




Indoor air quality (IAQ) is considered an important determinant of human health. The association between exposure to volatile organic compounds, particulate matter, house dust mite, molds and bacteria in day care centers (DCC) is not completely clear. The aim of this project was to study these effects.
Methods – study designThis study comprised two phases. Phase I included an evaluation of 45 DCCs (25 from Lisbon and 20 from Oporto, targeting 5161 children). In this phase, building characteristics, indoor CO2 and air temperature/relative humidity, were assessed. A children's respiratory health questionnaire derived from the ISAAC (International Study on Asthma and Allergies in Children) was also distributed. Phase II encompassed two evaluations and included 20 DCCs selected from phase I after a cluster analysis (11 from Lisbon and 9 from Oporto, targeting 2287 children). In this phase, data on ventilation, IAQ, thermal comfort parameters, respiratory and allergic health, airway inflammation biomarkers, respiratory virus infection patterns and parental and child stress were collected.
ResultsIn Phase I, building characteristics, occupant behavior and ventilation surrogates were collected from all DCCs. The response rate of the questionnaire was 61.7% (3186 children).
Phase II included 1221 children. Association results between DCC characteristics, IAQ and health outcomes will be provided in order to support recommendations on IAQ and children's health. A building ventilation model will also be developed.
DiscussionThis paper outlines methods that might be implemented by other investigators conducting studies on the association between respiratory health and indoor air quality at DCC.
A qualidade do ar interior (IAQ) é considerada um determinante importante da saúde humana. A associação entre a exposição a compostos orgânicos voláteis, partículas, ácaros, bolores e bactérias em creches (DCC) não é perfeitamente clara. O objectivo deste estudo foi estudar esses efeitos.
Metodologia – desenho do estudoEste estudo decorreu em duas Fases. A Fase I incluiu uma avaliação de 45 DCCs (25 em Lisboa e 20 no Porto, visando 5.161 crianças). Nesta Fase, foram avaliadas as características dos edifícios, o CO2 e a temperatura ambiente/humidade relativa no interior. Também foi distribuído um questionário de saúde respiratória das crianças derivado do ISAAC (Estudo Internacional sobre a Asma e Alergias em Crianças). A Fase II englobou duas avaliações e incluiu 20 DCCs seleccionadas da fase I, após uma análise de clusters (11 em Lisboa e 9 no Porto, visando 2.287 crianças). Nesta Fase, foram recolhidos dados sobre a ventilação, IAQ (qualidade do ar interior), parâmetros de conforto térmico, saúde em termos respiratórios e alérgicos, marcadores biológicos de inflamação das vias respiratórias, padrões de infecção de vírus respiratórios e stress dos pais e crianças.
ResultadosNa Fase I, foram recolhidas as características dos edifícios, o comportamento dos ocupantes e os marcadores de ventilação, para todas as DCCs. A taxa de resposta ao questionário foi de 61,7% (3.186 crianças).
A Fase II incluiu 1.221 crianças. Os resultados da associação entre as características dos DCC, a IAQ e os resultados para a saúde serão fornecidos para apoiar as recomendações sobre a IAQ e a saúde das crianças. Um modelo de ventilação de edifícios também será desenvolvido.
DiscussãoEste documento destaca a metodologia que pode ser implementada por outros investigadores que realizam estudos sobre a associação entre a saúde respiratória e a qualidade do ar interior, em creches e infantários.
Since the first studies on indoor air quality (IAQ), some common indoor air pollutants such as carbon monoxide, particulate matter, volatile organic compounds (VOC) and formaldehyde have been related to acute and chronic respiratory diseases,1 contributing to indoor air pollution burden of disease estimated at 2.7%.2 In modern society, children spend most of their time indoors (up to 85%),3 at home or in children day care centers (DCC), and they are particularly vulnerable to the effects of IAQ.4
Different studies have shown that IAQ and ventilation are associated with respiratory symptoms, allergy and infections.5–7 Furthermore, it was estimated that about one million deaths per year in children under 5, could be attributed to acute respiratory infections due to IAQ.8
Scientific and political authorities have proposed limits to the levels of air pollutants through recommendations and legislation. In 2006, Portuguese legislation was passed (Decreto-Lei 89/2006) setting reference levels for some indoor pollutants.9
The design and construction of buildings have focused on mechanical resistance, durability and comfort. Economic concerns related to energy efficiency in buildings have resulted in a decrease in ventilation flow rates and practices that have led to a deterioration in IAQ. It has been suggested that these might have been partly responsible for the rise in respiratory diseases in recent decades.10–12
Despite the large number of publications about the effects of indoor air pollution in schools, there is not much evidence about the association between IAQ in DCCs and health. This was addressed in some European reviews that systematized what has been done and what research is still required.13–15
Studies focused on IAQ in DCCs are important because of their specificity and potential impact on children's health. Furthermore, as there are no clear thresholds that define the level of exposure to indoor air pollutants that affects children's health at DCCs, studies of those environments could provide additional relevant information. Day care centres studies may help identify feasible interventions that could subsequently be implemented by policy makers. It has been shown that some interventions might be effective in modulating IAQ in schools16–18 and influencing respiratory symptoms.19
Because IAQ patterns and effects vary widely between different countries,8 local and national studies are important where interventions on population health are being considered. Each population is uniquely linked to its genetic background, specificities of the available infrastructures or construction typology, cultural behavior and climatic factors. This point has been made by Canha et al.20 who showed that there was a connection between ventilation strategies and lower ventilation rates and higher CO2 levels in Portuguese elementary school classrooms, when compared with Finnish classrooms in a rural setting. Other Portuguese studies targeting schoolchildren and adolescents have reported associations between IAQ and respiratory symptoms and wheezing.21,22
Outdoor and indoor environments should be considered simultaneously when studying the IAQ effects on human health. Different cross-sectional23–25 and longitudinal26–28 studies have shown the effects of both indoor and outdoor air pollutants on children's respiratory health. Background pollutant concentrations measured at central monitoring stations, traffic density/distance to major roads29,30 or dispersion models25 have been used29,31 to study outdoor air pollutants. Exposure to indoor environments, such as schools32,33 or houses, where children spend a large amount of time, has only more recently been taken into consideration.34,35
Some Portuguese studies have also reported IAQ deficiencies both in Lisbon36,37 and Oporto.22 Pegas et al.37 reported that ventilation problems are present throughout the year and different pollutant profiles can be found in different seasons of the year.
