.1, −32.7)* |
| Post-BD FEV1 (% predicted) | Ref | −3.2 (−7.4, 1.0) | Ref | −4.9 (−8.7, −1.0)* |
| Post-BD FVC, mL | Ref | 42.0 (−143.4, 227.4) | Ref | −140.8 (−275.2, 61.9) |
| Post BD FVC (% predicted) | Ref | −2.1 (−6.4, 2.3) | Ref | −3.2 (−8.2, 1.8) |
| Post BD FEV1/FVC,% | Ref | −1.2 (−2.3, −0.1)* | Ref | −2.4 (−4.1, −0.8)⁎⁎ |
| FEV1 positive BDR, OR(95%CI) | Ref | 1.3 (0.9,1.8) | Ref | 1.0 (0.7,1.4) |
| FEF25–75 (% predicted) | Ref | −4.8 (−11.3, 1.6) | Ref | −7.6 (−13.7, −1.6)* |
| Kco (% predicted) | Ref | −0.5 (−3.4, 2.3) | Ref | −4.2 (−7.1, −1.4)⁎⁎ |
| TLco (% predicted) | Ref | −0.5 (−3.4, 2.4) | Ref | −5.7 (−8.8, −2.6)⁎⁎ |
| Comorbidities, OR (95%CI) | n = 2182 | n = 168 | n = 1064 | n = 194 |
| Angina, Heart attack or myocardial infarction | Ref | 1.9 (0.9–3.8) | Ref | 0.4 (0.1–1.5) |
| Obstructive Sleep Apnoea | Ref | 1.3 (0.6–2.7) | Ref | 0.9 (0.5- 1.8) |
| Hypertension | Ref | 1.7 (1.2–2.4)⁎⁎ | Ref | 1.3 (0.9–1.8) |
| Type 2 Diabetes Mellitus | Ref | 1.3 (0.7–2.4) | Ref | 1.1 (0.6–2.0) |
| Depression | Ref | 1.4 (1.0–2.1)* | Ref | 1.3 (0.9–1.8) |
| Anxiety | Ref | 1.2 (0.8–1.9) | Ref | 1.3 (0.9–1.8) |
| Obesity | Ref | 1.6 (1.2–2.3)⁎⁎⁎ | Ref | 1.0 (0.7–1.4) |
Data are presented as mean difference (95%CI) or OR (95%CI) adjusted for childhood asthma, childhood bronchitis, childhood pneumonia/pleurisy, parental smoking and personal smoking.
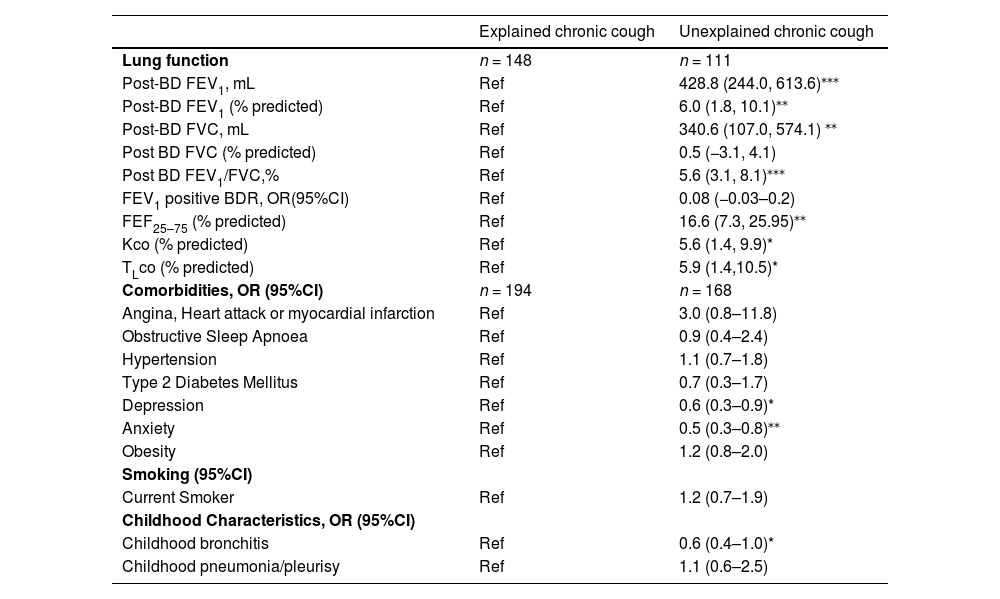
Adjusted association between cough status and lung function and comorbidity between explained and unexplained cough groups.
