


In Portugal, Outpatient Tuberculosis Centres (OTBC) are responsible for the diagnosis, treatment, screening and prevention of tuberculosis (TB), and only severe or resistant cases are hospitalized.
AimTo understand how infection control norms and standards were applied and how these centres responded during the pandemic.
MethodWe sent an electronic questionnaire to all coordinators of OTBC. The questionnaire included questions on infection control during the COVID-19 pandemic and evaluation of the functioning of the OTBC in two periods: during the 1st National State of Emergency and after 1 year.
ResultsThirty-two responses were obtained (52.5%). The infection control norms were globally applied; diagnosis, treatment, and prevention were kept, and contact screening was only affected during the 1st State of Emergency. However, half of the respondents (53.1%) believed that there were diagnostic delays during the 1st State of Emergency, rising to 68.8% after 1 year. Only 31.3% performed Directly Observed Therapy (DOT) in all patients during the 1st State of Emergency, and 59.4% after 1 year. Half the inquiries expected an increase in TB incidence in the near future.
ConclusionThe pandemic affected OTBC functioning, although the services were kept open; diagnostic delay and DOT appliance were the most affected.
Since the beginning of 2020, the coronavirus disease 2019 (COVID-19) pandemic has caused a significant disruption in all areas of healthcare worldwide.1–3 The functioning and response of many health services, including tuberculosis (TB) services, were profoundly affected by the policies adopted to respond to the pandemic, such as country lockdowns, reallocation of health professionals, materials, and diagnostic tools, and reduction of outpatient care.4–8
Hence, it is not surprising that several studies, carried in high-burden countries for TB, report a significant decrease in TB detection and notifications in the first months of the pandemic.9–11 Following this, a modelling analysis from Glaziou12 and the “Stop TB Partnership”13 predicted, for a 3-month lockdown period, an annual increase in TB deaths between 200,000 – 400,000, raising the total deaths to ∼1.6 – 1.8 million, numbers comparable to the ones seen between 2012 and 2015.12,13
Low-burden countries for TB also report significant changes in TB detection and patient care. A study carried out in Spain compared data from March-June in 2019 and 2020, and described an increase in latent and active TB in children of patient households (5.3% vs 7.7% in 2019 and 2020, respectively, p < 0.001); additionally, patients with the active disease diagnosed during the pandemic showed more severe manifestations.14
In a worldwide study by the Global Tuberculosis Network, a significant decline in detection of TB (and multidrug-resistant TB) cases and TB infection was observed, with an increase in telehealth consultations.2
Although much was written on the impact of COVID-19 on TB services and workplace safety resulting from infection control practices, not much is known on this,15,16 and country-specific analyses are not available.
In Portugal, before the pandemic, there was a downward trend in the incidence and notification rate of TB over the last 10 years.17 Between 2015 and 2019, there was a 24.6% decrease in the notification rate, placing it at 17.2 cases per 100 thousand inhabitants in 2019, with an estimated incidence rate of 19.0 cases per 100 thousand inhabitants.18 The National Tuberculosis Program is responsible for the monitoring and surveillance of TB; implementing control and elimination strategies, action plans, and protocols for the management of the disease.19
The diagnosis, screening, treatment, and follow-up of individual patients are performed at Outpatient TB Centres (OTBC), overseen by the National Tuberculosis Program. Aguiar et al.20 already described the adaptions made by one Portuguese OTBC during the pandemic, like the establishment of teleconsultations for individuals with presumptive TB, or the improvement of digital connectivity solutions between professionals. Still, different OTBC may have faced other problems and opted for different strategies - considering the panorama of the disease being different in the sub-regions of the country.21,22
Through the Directorate-General of Health, the Portuguese Government has published several norms and orientations regarding infection control in healthcare units during the pandemic.23–25 Those included: the provision of a surgical mask (if the user does not have his/her mask) and provision of sanitizing solution at entrance to clinic, as well as FFP2 masks and individual protection equipment to healthcare professionals; the need to keep a safe distance from other people; frequent surface washing and disinfection; the creation and regular update of a COVID-19 Contingency Plan made known to all professionals.23–26
In this study, we aimed to: understand how the different national OTBC have adjusted to comply with the above infection control norms and standards; to perceive the OTBC's coordinators’ perception regarding their centres’ responsiveness to the restrictive measures and adjustments during the pandemic and its impact on tuberculosis diagnosis, treatment, and screening. Finally, we aimed to compare the Portuguese experience with that of other countries.27
MethodsStudy design and study populationWe conducted a cross-sectional study using an electronic online questionnaire created in Google Forms. A pilot survey was performed in two OTBC to assess the questionnaire's relevance and understandability, and the final version was sent via e-mail to all OTBC's coordinators. The National Tuberculosis Program provided the list with the coordinator's electronic addresses. Responses were collected during March and April 2021. Participation was entirely voluntary, and the anonymity of the participants was ensured.