When studying children's illnesses it might also be important to consider their effects on parents, as diseases could enhance both child and parental stress. There is clear evidence that stress induces cortisol release and this hormone exerts an inhibitory action over the immune system.38,39 On the other hand, research has shown that the mothers of children with respiratory diseases, such as asthma, have higher levels of parenting stress, compared to those with healthy children,40–42 and children whose parents experience higher levels of stress show higher vulnerability to respiratory disease.43–45 Therefore, the parent–child relationship could influence the child's hypothalamus–pituitary–adrenal cortex (HPA) axis activation and cortisol release.46 In fact, cortisol may be one of the biological links between parent–child stress and respiratory disease in childhood. For these reasons ENVIRH also included an ancillary study to assess parental symptoms (depression/anxiety), psychosocial context (parental stress, marital satisfaction, life events) and a measure of the child's HPA axis activation (24-h cortisol production).
In view of the lack of studies about IAQ in Portuguese DCCs and the public health concern about this topic, we decided to conduct the ENVIRH study (Environment and Health in Children Day Care Centres). The main goals of the ENVIRH study were: (1) to characterize the respiratory health of the children attending DCCs; (2) to describe building characteristics and performance, including ventilation in DCCs; (3) to study the IAQ in DCCs, choosing those pollutants that might be more relevant to children's respiratory diseases, according to the literature: particulate matter, volatile organic compounds, formaldehyde, carbon dioxide, fungi and bacteria; (4) to assess how parental psychological and relational dimensions, together with child cortisol release (stress biomarker), may change according to child respiratory disease; (5) to study the relationship between the previous factors; and finally (6) to suggest recommendations for the authorities, the scientific community and the general public. This paper discusses the rationale of the ENVIRH Study and describes the methodology used by our team to carry it out.
Materials and methodsOur study was focused on DCCs. These are institutions that provide childcare while parents are at work. Besides basic care, these centers offer children a wide range of activities for their entertainment, including some educational activities.
DCCs provide care for infants, toddlers and pre-school children (up to 5–6 years old). We chose to study DCCs from the two main Portuguese cities (Lisbon and Oporto) mainly for reasons of feasibility. These are busy cities with different air pollution sources which influence outdoor air quality. DCCs are located in different places: some are in apartments, others in isolated villas (with or without gardens, terraces or other forms of outdoor spaces), some in modern buildings and others in very old parts of town. In our country, children DCCs vary from fully State-run to joint or solely private ventures. We approached the Instituto da Segurança Social (the DCC national regulatory authority) in order to obtain a list of potential DCCs to be included in the study. For this study, only the private social security institutions (IPSS) included in the list were considered, for practical reasons, as they broadly provided all the age ranges that we aimed to study and their participation was expected to be easier. Those DCCs (IPSS) belonged either to Confederação Nacional de Instituições de Solidariedade or to União das Misericórdias Portuguesas, both of which supported our study.
The project was designed to be carried out in two different phases. During Phase I we collected data on building characteristics and some preliminary IAQ indicators, and used a small screening health questionnaire. In Phase II a new health questionnaire was distributed to the same children who attended the selected DCCs, and a more detailed assessment of IAQ, building characteristics and ventilation was carried out. The project flowchart can be found in Figure 1. Task description will be divided in the two phases.