| Explained chronic cough | Unexplained chronic cough | |
|---|---|---|
| Lung function | n = 148 | n = 111 |
| Post-BD FEV1, mL | Ref | 428.8 (244.0, 613.6)⁎⁎⁎ |
| Post-BD FEV1 (% predicted) | Ref | 6.0 (1.8, 10.1)⁎⁎ |
| Post-BD FVC, mL | Ref | 340.6 (107.0, 574.1) ⁎⁎ |
| Post BD FVC (% predicted) | Ref | 0.5 (−3.1, 4.1) |
| Post BD FEV1/FVC,% | Ref | 5.6 (3.1, 8.1)⁎⁎⁎ |
| FEV1 positive BDR, OR(95%CI) | Ref | 0.08 (−0.03–0.2) |
| FEF25–75 (% predicted) | Ref | 16.6 (7.3, 25.95)⁎⁎ |
| Kco (% predicted) | Ref | 5.6 (1.4, 9.9)* |
| TLco (% predicted) | Ref | 5.9 (1.4,10.5)* |
| Comorbidities, OR (95%CI) | n = 194 | n = 168 |
| Angina, Heart attack or myocardial infarction | Ref | 3.0 (0.8–11.8) |
| Obstructive Sleep Apnoea | Ref | 0.9 (0.4–2.4) |
| Hypertension | Ref | 1.1 (0.7–1.8) |
| Type 2 Diabetes Mellitus | Ref | 0.7 (0.3–1.7) |
| Depression | Ref | 0.6 (0.3–0.9)* |
| Anxiety | Ref | 0.5 (0.3–0.8)⁎⁎ |
| Obesity | Ref | 1.2 (0.8–2.0) |
| Smoking (95%CI) | ||
| Current Smoker | Ref | 1.2 (0.7–1.9) |
| Childhood Characteristics, OR (95%CI) | ||
| Childhood bronchitis | Ref | 0.6 (0.4–1.0)* |
| Childhood pneumonia/pleurisy | Ref | 1.1 (0.6–2.5) |
Data are presented as mean difference (95%CI) or OR (95%CI) adjusted for childhood asthma, childhood bronchitis, childhood pneumonia/pleurisy, parental smoking and personal smoking where applicable.
Those with unexplained cough had significantly higher prevalence of angina, hypertension, depression and obesity compared to those without cough (Table 3). Prevalences of obstructive sleep apnoea, anxiety and type 2 diabetes mellitus were not significantly different between those with unexplained cough and those without chronic cough.
Adjusted associations between cough and non-respiratory comorbidities from multiple regression analyses showed increased odds of obesity, depression, hypertension and angina, heart attack or myocardial infarction to a lesser extent in those with unexplained cough compared to those without chronic cough (Table 4). There was no evidence of associations between explained cough and the non-respiratory comorbidities (Table 4). When comparing two cough groups, unexplained cough was associated with lower odds of depression and anxiety (Table 5).
DiscussionTo the best of our knowledge, this is the first population-based study investigating chronic “explained” cough associated with the more common specific aetiologies and “unexplained” cough in the context of prevalence, lung function and comorbidities. Chronic cough was present in 10% of our middle-aged population and surprisingly 46.4% of those had “unexplained chronic cough”.
Notably, compared to no chronic cough, unexplained chronic cough was also associated with worse FEV1/FVC ratio and greater risk of comorbidities including obesity, depression and hypertension, independent of personal smoking. These findings indicate that unexplained chronic cough represents a clinically important group for management and there is a clear need to explore and understand this unexplained cough group further. Our results also suggest that individuals with unexplained cough, particularly with a smoking history may already have underlying lung function deficits despite not being diagnosed with COPD according to spirometric definitions. These individuals may fall into the relatively newly termed “pre-COPD” group and thus warrant close follow up and preventative care.16 They may also have undiagnosed bronchiectasis as diagnosis requires awareness in primary care and which overlaps with COPD. This highlights the unmet clinical needs in this area, for general practitioners, respiratory physicians and allergists.17 As preventing decline in lung function has been regarded as important in reducing future morbidity18, this further supports the clinical importance of deeply evaluating patients with unexplained chronic cough given some lung function parameters were reduced in this clinically distinct group.
There were significant associations with certain atypical non-respiratory comorbidities in the unexplained chronic cough group including hypertension and obesity. The reported increased prevalence of hypertension in those with unexplained cough may have been due to ACE-inhibitor use, which in the literature has been implicated in 2–33% of dry cough.19 However, whether this was the cause in the current study population is unknown, although unlikely to be great, as this medication question was not specifically asked in the survey although medications in general were. The higher proportion of obesity in those with unexplained cough may be explained by a number of possibilities, as previously discussed in the literature, such as hypertension, which is more common in obese patients.20,21 There are also speculative mechanisms by which obesity as a syndrome is thought to affects the airways, such as the mechanical effect on airway diameter causing reduced lung volumes or increased obesity-related pro-inflammatory adipokines affecting bronchial hyperresponsiveness in non-asthmatics.22
We found that explained chronic cough was associated with marked global reduction in lung function indices including post-BD FEV1, FEV1/FVC, FEF25–75, Kco and TLco. These data are unsurprising and consistent with previous studies. For example, Koo et al. found that in a cohort of COPD patients, those with chronic cough showed both lower FEV1 and diffusing capacity (transfer factor) than the others in the cohort.23 Our findings highlight that among those with asthma or COPD, having chronic cough may be an indicator of more severe disease and significantly reduced lung function.
