



The carbonic anhydrase inhibitor acetazolamide stimulates ventilation through metabolic acidosis mediated by renal bicarbonate excretion. In animal models, acetazolamide attenuates acute hypoxia-induced pulmonary hypertension (PH), but its efficacy in treating patients with PH due to pulmonary vascular disease (PVD) is unknown.
Methods28 PVD patients (15 pulmonary arterial hypertension, 13 distal chronic thromboembolic PH), 13 women, mean±SD age 61.6±15.0 years stable on PVD medications, were randomised in a double-blind crossover protocol to 5 weeks acetazolamide (250mg b.i.d) or placebo separated by a ≥2 week washout period. Primary endpoint was the change in 6-minute walk distance (6MWD) at 5 weeks. Additional endpoints included safety, tolerability, WHO functional class, quality of life, arterial blood gases, and hemodynamics (by echocardiography).
ResultsAcetazolamide had no effect on 6MWD compared to placebo (treatment effect: mean change [95%CI] -18 [-40 to 4]m, p=0.102) but increased arterial blood oxygenation through hyperventilation induced by metabolic acidosis. Other measures including pulmonary hemodynamics were unchanged. No severe adverse effects occurred, side effects that occurred significantly more frequently with acetazolamide vs. placebo were change in taste (22/0%), paraesthesia (37/4%) and mild dyspnea (26/4%).
ConclusionsIn patients with PVD, acetazolamide did not change 6MWD compared to placebo despite improved blood oxygenation. Some patients reported a tolerable increase in dyspnoea during acetazolamide treatment, related to hyperventilation, induced by the mild drug-induced metabolic acidosis. Our findings do not support the use of acetazolamide to improve exercise in patients with PVD at this dosing.
ClinicalTrials.gov IdentifierNCT02755298
Therapeutic advances in treating patients with chronic pulmonary vascular disease (PVD) have markedly improved survival, exercise performance and quality of life (QoL).1-4 Two major forms of PVD are pulmonary arterial and chronic thromboembolic pulmonary hypertension (PAH and CTEPH), which are characterized by a chronically elevated pulmonary artery pressure (PAP) and pulmonary vascular resistance (PVR) due to reduction and/or remodelling of the pulmonary vascular bed.5 Pulmonary endarterectomy and/or balloon-angioplasty may substantially improve hemodynamics and functional impairment in CTEPH, but many patients with distal PVD in CTEPH have persisting PH resembling PAH.3 Despite remarkable improvements with PVD-targeted drug combination therapy, PVD is still incurable and associated with chronically impaired functional capacity and limited daily activity.6 Therefore, new therapeutic strategies that potentially act on different pathways are greatly needed.7
Acetazolamide, a carbonic anhydrase (CA) inhibitor, stimulates ventilation by inducing a metabolic acidosis mediated by renal bicarbonate excretion. Acetazolamide also reduced proximal tubular sodium reabsorption and thus serves as an adjunct to commonly prescribed loop diuretics in patients with right or left heart failure.8,9 A recent study has shown that that additive acetazolamide is effective to increase the number of successful decongestion in patients with decompensated heart failure.10 Another potentially beneficial effect of acetazolamide is a reduction in hypoxic pulmonary vasoconstriction independent of CA inhibition 11-13 which is possibly related to a reduction in hypoxia-mediated reactive oxygen species generation in pulmonary vascular smooth muscle.14 According to these various effects, Acetazolamide is used as diuretic, to improve blood oxygenation in selected patients with sleep related breathing disorders, to prevent acute mountain sickness in a hypobaric hypoxic environment and for the treatment of increased intraocular or intracerebral pressure.15-18 We have previously shown that acetazolamide given for one week to patients with PVD improved nocturnal arterial oxygen saturation (SpO2) and sleep disordered breathing.19 Acetazolamide reduced PAP in patients with chronic obstructive pulmonary disease (COPD) travelling to 3,100 m and reduced the incidence of altitude-related adverse health effects.20 In patients with PVD, intravenous injection of acetazolamide acutely lowered the rise in PVR induced by normobaric hypoxia vs. placebo but did not affect resting hemodynamics.21 In animal models of PH, beneficial effects of acetazolamide on pulmonary hemodynamics and remodelling have been demonstrated.22,23
Knowing the beneficial effect of acetazolamide on nocturnal blood oxygenation and the observed benefits on PH animal models, the objective of the current trial was to investigate whether oral acetazolamide over the course of 5 weeks improves functional and hemodynamic outcomes in patients with stable PVD.