Phase 1Between October and December 2010Sample size – school and children selection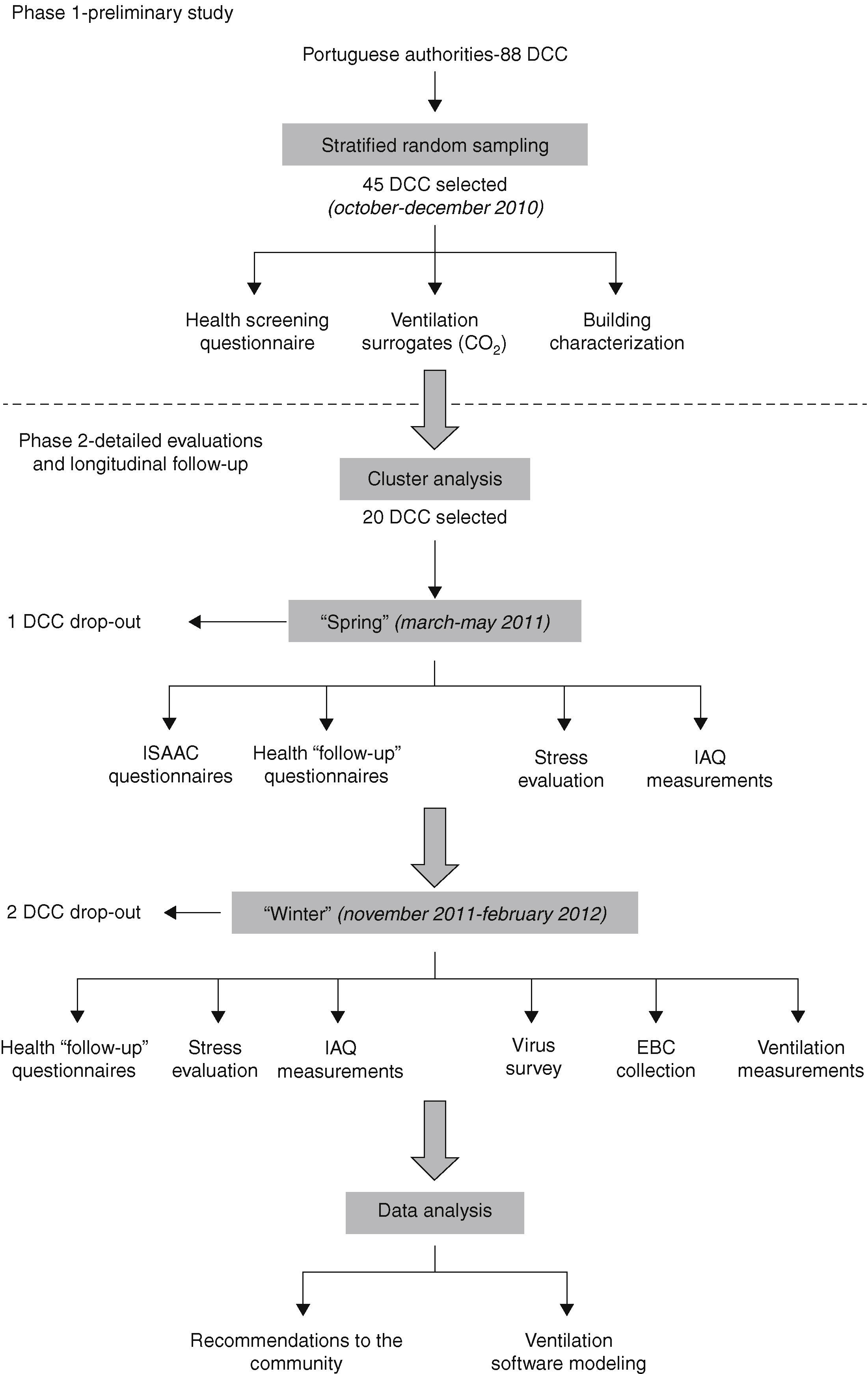
For technical reasons, we were only able to study in detail a limited number of DCCs. However, a sample size was calculated in order to guarantee a sufficient number of children to be able to estimate wheezing prevalence. Based on published data,47 a 25% prevalence of wheezing in the last twelve months was considered. For a confidence level of 95% and a 1.5% margin of error, assuming a 50% nonresponse rate and the median number of children per DCC from the list provided by the national authorities (median=105 children), we would need a sample size of 45 DCCs, equivalent to 4853 questionnaires.
Between October and December 2010, 45 out of 88 DCCs (48 in Lisbon and 40 in Oporto) were selected through proportional stratified random sampling, which took into consideration the proportionality in each stratum (district) between the number of recruited centers and the total number of centers. The 45 selected DCCs (25 in Lisbon and 20 in Porto) comprised 5161 children.
From the initial selection of 45 DCCs, 10 refused to participate (5 in each city) and were replaced following a random sampling, in order to achieve the intended number of centers and maintain the proportionality of districts.
Building characteristicsTechnicians visited all DCCs to collect data on building characteristics, according to a thorough standard checklist drafted for the study. Data collected were used in both phases. The recorded items included: type of building (single or multi-storey building), construction year (for some buildings older than 100 years an approximate age was considered), area (total and with heating or air conditioning), type of surroundings (urban, rural, mixed) and pollution sources identifiable by inspection, number of children (total and per room), building envelope (materials used to make walls, ceiling, windows and solar protections), ventilation type (whether mechanical, natural or hybrid, considering admission and exhaust sources in different compartments), building heating and air conditioning (strategies and fuel), water heating (device and location), cooking (strategy and fuel), past records and visual inspection for mold and dampness sites, occupant practices regarding climatization (heating and cooling) and ventilation during different seasons (summer, winter and spring/autumn), and user perceived quality of climatization comfort and air quality in different seasons.
Of note, only pollution sources that could be identified by inspection (e.g.: combustion appliances of types B and C according to European norms48) were recorded, because diffuse pollution sources, such as construction materials emissions, are not easily identifiable and it was not possible to introduce this information objectively into the survey. As we did not analyze chemicals such as ammonia, and did not plan to check all the chemical ingredients of all the cleaning products used in DCCs, no data were collected on these.
Building characteristics are expected to play a key role in the indoor air quality as some parameters (e.g. type of windows and type of window seals) affect the air permeability of the building envelope, which in turn could influence air pollutant levels.
Indoor air quality and ventilationIAQ analysis included measurements of CO2 levels (as CO2 is considered an IAQ surrogate marker), temperature and humidity in different compartments and at different hours of the day, after allowing for 10 to 15min stabilization of the reading in the equipment. For the measurement of outdoor and indoor air temperature and relative humidity, a digital thermo hygrometer, model Oregon Scientific THGR328N, was used. The estimated uncertainty is UT=±1.16°C. The concentration of CO2 was measured with a non-dispersive infrared absorption detector Telaire 7001. The estimated uncertainty is UCO2=±62ppm for a measurement of 1000ppm and UCO2=±175ppm for a measurement of 3000ppm. Measurements were taken during a period of day care center activity. Room occupancy during the measurement period was also registered.