Interestingly, there was significantly increased psychiatric comorbidity among those with explained chronic cough compared to those with unexplained chronic cough. This suggests that unexplained cough was not due to the psychiatric condition itself, but coincidentally to a co-morbid respiratory condition. Previous studies have documented the negative impact of chronic cough as a symptom on quality of life.17,23 Some studies have found that chronic cough as a symptom is more significantly associated with depression than diagnosis of asthma or allergic diseases.24 Despite this, in the current study there was no significant association between depression and those with explained chronic cough and those with no chronic cough. This may be due to the smaller sample size in the explained cough analysis, limiting the power to assess this association.
Some participants reported inhaled medication use, but did not report having asthma or COPD per se (two of the 4 conditions used to define “explained” cough) (Table 2). In this study, inhaled medication was defined by the question “Have you used any inhaled medicines to help your breathing in the last 12 months?”. It is possible that some people might have used inhaled medication for intercurrent acute respiratory illnesses although they had no chronic symptoms and/or diagnosed asthma/COPD. Inhaled medication for cough itself is sometimes prescribed by doctors (without a firm diagnosis) or potentially borrowed from family members and/or been purchased without a prescription (“over the counter” in Australia). On the other hand, due to self-reporting issues, we cannot rule out the possibility that some of these people did indeed have asthma or COPD.
This study has major strengths in that the Tasmanian Longitudinal Health Study from its inception has been a prospectively followed whole-of-population birth cohort, allowing us to estimate the prevalence of chronic cough in now middle-aged participants representing the general community with substantial information across the lifespan to date. Secondly, the availability of standardized lung function data for large numbers of participants allowed for analysis of functional changes in both explained and unexplained chronic cough which is unprecedented in the literature.
There are also some limitations in our study. Firstly, misclassification of self-reporting of diagnosis/symptoms may have led to some inaccuracy in prevalence estimates for both cough and/or co-morbidities. This is reflected in individuals who were on inhaled medication despite not reporting any respiratory symptoms/diseases. However, this was likely to be non-differential and so may in fact have underestimated our findings. Secondly, the cross-sectional associations identified in our study did not allow any conclusions about causation or temporality which limited the analysis of correlates in the chronic cough population. Thirdly, as the members of the cohort were not individually evaluated by a respiratory specialist, there is a lack of data on other disease aetiologies associated with chronic cough (e.g. bronchiectasis) and we do not have data on specific medication use (i.e. ACE inhibitors), which may overestimate the prevalence estimates of unexplained chronic cough. There were no specific data on neuroactive treatments. Finally, we do not have any detailed symptom data which may indicate cough hypersensitivity syndrome, a clinically useful paradigm in which cough is usually triggered by low levels of thermal, mechanical or chemical exposure and may be the relevant clinical feature of either explained or unexplained cough.25
ConclusionsChronic cough is prevalent in middle aged adults and a large proportion of them do not have established cough-associated conditions. There is a need to fully characterise disease correlates in those with chronic cough, particularly “unexplained chronic cough”, as they evidently suffer from increased comorbidities and worse lung function. There is also a need to better implement strategies to optimize treatment and management of adult chronic cough and to tease out likely causative factors.
Authors’ contributionsStudy concept and design: SS, SCD, DSB, JLP. Acquisition of data: SCD, EHW, MJA, GB, CL, PT, BB, GSH. Analysis and interpretation of data: SS, DSB, SCD, JLP, EHW, ABC, AL Drafting of the manuscript: SS, SCD, DSB, JLP, EHW, CL, GB, ABC, AL. Critical revision of the manuscript for important intellectual content: SS, DSB, SCD, JLP, EHW, ABC, AL, CL, GB, PT, GSH, MJA, BB. Statistical analysis: SS, SCD, DSB, JLP, EHW, ABC. Obtained funding: SCD, EHW, MJA, PT, CL, BB, GSH.
We acknowledge the TAHS study participants and previous investigators. We thank Professor Mark Jenkins, PhD, Centre for Epidemiology & Biostatistics, The University of Melbourne, Victoria, a TAHS investigator, but not a co-author of this manuscript, for his assistance with obtaining funds and data collection. We also acknowledge all the respiratory scientists who collected data in the lung function laboratories of Tasmania, Victoria, Queensland and New South Wales; the research interviewers, data entry operators and research officers. Finally, we thank the Archives Office of Tasmania for providing data from the 1968 TAHS questionnaires.
This study was supported by the National Health and Medical Research Council (NHMRC) of Australia under NHMRC project grant scheme (299901, 1021275) and NHMRC European collaborative grant scheme (1101313) as part of ALEC (Ageing Lungs in European Cohorts funded by the European Union's Horizon 2020 research and innovation programme under grant agreement No 633212); The University of Melbourne; Clifford Craig Medical Research Trust of Tasmania; the Victorian, Queensland & Tasmanian Asthma Foundations; The Royal Hobart Hospital; Helen MacPherson Smith Trust; and GlaxoSmithKline. The funding agencies had no direct role in the conduct of the study, the collection, management, statistical analysis and interpretation of the data, preparation or approval of the manuscript.