MethodsStudy subjectsPatients with PVD classified as PAH (WHO group 1) or distal CTEPH (WHO group 4) diagnosed according to current guidelines,24 aged 20 - 80 years, of both sexes were recruited from outpatients receiving care in the PH-Clinic, University Hospital Zurich. Study participants had to be in stable condition and on PVD-targeted therapy for > 4 weeks. Patients with CTEPH had distal disease not suitable for endarterectomy or persistent PH after pulmonary endarterectomy. Pregnant women and patients with left heart disease or more than mild obstructive or restrictive pulmonary disease, severe daytime hypercapnia (PaCO2 ≥ 6.5 kPa), liver disease, non-correctable electrolyte disturbances or severe chronic renal failure (GFR < 30 ml/min) and known allergy to acetazolamide and other carbonic anhydrase inhibitors, methazolamide, dichlorphenamide, thiazide diuretics, and sulfonamides were excluded. All patients gave written informed consent. The study complied with the declaration of Helsinki and was approved by the local ethical authorities (KEK-ZH-2016-00089-2) and registered at clinicaltrial.gov (NCT02755298).
Study design and sample sizeThis randomized, placebo-controlled, double-blind, cross-over trial assessed the effect of oral acetazolamide in stable, optimally treated patients with PVD on 6-minute walk distance (6MWD) and other outcome measures after 5 weeks of treatment. Patients received acetazolamide, 250 mg twice daily, and identical looking placebo capsules for 5 weeks each in random order with a wash-out period of at least two weeks between the study arms.
We assumed a minimal important difference (± SD) in the primary outcome 6MWD of 35 ± 50 m [9]. To achieve a power of 80%, α = 0.05, a minimum of 20 participants were required. Accounting for possible dropouts, the goal was to include 24 participants.
Participants were randomised to a treatment sequence in balanced blocks of four using a computer- generated list. The study staff and participants were unaware of the administered treatment (double-blinded design). Unblinding was performed only after completion of data analysis.
All the performed assessments are described in detail in the supplement.
OutcomesThe main outcome of this study was the change in 6MWD. Secondary outcomes included arterial blood gas analysis, hemodynamics by echocardiography, measures of QoL, cognitive performance and short-term safety and tolerability of acetazolamide in terms of side effects.
Statistical analysisThe data are summarized as mean and standard deviation. The primary outcome was analysed in the intention-to-treat (ITT) population and by per-protocol analysis using a mixed multivariate regression model adjusting for randomization and period effect and is reported as mean differences and 95% confidence interval (CI). Model assumptions were tested by visual inspection of the homogeneity and normality of the residuals and the random effects. Missing values for the main outcome were replaced by baseline values thus assuming no treatment effect (ITT). All statistical analyses were performed using R (version 2022.02.1). Statistical significance was assumed when 95% confidence intervals of mean differences did not overlap zero and with a p-value < 0.05.