An average of three rooms was monitored in each DCC so as to conduct the survey in a short period of time, under weather conditions as similar as possible. The sampled rooms were selected as for a worst case scenario, through empirical evaluation of the building, considering the spaces with a higher density occupancy, fewer windows and windows that were apparently less permeable to air.
Allergic and respiratory health evaluationRespiratory health status was assessed using a short health questionnaire derived from the ISAAC (International Study of Asthma and Allergies in Children) questionnaire.49 Questions concerned child and household characteristics such as age, sex, wheezing, rhinitis symptoms, atopic dermatitis, presence of siblings, parental medical history, cigarette smoke exposure and parental education. Questionnaires were handed out to parents by the DCC staff who collected them on completion.
Phase 2Phase II consisted of two visits: visit 1 – Spring (between March and May 2011) and visit 2 – Winter (between November 2011 and February 2012).
Sample size – school and children selectionIn Phase II, which began three months after Phase I, 20 DCCs were selected through a cluster analysis (which considered CO2 concentrations, temperature and humidity indoors, measured in Phase I) by a hierarchical model (Ward method). DCCs which were further apart in the dendrogram were chosen. During this phase, three DCCs dropped out of the study (one in Visit 1 and two in Visit 2).
All children (n=2287) in the selected DCCs were invited to participate and questionnaires were distributed as in Phase I.
Indoor air qualityThe IAQ pollutants studied were those included in Portuguese legislation,9 with the exception of radon and ozone. Radon was not measured due to financial constraints and because it was not mandatory for Lisbon. With regard to ozone, it was expected that indoor ozone concentrations would depend mostly on outdoor levels, as no potential indoor ozone sources were identified in DCCs.
The study was carried out under typical occupation conditions, during everyday activities and comprised the monitoring of chemical (carbon dioxide, carbon monoxide, formaldehyde, total volatile organic compounds and PM10) and biological (bacteria, fungi and house-dust mites) contaminants, as well as thermal comfort parameters. In all, 5–9 classrooms were evaluated in each DCC (from 3 months up to 5–6 years).
The methods chosen to evaluate chemical parameters were based on the Technical Note NT-SCE-02 document50 that establishes the proper methodologies to perform indoor air quality audits in buildings, in accordance with published legislation.9 The relevant references and requirements of this Technical Note can be consulted in Table 1. Reference methods were used for PM10 and total volatile organic compounds (TVOC), while equivalent methods were used for formaldehyde, carbon dioxide and carbon monoxide. Thermal comfort, and bacteria and fungi quantifications followed accredited methods that comply with ISO and EN standards. No standards or reference methods are described to quantify house dust mite antigens.
| Pollutant | Reference method | Equivalent method | Technical Characteristics | |
| Maximum allowable errorc | Resolution | |||
| Carbon dioxide (CO2) | Non-dispersive infrared (NDIR) | Electrochemical method; infrared (FTIRd), PAS – photo acoustic sensor | Maximum reference concentration±10% | 1ppm |
| Carbon monoxide (CO) | Non-dispersive infrared (NDIR) | Electrochemical method; infrared (FTIR), PAS – photo acoustic sensor | Maximum reference concentration±10% | 0.1ppm |
| Particulate matter (PM10) | Gravimetric method with size-selective sampling heads PM10 (filter collection and weighing) | Optical dispersion (UV; Laser); absorption of beta radiation; tapered element oscillating microbalance (TEOM); piezoelectrioc resonance | Maximum reference concentration±10% | 1mg/m3 |
| Formaldehyde (HCHO) | Sample collection and chromatography analysis (ISO 16000-2:2006, ISO 16000-3:2001 and ISO 16000-4:2004) | Passive samplers impregnated with DNPHe diffusive sampling method; electrochemical method; impinger method; photometry method | Maximum reference concentration±20% | 0.01ppm |
| Total volatile organic compounds (TVOC) | Sample collection and chromatographic analysis (ISO 16000 – Part V:2007, Part VI:2004) | Passive samplers (Tenax, activated carbon, etc.); canisters; FID – flame ionization detector; PID – photo ionization detector; PAS – photo acoustic sensor; infrared (FTIR) | Maximum reference concentration±10% | 0.01ppm |
a The reference method is the method set by national, European (EU) or international regulations (e.g., ISO) for the measurement of a specific air pollutant. CEN methods CEN (EN-ISO) are considered reference methods.
b The equivalent method is a measurement method that provides an adequate result when compared to those obtained through the reference method; the difference in the results obtained through the two types of methods is within a certain interval of statistical uncertainty.
c The maximum allowable error is the maximum measurement error when compared to a reference value set by specifications or regulations (the latter corresponds to the maximum reference concentration set by RSECE), regarding a measurement, measurement instrument or measurement system. (ISO/IEC Guide 99-12:2007 International Vocabulary of Metrology – Basic and General Concepts and Associated Terms, VIM).
d Fourier transform infra-red.
e Dinitrophenylhydrazine (DNPH) absorbent solution.
Formaldehyde was determined using the NIOSH 3500 method (chromotropic acid) by visible absorption spectrophotometry, with air samples taken on impingers by active sampling with personal pumps, previously calibrated and verified after sampling.
TVOC were determined according to the International standard ISO 16 000, part 6, by active sampling on Tenax TA sorbent, thermal desorption and gas chromatography using a flame ionization detector (Perkin Elmer Autosystem®, Waltham, Massachussets, USA).
Carbon dioxide and carbon monoxide were measured in all DCC rooms during typical occupancy conditions, using a photoacoustic multi-gas monitor (Model 1312, INNOVA Air Tech Instruments, Ballerup, Denmark).