Ethical approvalEthical approval was obtained from the Ethics Committee of the Institute of Public Health of the University of Porto on September 19, 2020 (reference CE20170).
According to the Ethical Principles for Medical Research involving human subjects expressed in the Declaration of Helsinki and the current national legislation, all participants are asked to give their informed consent. Furthermore, because this was an online survey, participants had to choose “I accept to participate” to continue with the questionnaire.
Data collectionAn online questionnaire was prepared. The questionnaire consisted of 32 questions, divided into three sections. The first part contained 4 demographic questions: age, sex, profession, and workplace. To guarantee the anonymity of the responders and further explore possible asymmetries between regions, workplaces were grouped into Regional Health Administrations: North, Centre, Lisbon and Tagus Valley, Alentejo, and Algarve (Fig. 1).

The second part (8 questions) addressed infection control measures during the pandemic, namely the provision of alcoholic solutions and masks to professionals and patients; the existence of personal protective equipment; the correct disinfection of places and surfaces; and the existence of a contingency plan, in accordance with the norms of the Directorate-General of Health.11-12
Finally, the third section (20 questions) aimed to evaluate the functioning of the OTBC in two distinct periods: during the 1st State of Emergency (an exceptional national state, declared by the President of the Republic, that took place from March 18, 2020, to May 2, 2020, in which a set of measures like partial suspension of rights, freedoms, and guarantees of citizens took place, in order to face a possible public calamity), and at the date in which participant answered to the questionnaire (1 year after the 1st State of Emergency). The questions addressed the following topics: consultation and teleconsultation; patient's resource to the OTBC; delays in the diagnosis of active disease; follow-up and treatment of patients with active or latent disease; screening of contacts of patients with active disease; screening of patients’ candidate for biological therapy; and management of directly observed therapy (DOT).