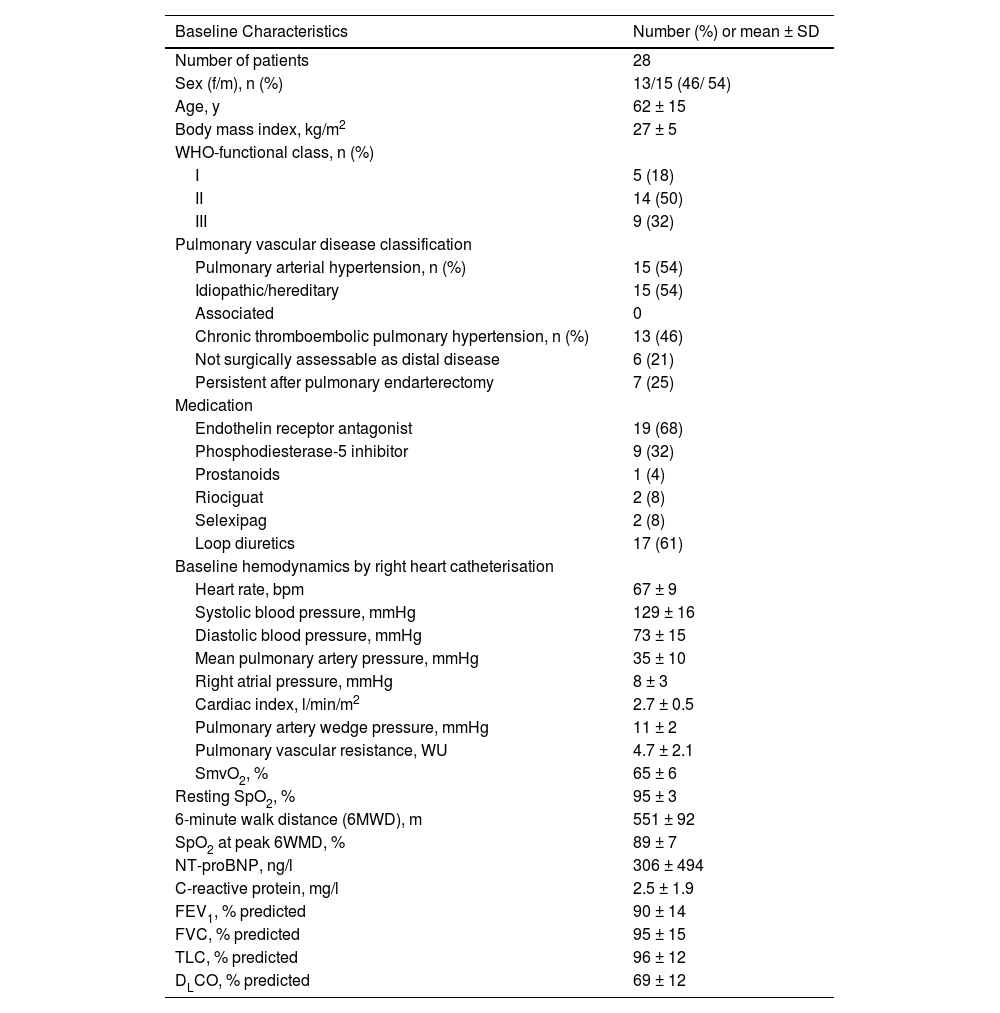
ResultsWe screened 52 patients for eligibility between 2017 to 2020. Twenty-eight patients with a mean ± SD, age 62 ± 15 years, 13 females, 15 PAH, 13 distal CTEPH (Fig. 1, Table 1) were randomized. All patients were on stable PH-medication and had a baseline 6MWD of 551 ± 92 m. Twenty-five patients completed the study. Three patients withdrew from the study, two in the acetazolamide phase due to side effects and one in the placebo phase as feeling no effects.

Baseline characteristics.
SmVO2: mixed venous oxygen saturation, SpO2: oxygen saturation by pulse oximetry, FEV1: forced expiratory volume in one second, FVC: forced vital capacity, TLC: total lung capacity, DLCO: diffusion lung capacity for carbon monoxide.