Duplicate samples of culturable airborne bacteria and fungi were collected indoors and outdoors using the Microbiological Air Sampler MAS-100 (Merck Millipore, Billerica, USA) with a sampling flow rate of 100L/min. Malt extract agar (MEA), trypticase soy agar (TSA) and MacConkey agar plates were used as a collection media for fungi, total bacteria and gram-negative bacteria, respectively. The collected air volume depended on the expected loading, 100L for bacteria and 250L for fungi. Sampling and analysis of fungi and bacteria followed the EN 1309851 and were accredited according to the NP ISO IEQ 17025 standards.52
Dust samples for house dust mite evaluation were collected on filters using a vacuum cleaner with a Dustream™ collector (INDOOR Biotechnologies LTD, Cardiff, Wales). Dust samples were analyzed using an ELISA test to quantify Der p1 and Der f1 mite allergens.
Particulate matter with aerodynamic equivalent diameter<10μm (PM10) were collected using PTFE filters on Personal Environmental Monitors (SKC) attached to personal pumps. The filters were analyzed gravimetrically for particle mass before and after sampling.
In order to determine the origin of the contaminant and to minimize spatial and temporal fluctuations of outdoor pollution, samples of carbon dioxide, carbon monoxide, TVOC, formaldehyde, PM10, bacteria and fungi were collected in the surrounding area of each building at the same time as the indoor measurements. For each measurement, campaign field blanks and laboratory positive controls were included. All sampling pumps used were calibrated before and verified after each sampling campaign.
The thermal comfort evaluation was performed according to the ISO 7730:2005 norm53 and was accredited according to the NP ISO IEQ 17025 standard.52 Measurements of the thermal parameters were conducted with a Thermal Analyzer Brüel & Kjaer Model 1213, equipped with transducers, INNOVA: MM0034 (air temperature), MM0036 (temperature flat radiation), MM0037 (humidity) and MM0038 (air velocity).
VentilationThe effective total air change per hour was determined using passive samplers and homogeneous emission of perfluorocarbon tracers (PFT), as described in standard Nordtest Method VVS 11854 and in ISO Standard 16000-8. This method allows measurement of ventilation over long periods of time because sample volume requirements are very low: sample units do not interfere with daily activities and measurements can be made at the lab instead of on-site. The main disadvantage, however, is that the measurements reflect average ventilation rates and do not reflect differences between time periods or compartments with ventilation heterogeneity.
Four to eight activity rooms were monitored for a two-week period during January 2012. The number of rooms was chosen according to the range of children age groups in each DCC, room availability and technical feasibility issues.
In order to perform the measurements, PFT sources were positioned in each room, with tracer gas emission rates adjusted to the room volumes. The tracer gas diffused out of the sources with a known constant rate and mixed with the room air. To measure the time-averaged concentration of the tracer gas in rooms, an integrating sampling was performed, using diffusive samplers. Given that the rooms under investigation were not isolated but connected to the rest of the building by corridors or connecting rooms, a second tracer gas was spread in the spaces outside the measured rooms in order to distinguish between inflow of outside “fresh air” and inflow of “old” air from the rest of the building.
PENTIAQ A.B., Sweden, supplied the PFT sources and samplers and performed the analysis of their content. Estimated precision, including the repeatability and reproducibility, is within 10% and systematic errors will likely yield <5% deviation from the true value.
Allergic and respiratory health evaluationRespiratory health was evaluated at baseline of Phase II (between March and April 2011) by using the full version of the ISAAC questionnaire. This questionnaire collected detailed data on wheezing and allergic diseases, absenteeism, respiratory infections, past medical history and also included environmental questions. As in the previous phase, questionnaires were handed out to parents by the DCC staff.
In order to evaluate recent symptoms (in the previous two months) of respiratory diseases, two follow-up health questionnaires were also distributed: one in May 2011 (for March and April health condition) and one in February 2012 (for December 2011 and January 2012). The follow-up questionnaires measured how often in the given period of time the child coughed, was wheezy, showed symptoms of rhinitis, a respiratory infection, otitis and pneumonia and needed an antibiotic; and how often respiratory diseases led to DCC absenteeism, need to consult a doctor, go to an emergency department and be admitted to hospital.
Airway inflammationThis task was only performed in Lisbon during Visit 2. Children aged between 4 and 5 years were invited for exhaled breath condensate (EBC) collection so as to determine airway inflammation biomarkers (pH and total nitrites/nitrates). A limit of 100 EBC collections was established due to budgetary constraints.
EBC was collected over a period of 15min using an R-Tube (Respiratory Research Inc., Austin, TX, USA). pH was measured through a glass microelectrode (Hi 9025, Hanna Instruments, Italy) after deaerating the sample with argon. Nitrate levels were determined through a chemoluminescence method by reaction with vanadium trichloride and release of nitrous oxide with a Sievers 280i NOA™ analyser (Sievers Instruments, Inc., CO, USA).
Respiratory virus collectionCarers were given a free telephone number to report to the study team any respiratory infection. After each call, the medical team collected swab samples from the oro- and naso-pharynx of the sick children. The samples were tested for the following viruses: adenovirus, influenza A and B, parainfluenza 1–4, respiratory syncytial virus, rhinovirus, enterovirus, human metapneumovirus, human bocavirus and coronavirus. Virus detection was performed through polymerase chain reaction amplification of viral nucleic acids in swab samples. These were extracted with the EZ1 Virus Mini Kit™ v2.0, and amplification reactions and detection of products were performed using the Rotorgene™ PCR system (QIAGEN, Hilden, Germany).