Questions were mostly closed (e.g., yes/no), but contained an “other” option where inquires could justify their answers, when appropriate. The last question was completely open, and responders were free to share their final comments.
Comparison with other countriesThe results of the survey were compared with the findings of a recent Global Tuberculosis Network study.2
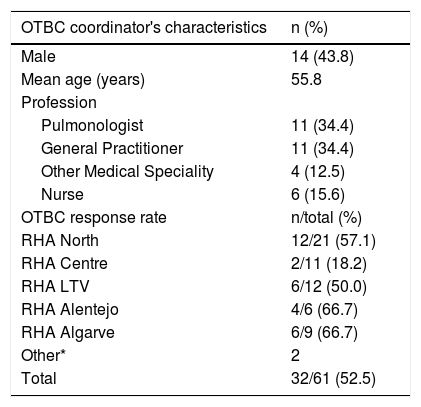
ResultsThirty-two OTBC coordinators accepted to answer the questionnaire, from a total of 61 (52.5% response rate). The Regional Health Administrations most represented were Alentejo and Algarve, with a 66.7% response rate each. Two locations were kept undisclosed (one didn't answer, and the other was not revealed to protect the anonymity of the responder). OTBC coordinator's characteristics and response rate by region are summarised in Table 1.
Outpatient Tuberculosis Centres coordinator's characteristics and response rate by region.
| OTBC coordinator's characteristics | n (%) |
|---|---|
| Male | 14 (43.8) |
| Mean age (years) | 55.8 |
| Profession | |
| Pulmonologist | 11 (34.4) |
| General Practitioner | 11 (34.4) |
| Other Medical Speciality | 4 (12.5) |
| Nurse | 6 (15.6) |
| OTBC response rate | n/total (%) |
| RHA North | 12/21 (57.1) |
| RHA Centre | 2/11 (18.2) |
| RHA LTV | 6/12 (50.0) |
| RHA Alentejo | 4/6 (66.7) |
| RHA Algarve | 6/9 (66.7) |
| Other* | 2 |
| Total | 32/61 (52.5) |
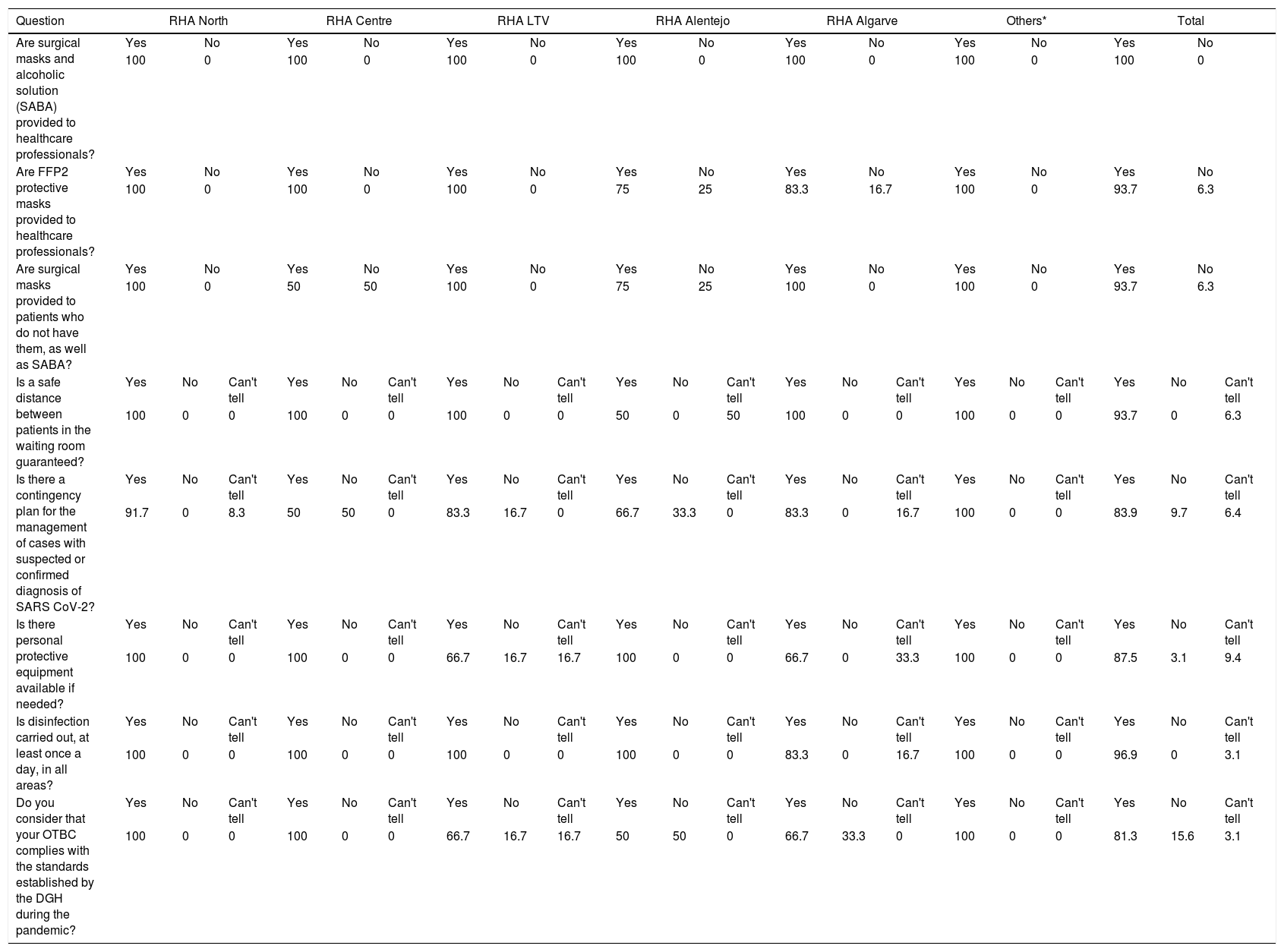
Answers concerning hygiene and safety measures during the pandemic are summarised in Table 2. Surgical masks and alcohol sanitizing solution were provided to healthcare professionals in all OTBC, but FFP2 masks were not supplied in 2 centres. Also, in 2 centres, patients were not routinely provided with surgical masks or sanitizing solution. Disinfection of common areas was carried out, at least once a day, in all OTBC except one.
Compliance to hygiene and safety measures during the pandemic. Results are presented as relative frequencies (%).