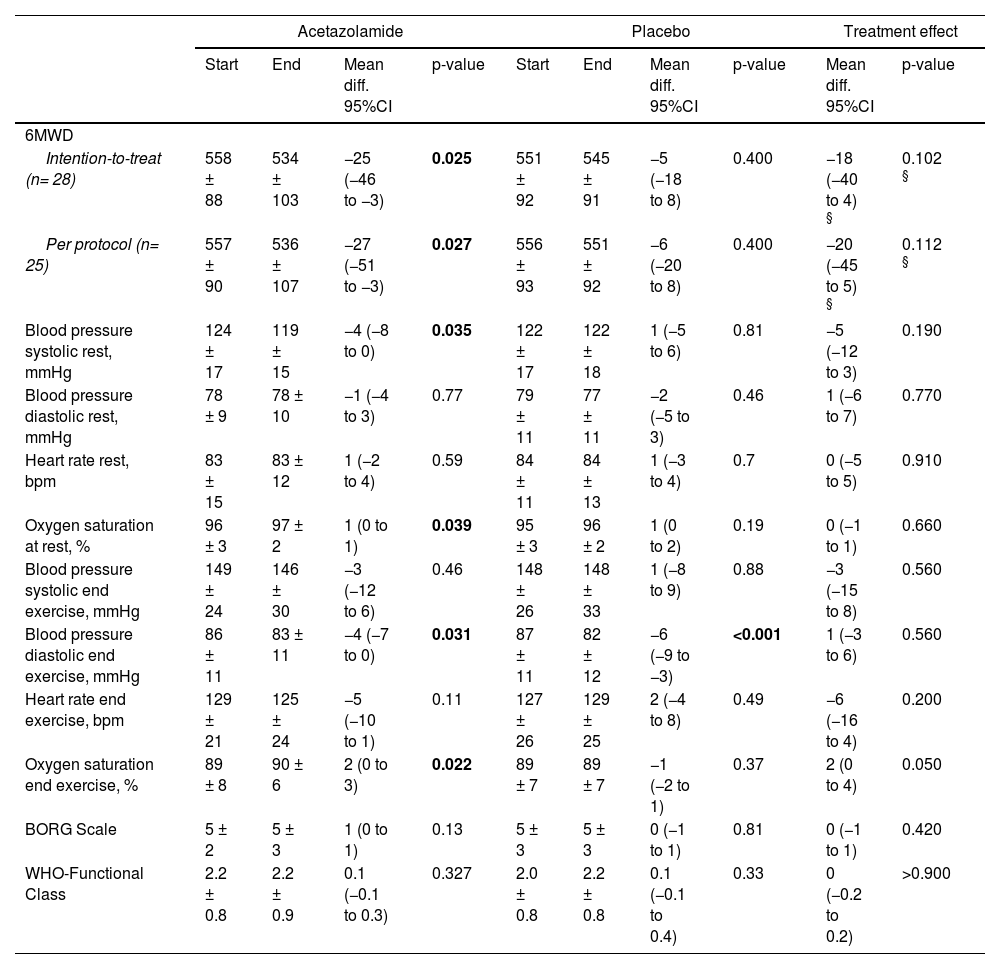
In the intention-to-treat analysis, the 6MWD was slightly, albeit significantly, reduced in the acetazolamide phase (mean difference (95% CI) -25 (-46 to -3) m, p = 0.025) whereas no change was found in the placebo phase (-5 (-18 to 8) m, p = 0.400). This resulted in an overall, non-significant treatment effect of -18 (- 40 to 4) m p = 0.102) (Table 2, Fig. 2). The oxygen saturation before and after 6MWT was higher at the end of the acetazolamide phase compared to the placebo phase (Table 2).
Main outcome: Change in 6-minute walk distance (6MWD) with different treatments.
| Acetazolamide | Placebo | Treatment effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Start | End | Mean diff. 95%CI | p-value | Start | End | Mean diff. 95%CI | p-value | Mean diff. 95%CI | p-value | |
| 6MWD | ||||||||||
| Intention-to-treat (n= 28) | 558 ± 88 | 534 ± 103 | −25 (−46 to −3) | 0.025 | 551 ± 92 | 545 ± 91 | −5 (−18 to 8) | 0.400 | −18 (−40 to 4) § | 0.102 § |
| Per protocol (n= 25) | 557 ± 90 | 536 ± 107 | −27 (−51 to −3) | 0.027 | 556 ± 93 | 551 ± 92 | −6 (−20 to 8) | 0.400 | −20 (−45 to 5) § | 0.112 § |
| Blood pressure systolic rest, mmHg | 124 ± 17 | 119 ± 15 | −4 (−8 to 0) | 0.035 | 122 ± 17 | 122 ± 18 | 1 (−5 to 6) | 0.81 | −5 (−12 to 3) | 0.190 |
| Blood pressure diastolic rest, mmHg | 78 ± 9 | 78 ± 10 | −1 (−4 to 3) | 0.77 | 79 ± 11 | 77 ± 11 | −2 (−5 to 3) | 0.46 | 1 (−6 to 7) | 0.770 |
| Heart rate rest, bpm | 83 ± 15 | 83 ± 12 | 1 (−2 to 4) | 0.59 | 84 ± 11 | 84 ± 13 | 1 (−3 to 4) | 0.7 | 0 (−5 to 5) | 0.910 |
| Oxygen saturation at rest, % | 96 ± 3 | 97 ± 2 | 1 (0 to 1) | 0.039 | 95 ± 3 | 96 ± 2 | 1 (0 to 2) | 0.19 | 0 (−1 to 1) | 0.660 |