Parental and child stress evaluationThe adults’ psychological (anxiety/depression), parental (parenting stress and life events) and marital (satisfaction) dimensions were evaluated using the following instruments: The Hospital Anxiety and Depression Scale,55 The Parenting Stress Index – Short Form,56 The Life Stress Scale of the Parenting Stress Index-Long Form,57 and The Portuguese Marital Satisfaction Scale.58 All these questionnaires are validated for the Portuguese language.
A cortisol test was done in 24-h urine samples to study its association with children's stress. Urine samples were collected from children aged 4–6 years. The parents were instructed to collect the child's urine during the weekend and complet the questionnaires in the same week. During Visit 1, urine samples were collected from 127 children. During Visit 2, only 98 of those 127 provided a second urine sample.
Ethical issues and authorizationsThe study was carried out according to the Helsinki Declaration and was approved by the following authorities: the Ethics Committee from Faculdade de Ciências Médicas, the National Committee on Data Protection, the Social Security Institute and national authorities representing solidarity institutions (Confederação Nacional de Instituições de Solidariedade e União das Misericórdias Portuguesas). The selected DCCs were only included in the study after approval by their respective administration boards. Only those children whose carers gave their signed and informed consent, were included.
Data management and statistical analysisData gathered during the study was recorded on a Microsoft Access™ database. This database was developed specifically for the study by the research team in order to record the large amount of data. Data input was the responsibility of only a few people and was checked to ensure that all records were correctly introduced.
A cluster analysis (hierarchical model – Ward method) that considered CO2 concentrations, temperature and humidity indoors, measured in Phase I, was used in order to select the 20 DCCs for Phase II. DCCs that were further apart in the dendrogram were chosen.
An exploratory analysis of the variables of interest was carried out using classic descriptive statistics to calculate frequencies, means, medians and associated dispersion measures and confidence intervals for population demographics, DCC characteristics, exposure values and health parameters. Parametric and non-parametric tests of hypothesis were used as appropriate. Crude and adjusted odds-ratios and regression coefficient estimates were calculated with corresponding 95% confidence intervals. Logarithmic transformation and adjustments for confounders were carried out when necessary. These were followed by more complex statistical methods such as regression models that considered the structure of dependence between individuals within the same class/institution. Parameters of these models were estimated through mixed effects models. In Phase I, two-level logistic random-intercept models were used to take into account DCCs. In Phase II, three-level logistic random-intercept models were used, as children were nested in rooms and classrooms were nested in DCCs. Different variables collected from the literature were analyzed as potential confounders: age, gender, personal history of atopic dermatitis, parental history of allergic respiratory disease, parental education, parental smoking, existence of older siblings, air conditioning, dampness and pets at home, breastfeeding, birth and gestational weight, and city and home surroundings.
The level of significance considered was α=0.05, although p-values >0.05 and <0.1 will still be considered for reporting. This data analysis will be performed for both phases of the project with the software STATA (StataCorp LP, Stata Statistical Software: Release 12; TX, USA). ALP is responsible for the data management and statistical analysis.
Computer ventilation modelingThe software CONTAM59 (version 3.0.1.1; Walton and Dols, 2010) was used to model the airflow in the DCCs. It was considered that the air permeability of the envelope was due to just windows and doors, and the measured air permeability was extrapolated considering the length of the opening joint and, where relevant, the extent of the gap between the casement and the ground sill. The pressure coefficients of windows and doors were estimated on the basis of what is recommended under EN 1991-1-4, where the pressure coefficients considered are the average values for exposed façades. Where the façade was sheltered by other buildings, the pressure coefficient of the downstream façade was used to determine the wind direction. The pressure coefficient considered for roof windows was −1.0 and did not depend on wind direction.
In order to simulate ventilation conditions similar to CO2 gas tracer tests, steady-state conditions, the weather data and PFT results were considered. The model was then used to sequentially calculate ventilation changes in different situations: opening or closing doors/windows in different combinations, changing the ventilation sources and schedules.
ResultsData collection was carried out successfully. Data analysis is still ongoing and almost completed. We have already presented preliminary results at scientific meetings and promoted public discussions about the study.60 Formal recommendations to national authorities and public education materials will be made available in written documents. The number of evaluations performed in each task is summarized in Table 2.
Number of observations in the different tasks of the study.
| Phase I | Phase II | ||
| December 2010 | Visit 1 (“Spring”)March–May 2011 | Visit 2 (“Winter”)December 2011–February 2012 | |
| Building characteristicsa | 45 (100%) | – | – |
| Ventilation surrogates (CO2)a | 45 (100%) | 19 (95%) | 17 (85%) |
| Ventilation (PFT)a | – | – | 16 (80%) |
| Air pollutantsa | – | 19 (95%) | 17 (85%) |
| Health screening questionnaires | 3186 (61.7%) | – | – |
| ISAAC questionnaires | – | 1221 (53.4%) | – |
| Recent complaints (“follow-up”) questionnaires | – | 755 (33%) | 667 (29.2%) |
| Exhaled breath condensate | – | – | 100 |
| Virus collections | – | – | 94 |
| Parental stress questionnaires | – | 533 | 255 |
| Urine cortisol test | – | 127 | 98 |
Building and IAQ characteristics refer to the number of DCCs evaluated. Health variables relate to the number of children evaluated. Percentages represent the proportion of individuals (DCCs or children) evaluated out of the eligible population at a given time point and “–” means that measurement was not applicable at that time.
During Phase I we collected data on 45 DCCs (25 in Lisbon and 20 in Oporto). All participating and non-participating DCCs were included in the same management model (IPSS). As DCC selection procedure was stratified according to the district, the proportion of social strata/residential areas was expected to be similar in both participating and non-participating DCCs. Despite this, the non-participating DCCs could not be visited and no data was available to allow us to compare building characteristics with those of participating DCCs.