| Question | RHA North | RHA Centre | RHA LTV | RHA Alentejo | RHA Algarve | Others* | Total | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Are surgical masks and alcoholic solution (SABA) provided to healthcare professionals? | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | |||||||||||||||
| Are FFP2 protective masks provided to healthcare professionals? | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | 75 | 25 | 83.3 | 16.7 | 100 | 0 | 93.7 | 6.3 | |||||||||||||||
| Are surgical masks provided to patients who do not have them, as well as SABA? | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||||||||
| 100 | 0 | 50 | 50 | 100 | 0 | 75 | 25 | 100 | 0 | 100 | 0 | 93.7 | 6.3 | |||||||||||||||
| Is a safe distance between patients in the waiting room guaranteed? | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | |||||||
| 100 | 0 | 0 | 100 | 0 | 0 | 100 | 0 | 0 | 50 | 0 | 50 | 100 | 0 | 0 | 100 | 0 | 0 | 93.7 | 0 | 6.3 | ||||||||
| Is there a contingency plan for the management of cases with suspected or confirmed diagnosis of SARS CoV-2? | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | |||||||
| 91.7 | 0 | 8.3 | 50 | 50 | 0 | 83.3 | 16.7 | 0 | 66.7 | 33.3 | 0 | 83.3 | 0 | 16.7 | 100 | 0 | 0 | 83.9 | 9.7 | 6.4 | ||||||||
| Is there personal protective equipment available if needed? | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | |||||||
| 100 | 0 | 0 | 100 | 0 | 0 | 66.7 | 16.7 | 16.7 | 100 | 0 | 0 | 66.7 | 0 | 33.3 | 100 | 0 | 0 | 87.5 | 3.1 | 9.4 | ||||||||
| Is disinfection carried out, at least once a day, in all areas? | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | |||||||
| 100 | 0 | 0 | 100 | 0 | 0 | 100 | 0 | 0 | 100 | 0 | 0 | 83.3 | 0 | 16.7 | 100 | 0 | 0 | 96.9 | 0 | 3.1 | ||||||||
| Do you consider that your OTBC complies with the standards established by the DGH during the pandemic? | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | Yes | No | Can't tell | |||||||
| 100 | 0 | 0 | 100 | 0 | 0 | 66.7 | 16.7 | 16.7 | 50 | 50 | 0 | 66.7 | 33.3 | 0 | 100 | 0 | 0 | 81.3 | 15.6 | 3.1 | ||||||||
In 83.9% of all OTBC, there was a contingency plan for managing cases with suspected or confirmed SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus-2). The majority (81.3%) considered that their OTBC complied with the safety standards established by the Directorate-General of Health.
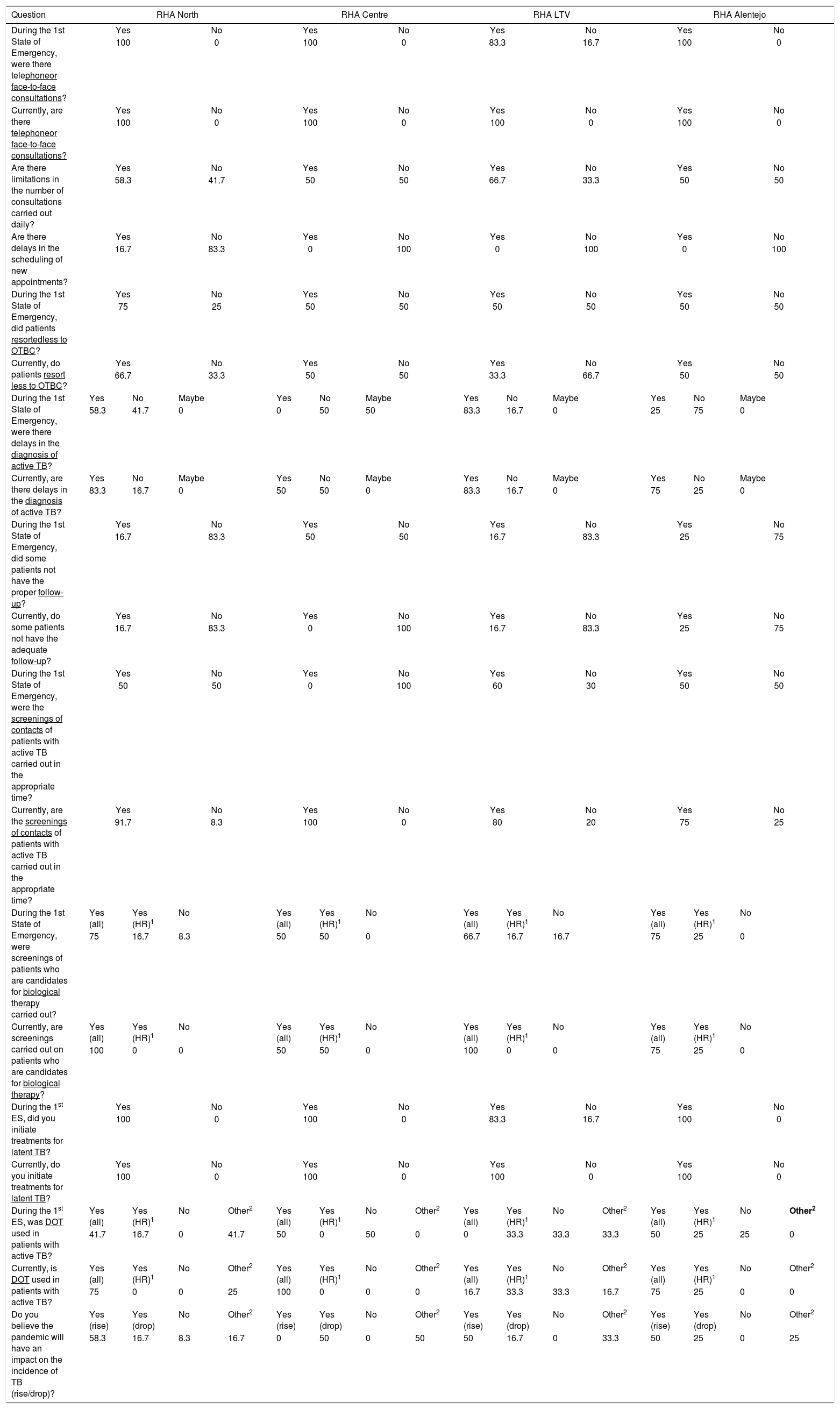
Functioning of the outpatient TB centresComparing the functioning of the OTBC during the 1st State of Emergency and after 1 year (Table 3), responders stated that those consultations (face-to-face and/or by telephone) were maintained in both periods (except during the 1st State of Emergency). Almost 60% reported limitations in the number of consultations carried out daily, although only 6.3% referred to delays in scheduling new appointments.