| Blood pressure systolic end exercise, mmHg | 149 ± 24 | 146 ± 30 | −3 (−12 to 6) | 0.46 | 148 ± 26 | 148 ± 33 | 1 (−8 to 9) | 0.88 | −3 (−15 to 8) | 0.560 |
| Blood pressure diastolic end exercise, mmHg | 86 ± 11 | 83 ± 11 | −4 (−7 to 0) | 0.031 | 87 ± 11 | 82 ± 12 | −6 (−9 to −3) | <0.001 | 1 (−3 to 6) | 0.560 |
| Heart rate end exercise, bpm | 129 ± 21 | 125 ± 24 | −5 (−10 to 1) | 0.11 | 127 ± 26 | 129 ± 25 | 2 (−4 to 8) | 0.49 | −6 (−16 to 4) | 0.200 |
| Oxygen saturation end exercise, % | 89 ± 8 | 90 ± 6 | 2 (0 to 3) | 0.022 | 89 ± 7 | 89 ± 7 | −1 (−2 to 1) | 0.37 | 2 (0 to 4) | 0.050 |
| BORG Scale | 5 ± 2 | 5 ± 3 | 1 (0 to 1) | 0.13 | 5 ± 3 | 5 ± 3 | 0 (−1 to 1) | 0.81 | 0 (−1 to 1) | 0.420 |
| WHO-Functional Class | 2.2 ± 0.8 | 2.2 ± 0.9 | 0.1 (−0.1 to 0.3) | 0.327 | 2.0 ± 0.8 | 2.2 ± 0.8 | 0.1 (−0.1 to 0.4) | 0.33 | 0 (−0.2 to 0.2) | >0.900 |
Data are shown as mean ± Standard deviation or mean difference and 95% confidence interval.
. A) Boxplot of 6MWD before and at the end of acetazolamide and placebo treatment. B) Change in 6MWD with acetazolamide and placebo displayed as mean and 95% confidence interval and treatment effect (mean change and 95% confidence interval).")
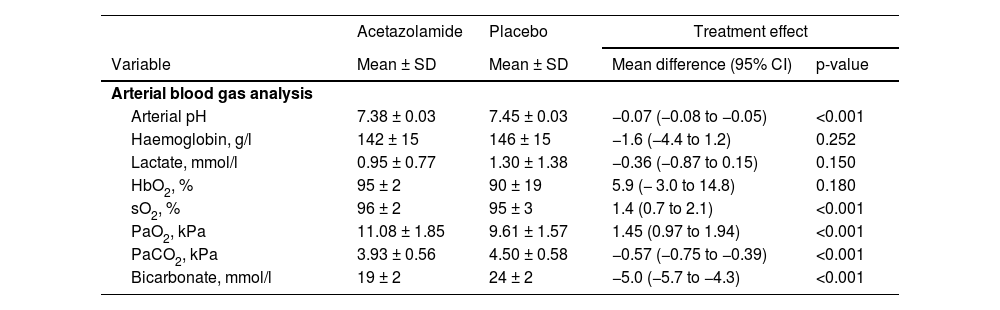
Arterial blood gas analysis showed a metabolic acidosis induced by acetazolamide (between group differences (95% CI): arterial pH -0.07 (-0.08 to -0.05), bicarbonate (-5.0 (-5.7 to 4.3) mmol/l, all p <0.001) and expected hyperventilation (PaCO2 -0.57 (-0.75 to -0.39) kPa, PaO2 1.45 (0.97 to 1.94) kPa), both p<0.001). (Table 3).
Blood gas analysis.
Data are shown as mean ± standard deviation and mean difference with 95% confidence interval.
Abbreviations: HbO2: oxyhaemoglobin, sO2: oxygen saturation, PaO2: arterial partial pressure of oxygen, PaCO2: arterial partial pressure of carbon dioxide.