The age of the buildings was very diverse with a median age of 50 years (P25–P75: 20–134) – the oldest built in 1579 and the most recent in 2008.
In Phase I, CO2 was used to select the DCCs to be included in Phase II as it allowed sampling of DCCs in two different clusters insofar as ventilation was concerned. The first cluster included 4 DCCs in Lisbon and 5 in Oporto. Average CO2 levels, indoor temperature and relative humidity were 2137±368ppm, 18.7±2.2°C and 57.4±5.0%, equivalent to the cluster with worst ventilation conditions. The second cluster included 7 DCCs in Lisbon and 4 in Oporto. Average CO2 levels, indoor temperature and relative humidity were 1233±170ppm, 20.1±1.8°C and 45.6±5.9%, equivalent to the cluster with better ventilation. CO2 (p<0.001), indoor temperature (p=0.025) and relative humidity (p<0.001) differed significantly between the two clusters.
Phase I questionnaire allowed us to collect some data on parental education, medical history and smoking at home. It was also possible to estimate the prevalence of wheezing in the previous 12 months, atopic dermatitis, reported asthma and food allergy. As for the response rate, 3186 out of 5161 questionnaires were returned (61.7%). About half of the sample (50.5%) were boys and the average age was 3.1±1.5 years.
During Phase II we had one DCC drop out during Visit 1 and two others during Visit 2. Indoor air quality was evaluated in 19 DCCs during Visit 1 and in 17 DCCs during Visit 2. Measurements included thermal comfort parameters, CO, CO2, PM10, TVOC, formaldehyde, bacteria, molds and dust mites. Information regarding indoor and outdoor values was collected.
Objective ventilation measures were gathered during Visit 2 from 16 DCCs (7 in Lisbon and 9 in Oporto). The ventilation data are being used to create modeling software that may be useful in future studies.
In relation to the questionnaires used in Phase II, we had different return rates. Of the 2287 ISAAC questionnaires handed out, 1221 were returned (53.4%). The average age of the sample was 3.5±1.5 years, and 52.4% were boys.
Data concerning non-respondents were available only for the DCCs included in Phase II, as many institutions considered these data confidential. With regard to the ISAAC questionnaire, no statistical differences were found for gender (p=0.700) and age (children under 3 years versus children over 3 years: p=1.00) between respondents and non-respondents. When the Phase I and Phase II samples were compared in terms of gender and age, the only significant difference between Phase I and the ISAAC questionnaire was that children in Phase II were slightly older.
As for the questionnaires used to evaluate recent respiratory symptoms (follow-up questionnaires), 755 out of 1221 were answered during Visit 1 (53.3% of boys with an average age of 3.5±1.5 years) and 667 out of 1411 during Visit 2 (54% of boys with an average age of <3.2±1.6 years).
During Visit 2, nitrates/nitrites and pH were measured in 100 exhaled breath condensate samples collected in Lisbon DCCs, and 94 samples from children of different DCCs were collected and tested for respiratory viruses, out of the target population of 1411 children. Finally, parental stress questionnaires were collected during both visits.
DiscussionENVIRH is the first Portuguese study addressing the effect of IAQ on children less than six years old, in a multidisciplinary perspective through objective measurements of IAQ, ventilation, building characteristics and health outcomes. This paper reviews its rationale and outlines methods that might be implemented by other investigators conducting studies on the association between these variables.
The major strengths of the study are the inclusion of a sample of carefully selected DCCs, the longitudinal approach, the detailed characterization of each DCC and the complex statistical analyses that took into consideration the correlation structure of the observations for each classroom/DCC.
Our study has evaluated a considerable number of DCCs and children. Air pollutant patterns could vary according to the environment studied.61
It might have been interesting to include in our DCC sample institutions from urban and rural settings; however – like other Portuguese authors – we decided to study only urban areas, namely Lisbon20,36,37 and Oporto.62 This allowed us to study a larger number of DCCs and limited the environmental confounding that we would have found if we had also included DCCs from rural settings.
There were some concerns about the representativity of our sample in Phase II as we were unable to study a large sample of DCCs. To address this issue we designed the study in two main phases. During Phase I we assessed a larger sample, and during Phase II a more detailed evaluation was conducted.
The participation rate was lower than in other epidemiological studies which also used the ISAAC questionnaire in this age group.7,63 The different types of assessments (through questionnaire and biological fluids) and the requests for ongoing follow-up may have influenced the decision to participate in a study that could have taken up a substantial amount of time. The need for active consent64 might also have influenced the final number of participants as we only handed out questionnaires to those parents who gave written consent. Despite this limitation, the male–female proportion and the average age were similar across the different questionnaires.
CO2 levels were used to divide the Phase I DCCs into two different clusters in terms of ventilation, which were then included in Phase II. This was possible because CO2 is an established marker of building ventilation65 and together with occupancy could be used to develop effective models to predict room ventilation.66 Phase II was designed to include two evaluations at different times with a dual purpose: ensuring seasonal variety and enabling a longitudinal evaluation. The first and comprehensive evaluation of children's health took place during the Spring of 2011 using the ISAAC questionnaire. It set the respiratory and environmental baseline characteristics for the participating children. The first follow-up questionnaire was distributed shortly after, during the Spring, and allowed us to gather information about recent health events. This questionnaire was then repeated during the Winter, 9 months after the first evaluation.