Functioning of the Outpatient Tuberculosis Centres during the 1st State of Emergency (SE) and at the current date. Results are presented as relative frequencies (%).
| Question | RHA North | RHA Centre | RHA LTV | RHA Alentejo | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| During the 1st State of Emergency, were there telephoneor face-to-face consultations? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 100 | 0 | 100 | 0 | 83.3 | 16.7 | 100 | 0 | |||||||||
| Currently, are there telephoneor face-to-face consultations? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | |||||||||
| Are there limitations in the number of consultations carried out daily? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 58.3 | 41.7 | 50 | 50 | 66.7 | 33.3 | 50 | 50 | |||||||||
| Are there delays in the scheduling of new appointments? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 16.7 | 83.3 | 0 | 100 | 0 | 100 | 0 | 100 | |||||||||
| During the 1st State of Emergency, did patients resortedless to OTBC? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 75 | 25 | 50 | 50 | 50 | 50 | 50 | 50 | |||||||||
| Currently, do patients resort less to OTBC? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 66.7 | 33.3 | 50 | 50 | 33.3 | 66.7 | 50 | 50 | |||||||||
| During the 1st State of Emergency, were there delays in the diagnosis of active TB? | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | ||||
| 58.3 | 41.7 | 0 | 0 | 50 | 50 | 83.3 | 16.7 | 0 | 25 | 75 | 0 | |||||
| Currently, are there delays in the diagnosis of active TB? | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | ||||
| 83.3 | 16.7 | 0 | 50 | 50 | 0 | 83.3 | 16.7 | 0 | 75 | 25 | 0 | |||||
| During the 1st State of Emergency, did some patients not have the proper follow-up? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 16.7 | 83.3 | 50 | 50 | 16.7 | 83.3 | 25 | 75 | |||||||||
| Currently, do some patients not have the adequate follow-up? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 16.7 | 83.3 | 0 | 100 | 16.7 | 83.3 | 25 | 75 | |||||||||
| During the 1st State of Emergency, were the screenings of contacts of patients with active TB carried out in the appropriate time? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 50 | 50 | 0 | 100 | 60 | 30 | 50 | 50 | |||||||||
| Currently, are the screenings of contacts of patients with active TB carried out in the appropriate time? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 91.7 | 8.3 | 100 | 0 | 80 | 20 | 75 | 25 | |||||||||
| During the 1st State of Emergency, were screenings of patients who are candidates for biological therapy carried out? | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | ||||
| 75 | 16.7 | 8.3 | 50 | 50 | 0 | 66.7 | 16.7 | 16.7 | 75 | 25 | 0 | |||||
| Currently, are screenings carried out on patients who are candidates for biological therapy? | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | ||||
| 100 | 0 | 0 | 50 | 50 | 0 | 100 | 0 | 0 | 75 | 25 | 0 | |||||
| During the 1st ES, did you initiate treatments for latent TB? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 100 | 0 | 100 | 0 | 83.3 | 16.7 | 100 | 0 | |||||||||
| Currently, do you initiate treatments for latent TB? | Yes | No | Yes | No | Yes | No | Yes | No | ||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | 100 | 0 | |||||||||
| During the 1st ES, was DOT used in patients with active TB? | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 |
| 41.7 | 16.7 | 0 | 41.7 | 50 | 0 | 50 | 0 | 0 | 33.3 | 33.3 | 33.3 | 50 | 25 | 25 | 0 | |
| Currently, is DOT used in patients with active TB? | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 |
| 75 | 0 | 0 | 25 | 100 | 0 | 0 | 0 | 16.7 | 33.3 | 33.3 | 16.7 | 75 | 25 | 0 | 0 | |
| Do you believe the pandemic will have an impact on the incidence of TB (rise/drop)? | Yes (rise) | Yes (drop) | No | Other2 | Yes (rise) | Yes (drop) | No | Other2 | Yes (rise) | Yes (drop) | No | Other2 | Yes (rise) | Yes (drop) | No | Other2 |
| 58.3 | 16.7 | 8.3 | 16.7 | 0 | 50 | 0 | 50 | 50 | 16.7 | 0 | 33.3 | 50 | 25 | 0 | 25 | |
| Question | RHA Algarve | Others* | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| During the 1st State of Emergency, were there telephoneor face-to-face consultations? | Yes | No | Yes | No | Yes | No | ||||||||||