WHO functional class (Table 2), quality of life (supplementary table 1) and cognitive function tests ((Figure of 5-Test and Trail making test) supplemental table 4) showed no differences between placebo and acetazolamide treatment. Furthermore, right and left ventricular parameters measured by echocardiography – most notably systolic PAP – did not differ at the end of either phases (supplementary table 3).
SafetyDrug specific side effects and adverse effects were documented after each treatment phase and patients reported mostly paraesthesia (37%), change of taste (22%), gastrointestinal distress (15%), headache (15%), and fatigue (15%). Twenty-six percent of the patients reported mild dyspnea during the acetazolamide phase see supplementary table 2. No serious adverse event occurred.
DiscussionThis is the first randomized, placebo-controlled clinical cross-over trial evaluating the effect of oral acetazolamide given for 5 weeks on exercise capacity and hemodynamic measures in patients with PVD. Acetazolamide did not improve 6MWD despite an improvement in blood oxygenation at rest and end-exercise due to hyperventilation induced by the drug-induced metabolic acidosis. There were no differences in QoL, echocardiographic parameters, cognitive function or WHO-functional class. During the acetazolamide treatment, known side effects, such as paraesthesia, and change of taste were significantly more reported. Interestingly, dyspnea perception increased despite improved blood oxygenation.
Acetazolamide is known to improve blood oxygenation in selected patients with sleep related breathing disorders and is used to prevent altitude-related illness in a hypobaric hypoxic environment.15-17 In accordance with these known effects of acetazolamide, we demonstrated improved arterial blood oxygenation by hyperventilation as reflected by the lower PaCO2 induced by metabolic acidosis due to renal bicarbonate excretion at the end of the acetazolamide treatment phase compared to the placebo phase. However, despite the increase in PaO2, approximately a quarter of the patients reported increased dyspnea, most probably caused by the increased ventilatory drive induced by the lower arterial pH. This is in accordance with studies in the healthy and in patients with chronic lung diseases at high altitude, which show an improved blood oxygenation with acetazolamide vs placebo, along with less altitude related adverse health effects.18 However, the effect of acetazolamide on exercise performance at altitude is less clear. Studies in healthy people reveal conflicting results, some showing no effects, others revealing a slightly reduced exercise capacity. Bradwell et al. assessed 20 healthy subjects in a randomized, placebo-controlled trial at 3,459 m and showed that more participants in the acetazolamide group were unable to finish a predefined submaximal exercise test after 16 to 27 hours of altitude exposure despite better oxygenation and furthermore described their perception of exercise as more difficult compared to the placebo group.25 In contrast to this study, Bradbury et al assessed 10 healthy subject in a cross-over design and again an improvement in oxygenation and reduction in acute mountain sickness was seen in the acetazolamide group but despite these differences, no change in time to complete a 2-mile self-paced treadmill time trial 2 and 24 h after exposure to hypobaric hypoxia (3500 m) was observed.26 When considering these studies, we need to take into account that Bradwell assessed men and women between 18–67 years of age and none of the participants < 30 y failed the exercise test independently of their treatment allocation 25 whereas Bradbury assessed 10 well trained young men (22 ± 3 years, VO2peak: 50.8 ± 6.5 ml·kg−1·min−1; body fat %: 20.6 ± 5.2%) 26 and thus it might not be possible to extrapolate the results in this second study to females, the untrained or older individuals at high altitude. Studies in patients with respiratory diseases, who may be at particular risk of increased dyspnea in case of drug-induced hyperventilation, are very scarce. Acetazolamide has repeatedly been shown to improve sleep-related breathing disorders at altitude among healthy and patients with obstructive sleep apnea or COPD, along with improved cerebral tissue oxygenation.27,28 In a non-hypoxic environment at low altitude, acetazolamide may be used to improve sleep-related breathing in patients with heart failure, whereas effects in patients with chronic respiratory failure are less clear.17,29-32 In patients with PVD, we have previously shown that acetazolamide given for one week improved nocturnal arterial oxygen saturation (SpO2) and sleep disordered breathing while the 6MWD distance on the following day was not altered in this short-term study.19 However, improved nocturnal oxygenation by oxygen therapy improved daytime performance in the same trial in PVD 19 and the improved blood oxygenation during exercise induced by supplemental oxygen significantly improved cycling performance in PVD.33 That is why we hypothesized, that improved oxygenation as induced by acetazolamide could improve exercise performance as measured by the 6MWD, a hypothesis that is not supported by the present data.