IAQ parameters were also collected from the DCCs during Spring and Winter in order to study the association between IAQ parameters and respiratory events. Studies have shown that there are seasonal variations in indoor pollutant levels.37,61 Pegas et al. showed in a group of Lisbon elementary schools that bioaerossols and CO2 levels were above the recommended limits in different seasons and some volatile organic compounds concentrations were higher during the Winter.37
As different patterns of indoor air pollutants can be found throughout the year, seasonal studies are relevant in order to identify specific problems for the time of the year in order to plan effective actions.
The cross-sectional part of our study, performed in each phase, will allow us to study the association between DCC IAQ and respiratory symptoms in young children. For this purpose we took into consideration different variables reported in the literature as confounders. ISAAC questionnaire was used to collect information about those covariates related not only to the children, but also to the home environment.
ENVIRH also included a longitudinal part to study causal associations, as we planned to follow-up with the participating children. However, the decrease in the participation rate across the study will limit this objective.
Different indoor air pollutants have been associated with respiratory diseases or symptoms.15 ENVIRH was designed to study IAQ as thoroughly as possible. Adding PM2.5 would be interesting because of their impact on lower airways.1 However, it has been shown that exposure to PM10 is associated with respiratory disease15 and airway inflammation biomarkers,22 making it acceptable for our purposes.
Carbon dioxide level was measured in both phases and visits because it is a surrogate of ventilation. Although a more specific quantification was needed to create ventilation model software, PFT technique was used only in a few DCCs and during Visit 2, because it is burdensome. PFT technique to determine air infiltration rates at homes and buildings, has been reported in several studies,67,68 while its applicability and effectiveness have been discussed elsewhere.69,70 Ventilation studies are important because this variable not only reflects IAQ but, when considering interventions to improve exposure to pollutant, also shows that improving ventilation will positively affect all airborne contaminants. We also looked at air pollutants outside the DCCs in order to differentiate indoor from outdoor sources. It might be interesting in future studies to determine the contribution of the outdoor to IAQ by analyzing traffic patterns in the surrounding areas, as it may be another intervention target.
The ISAAC questionnaire has been an important validated tool in different epidemiological studies all over the world. In order to get a more objective picture of the airways, we measured some inflammatory biomarkers in the EBC; however, due to funding limitations we only collected 100 samples. EBC study could be very useful as it is a non-invasive and easy-to-collect technique and allows the measurement of different markers. Different studies showed that nitrogen products and pH in EBC were associated with asthma and FEV1 deterioration.71 As far as pH is concerned, an association was found between benzene, NO2 and PM10 levels and EBC acidity.22
Another constraint we faced was the low number of children from whom virus swabs were collected, despite the efforts of our team who held several public discussions with parents and DCC staff. This may be because of parents’ concern about the technique and not appreciating the importance of this aspect of the study. Although we should note that after the Influenza H1N1 alert in 2011 the study compliance increased dramatically.
Stress evaluation is an emerging issue in childhood respiratory disease studies. It has been shown that chronic stress in the family may lead to children's respiratory infections or diseases.72 Parental stress levels were assessed by validated instruments. Children's stress levels were inferred from cortisol levels measured in 24h urine samples to monitor for circadian rhythm alterations. This approach is validated, although results need to be interpreted carefully when assessing children <3 years of age, as urinary cortisol levels could rise during DCC attendance in this age group.73 This was not relevant to our study as urine was collected only in children over 4 years of age.
Our main concern in ENVIRH was to contribute to healthier environments for children. This issue is regarded as a priority by the World Health Organization and the European Commission.74,75 Improving children's health is such a major concern, not only for its short-term effects, but also because it will lead to a physically, psychologically and socially healthier individual. With that in mind, some particularly important outcomes for our study were: contributing to public education and making recommendations to national authorities; and creating modeling software for the analysis of ventilation patterns. Public education should be the mainstream of all interventions involving the population, contributing to a healthy and conscious lifestyle and to greater awareness of diseases and associated risks.
DCC staff representatives, parents’ associations and health authorities were invited to participate in the study seminars. The next objective will be to contribute to recommendations, as it has been shown that when there are formal IAQ programs it is more likely that institutions will implement the necessary changes and strategies to improve IAQ.76
In addition, legislation relating to DCCs may be a good starting point to improve respiratory health in children, regulating cost-effective changes for environments where children spend a significant amount of time. Modeling software for ventilation studies may also prove valuable toward these ends, from two perspectives: research and policy implementation. For research in other settings, models may prove as valuable, reliable and more affordable instruments to calculate IAQ parameters than direct measurements, even if they retain some limitations.77,78 They may also be useful for building design and ventilation strategies in some cases78,79 and could be used to predict the health impact and costs of specific situations and interventions, bringing together engineers, physicians and policy makers.
ConclusionStudies on IAQ and children's respiratory health need to be carried out as there are few publications on this subject. Most data come from areas of the world with different building and environmental characteristics (building stock, construction materials, cleaning and ventilation habits in DCC and climate). For this reason, national studies designed to address specific regional needs, should be conducted.
We recommend addressing these issues in multidisciplinary teams, creating knowledge that could be readily transmitted to the community, thus helping to improve the health of populations in the short and long terms.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThe activities of project ENVIRH were funded by research grants from national funds attributed by Fundação para a Ciência e Tecnologia (Project references – PTDC/SAU-ESA/100275/2008 and PEST-OE/MAT/UI0006/2011).
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors express their deepest gratitude to the parents and to the children as well as to the carers for their important contribution. We also thank all the other DCC staff and authorities involved in the study.
The authors also thank Prof. Maria Guarino for contributing with nitrate measurements.
This manuscript details the research protocol used in the ENVIRH study, a multidisciplinary initiative that included five different institutions. For this motive the present manuscript has more than six authors. All the authors contributed to the conception, design, collection of data or analysis and interpretation of data, article drafting and revision.