| 100 | 0 | 100 | 0 | 96.9 | 3.1 | |||||||||||
| Currently, are there telephoneor face-to-face consultations? | Yes | No | Yes | No | Yes | No | ||||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | |||||||||||
| Are there limitations in the number of consultations carried out daily? | Yes | No | Yes | No | Yes | No | ||||||||||
| 50 | 50 | 100 | 0 | 59.4 | 40.6 | |||||||||||
| Are there delays in the scheduling of new appointments? | Yes | No | Yes | No | Yes | No | ||||||||||
| 0 | 100 | 0 | 100 | 93.7 | 6.3 | |||||||||||
| During the 1st State of Emergency, did patients resortedless to OTBC? | Yes | No | Yes | No | Yes | No | ||||||||||
| 66.7 | 33.3 | 100 | 0 | 64.5 | 35.5 | |||||||||||
| Currently, do patients resort less to OTBC? | Yes | No | Yes | No | Yes | No | ||||||||||
| 83.3 | 16.7 | 50 | 50 | 64.5 | 35.5 | |||||||||||
| During the 1st State of Emergency, were there delays in the diagnosis of active TB? | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | |||||||
| 50 | 50 | % | 0 | 100 | 0 | 50 | 46.9 | 3.1 | ||||||||
| Currently, are there delays in the diagnosis of active TB? | Yes | No | Maybe | Yes | No | Maybe | Yes | No | Maybe | |||||||
| 33.3 | 66.7 | 0 | 50 | 50 | 0 | 68.8 | 31.2 | 0 | ||||||||
| During the 1st State of Emergency, did some patients not have the proper follow-up? | Yes | No | Yes | No | Yes | No | ||||||||||
| 33.3 | 66.7 | 0 | 100 | 21.9 | 78.1 | |||||||||||
| Currently, do some patients not have the adequate follow-up? | Yes | No | Yes | No | Yes | No | ||||||||||
| 16.7 | 83.3 | 0 | 100 | 15.6 | 84.4 | |||||||||||
| During the 1st State of Emergency, were the screenings of contacts of patients with active TB carried out in the appropriate time? | Yes | No | Yes | No | Yes | No | ||||||||||
| 66.7 | 33.3 | 100 | 0 | 58.1 | 41.9 | |||||||||||
| Currently, are the screenings of contacts of patients with active TB carried out in the appropriate time? | Yes | No | Yes | No | Yes | No | ||||||||||
| 100 | 0 | 100 | 0 | 90.3 | 9.7 | |||||||||||
| During the 1st State of Emergency, were screenings of patients who are candidates for biological therapy carried out? | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | |||||||
| 83.3 | 16.7 | 0 | 50 | 50 | 0 | 71.9 | 21.9 | 6.2 | ||||||||
| Currently, are screenings carried out on patients who are candidates for biological therapy? | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | Yes (all) | Yes (HR)1 | No | |||||||
| 100 | 0 | 0 | 100 | 0 | 0 | 93.8 | 6.2 | 0 | ||||||||
| During the 1st ES, did you initiate treatments for latent TB? | Yes | No | Yes | No | Yes | No | ||||||||||
| 100 | 0 | 100 | 0 | 96.9 | 3.1 | |||||||||||
| Currently, do you initiate treatments for latent TB? | Yes | No | Yes | No | Yes | No | ||||||||||
| 100 | 0 | 100 | 0 | 100 | 0 | |||||||||||
| During the 1st ES, was DOT used in patients with active TB? | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | ||||
| 16.7 | 33.3 | 33.3 | 16.7 | 50 | 50 | 0 | 0 | 31.3 | 25 | 18.7 | 25 | |||||
| Currently, is DOT used in patients with active TB? | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | Yes (all) | Yes (HR)1 | No | Other2 | ||||
| 33.3 | 16.7 | 33.3 | 16.7 | 100 | 0 | 0 | 0 | 59.4 | 12.5 | 12.5 | 15.6 | |||||
| Do you believe the pandemic will have an impact on the incidence of TB (rise/drop)? | Yes (rise) | Yes (drop) | No | Other2 | Yes (rise) | Yes (drop) | No | Other2 | Yes (rise) | Yes (drop) | No | Other2 | ||||
| 50 | 16.7 | 33.3 | 0 | 50 | 0 | 50 | 0 | 50 | 18.8 | 12.5 | 18.8 | |||||
More than two-thirds of the respondents considered that, in both periods, there were fewer outpatient visits to the OTBC; three coordinators suggested that this was due to a decrease in referral by other health units. In addition, half of the respondents believed that there were delays in diagnosing active disease in the 1st State of Emergency, increasing to 68.8% after 1 year. Once again, two coordinators referred to delays in referrals from other health units as a possible cause. Regarding patient follow-up, 21.9% considered that it was insufficient during the 1st State of Emergency, in contrast to 15.6% after 1 year. One inquiry mentioned a reduction in DOT, and another delay in referrals, as plausible explanations.