Long-term treatment with acetazolamide in hypoxia-induced PH animal models has led to a decrease in PAP.22,23 In accord with this study, we found that in patients with COPD travelling to 3,100 m, acetazolamide taken prophylactically before an altitude sojourn lowered the altitude-induced increase in PAP compared to placebo.20 In a randomized trial in patients with PVD, intravenous acetazolamide lowered the PVR-increase induced by normobaric hypoxia vs. placebo but did not affect resting hemodynamics measured with right heart catheter examination.21 These studies possibly indicate that only hypoxic patients might benefit from acetazolamide hemodynamic improvement.
The mechanisms of exercise limitation in patients with respiratory disease are complex – especially in PVD. Several mechanisms from central to circulatory, muscular limitation and impaired oxygen transport, capillarity and metabolism have been proposed.34 The increase in dyspnea reported by a quarter of the patients in this study can probably be explained by the acetazolamide induced stimulation of ventilation which might result in greater work of breathing during exercise and explain the reduction in exercise capacity. Concerning the increased dyspnea perception in response to an increased respiratory drive, different dosages of acetazolamide, e.g. only evening medication or lower dosages in the morning, might reduce side effects and might result in different findings.
Our study has several limitations. The sample size was relatively small. However, a cross-over design allows a smaller sample size for a given power, which is of importance in interventional trials in a rare disease such as PVD. Our patients were all stable on optimal PH-medical therapy and had a good baseline 6MWD of > 550 m, which may not be easily improved by further therapy due to the well-documented ceiling effect of 6MWD.35,36 Thus in classical PH-trials, patients with walk-distances >450m have been excluded. However, the 6MWD is an established clinically important end-point for clinical trials in PH 7 and as much as morbidity and mortality outcomes may be preferred, such endpoints are not realistic in a small investigator-initiated proof-of concept trial.
We assessed hemodynamics by echocardiography but are aware that assessment of pulmonary vascular resistance by right heart catheterisation would have been the preferred outcome for such a proof-of concept study. However, repetitive right heart catheterisations after a relatively short time in a cross-over trial is not feasible for most participants. There was no effect of acetazolamide on patient-reported outcomes, such as QoL. The rather short duration of 5 weeks and low dosing of acetazolamide might not have been sufficient to demonstrate changes, since other known therapies in PVD may take longer to reach maximal benefit, particularly if the intended effect is to achieve regression of pathologic remodelling and not immediate vasodilation. In an animal model of PVD, Christou et al. found changes in pulmonary hemodynamics and pulmonary vascular histology at 7 weeks in response to higher dosing of 100 mg/kg acetazolamide per day (compared to our dosing of ∼ 1-2 mg/kg per day).37 The study design did not allow us to evaluate the effect of acetazolamide on the effectiveness of PVD targeted drug therapies and a potential change in effectiveness of these medications. Thus, we cannot exclude the possibility that drug interactions or other mechanisms of acetazolamide, such as anti-inflammatory ones, may have influenced our results. Nor do we know whether inclusion of more severe PVD-patients would have altered the results.
In summary, we have shown that 5 weeks of 250 mg acetazolamide b.i.d. did not improve 6MWD despite improved blood oxygenation at rest and during exercise but was associated with a significant increase in dyspnea perception probably related to hyperventilation to compensate the metabolic acidosis induced by acetazolamide. Acetazolamide did not improve hemodynamics assessed by echocardiography, nor did it have any effect on other outcome measures such as QoL, WHO functional class, or cognitive function. The current study does not support the use of acetazolamide to improve exercise and daytime performance in patients with PVD at the doses and treatment duration used.
Author contributionsAll authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. All authors contributed to the production of the final manuscript with revision for important intellectual content. SU is the guarantor of the paper.
FundingThis study was funded by the Swiss National Science Foundation