The use of DOT across the different centres varied. During the 1st State of Emergency, only 31.3% reported using DOT with all patients (either face-to-face or video call); 25% report using it only in high-risk patients; 25% used it 1-3 days of the week, via phone call, or with the help of family member; and 18.7% did not use DOT at all. Three responders point to the lack of human resources as the justification for these results. After 1 year, DOT use in all patients increased to 59.4%, but 15.9% continued to report not using DOT in any patient. It is important to highlight that the National Tuberculosis Program recommends DOT in all cases of TB.28
Contact screening for risk individuals was not performed routinely in 41.9% of OTBC during the 1st State of Emergency, decreasing to 9.7% after 1 year; two coordinators mentioned imagological and laboratory delays during the 1st State of Emergency. Screening of high-risk patients who were candidates for biological therapy was carried out in all centres except 2 during the 1st State of Emergency, and in all centres after 1 year. Treatment for latent tuberculosis was carried out in all but one centre during the 1st State of Emergency, and by all centres after 1 year.
Half of the responders believed the pandemic will lead to an increased incidence of TB in Portugal in the near future. On the final question, the following problems were raised: the occupation of the OTBC installations by other services; patients missing their appointments more often since the beginning of the pandemic; fear of the effect of immunosuppression used to treat COVID-19 patients in TB epidemic and severity of the disease; patients fears about to recourse to health units; lack of cameras to make video calls; and delays in patient's referral from primary care units.
DiscussionOverall, there were no apparent asymmetries between Portuguese Regional Health Administrations. However, there were some irregularities in particular areas: one region changed OTBC practice during the 1st State of Emergency, and two had difficulties related to the disposable masks. Regarding the latter, the inquires did not clarify if this happened at the beginning or throughout the pandemic, but several newspapers reported a lack of provision of masks at various health facilities at the onset of the pandemic, particularly in primary care units;29,30 additionally, there were also reports of mask thefts in some units.31 Nevertheless, most OTBC complied with the norms established by the Directorate-General of Health regarding hygiene and safety measures. It should be noted that mask use and hand hygiene was mandatory not only in Portugal, but in most countries worldwide.27
Nearly all were able to maintain treatments for latent TB and screenings of high-risk patients’ candidates for biological therapy. Contact tracing and screening were negatively impacted during the 1st State of Emergency, but significantly improved after one year. Conversely, a worrisome percentage of coordinators mentioned delays in diagnosing active disease and not using DOT in both periods. There was an overall decrease in the number of patients seeking or referred to the OTBC.
The management of latent TB varied between different countries. The Global Tuberculosis Network study reports a decrease in newly diagnosed TB infections in 2020, comparing with 2019 (363 ± 51 per month in 2019 versus 248 ± 76 per month in 2020; p = 0.0007).2 Similarly, Migliori et al.1 conducted a study carried in 33 centres from 16 different countries that evaluated the volume of TB-related healthcare activities in the first 4 months of the pandemic (during national lockdowns), and compared it to the same period in 2019. Most centres reported reductions in newly diagnosed cases of active and latent TB and in total active and latent TB outpatient visits; they explained, furthermore, that some centres didn't consider latent TB a high priority during the pandemic.1 In England, the latent TB program was paused in response to the pandemic,32 and in China, many TB-directed services were closed and reorganized into COVID-19 centres, and presumptive TB patients could not seek medical assistance due to movement restrictions.33 This contrasts with what happened in Portugal: OTBC were kept open, latent TB screening and treatments continued throughout the pandemic, and mobility for health reasons was permitted.
Contact tracing was compromised during the 1st State of Emergency in 41.9% of the OTBC. In comparison Aznar et al.14 investigated 13 Spanish centres during the same period and reported slightly worse results, with 53.8% of centres reporting changes in contact screening programs. Additionally, follow-up of patients was either cancelled or delayed by 76.9%. In our study, only 21.9% considered that patient follow-up was inadequate during 1st State of Emergency. It should also be noted that both contact tracing and patient follow-up improved significantly after 1 year.
Overall, fewer patients accessed the OTBC, which matches what is described in published literature.1,5,14,15,33 Lower referrals from primary care units and patient's fear of contracting the disease were referred to as possible causes. The Regulatory Authority for Health report confirmed that the number of face-to-face appointments in primary care units in Portugal decreased substantially during the 1st State of Emergency (33%, 73%, and 66% during March, April, and May 2020, respectively)34. On the other hand, patient fear was often interpreted as the general decrease in healthcare service's use.1,33,35 Other plausible reasons for this reduction include movement restrictions, enforced isolation measures, and widespread discouragement to seek medical care in health facilities if only mild symptoms were present.1,5
TB diagnostic delays were described in both periods. The reduction of diagnostic and treatment delay is a priority to the National Tuberculosis Program,17 so changes need to be made to reverse this outcome. It is important to note, however, that other countries faced the same problem10,14,33,36 The Global Tuberculosis Network study reports a significant decline in newly diagnosed TB disease in outpatient clinics (613 ± 57 per month in 2019 versus 475 ± 90 per month in 2020; p = 0.0005) and in drug-resistant TB disease (393 ± 31 per month in 2019 versus 127 ± 32 per month in 2020; p < 0.001), despite the significant increase of telehealth activities in 2020.2 Narita et al.37 described the stories of three patients in the United States of America with TB diagnosis delays: one had risk factors for TB and had to wait a month to get chest radiography; the second was tested 13 times for SARS-CoV-2 before her TB diagnosis; and the third had a chest radiograph that revealed right-upper-lobe opacities without cavities, so TB was not considered until 2 months later when her symptoms and chest radiography got worse.37 Additionally, they interviewed 29 TB patients diagnosed in March 2020 or later: 4 reported delays in their TB diagnosis because of issues related to the pandemic, and 3 did not seek immediate care because of fear of contracting COVID-19. Overall, it seems that delays in active TB diagnosis are a result of multiple factors: patient's fear of seeking care, referral delays, the insufficient response of health and diagnostic units, and incorrect diagnoses due to the similarities between TB and COVID in terms of signs, symptoms, and chest radiography findings.38 More awareness of TB should be sought during the pandemic, and emphasis placed on active case finding and fast referral.
The use of DOT was significantly affected in both periods, even though the National Tuberculosis Program recommends its use in all patients with active disease.28 So far, not many studies have addressed the use of DOT during the pandemic. Zimmer et al.39 surveyed 845 TB stakeholders (TB patients, healthcare workers, national TB program and policy officers, TB researchers, and TB civil societies, advocates, and survivors) from Europe, Africa, Asia, and America. About 70% of healthcare workers and program and policy officers reported a reduction in TB patients receiving DOT since the pandemic. Some factors that may have contributed to these findings have already been mentioned: lockdown measures and restriction in local public transportation services, restriction of liberties, fear of COVID-19 (which was reported by 55% of all surveyed participants with active TB), and stigmatization.39 In our survey, the lack of material and human resources was the main reason for the lack of DOT use. Hiring more staff for centres struggling to use DOT is a possible solution but may not be feasible during the pandemic. Another option is the acquisition of cameras for more widespread use of Video Observed Therapy, which seems to be as effective as DOT.40
Our study has some limitations that needed to be highlighted. First, the response rate was not homogeneous across all Regional Health Administrations, which limits our comparisons between different regions. Still, we consider a 52.5% response rate to be fairly representative of the national panorama. Secondly, variables concerning the 1st State of Emergency were collected retrospectively.
Apart from this, some strengths should be highlighted. This is, as far as we know, the first national study being conducted on this theme; we achieved a significant participation rate in the regions with the highest incidence of TB and highest number of OTBC. The accuracy of findings allows us to discuss the example of Portugal in comparison with recent multi-country studies published by the Global Tuberculosis Network.
ConclusionsOverall, most OTBC's were able to follow the set of norms published by the Directorate-General of Health and maintain diagnostic, treatment, screening and prevention of TB during the pandemic, which contributed to protecting Portugal from the worse consequences of the subsequent waves of the COVD-19 pandemic. Nevertheless, attention should be given to enhance COVID-19 prevention (by encouraging anti-COVID-19 vaccination) and, specifically for TB, to reduce diagnostic delay and barriers to DOT implementation.
Authors’ contributionsIR and RD formulated the initial research questions and study methodology. IR and RD contributed to refining the research and study methodology. IR was responsible for data analysis. All authors were involved in data interpretation. IR wrote the first draft of the paper. AA, RD and GBM reviewed the document. All authors provided inputs on and approved the final version of the manuscript.


