


Pulmonary epithelioid hemangioendothelioma (PEHE) is an extremely rare, low-moderate malignant tumour of vascular origin.1 Herein, we report a rare case of malignant PEHE masquerading as lung adenocarcinoma with radiological presentations and histological manifestations.
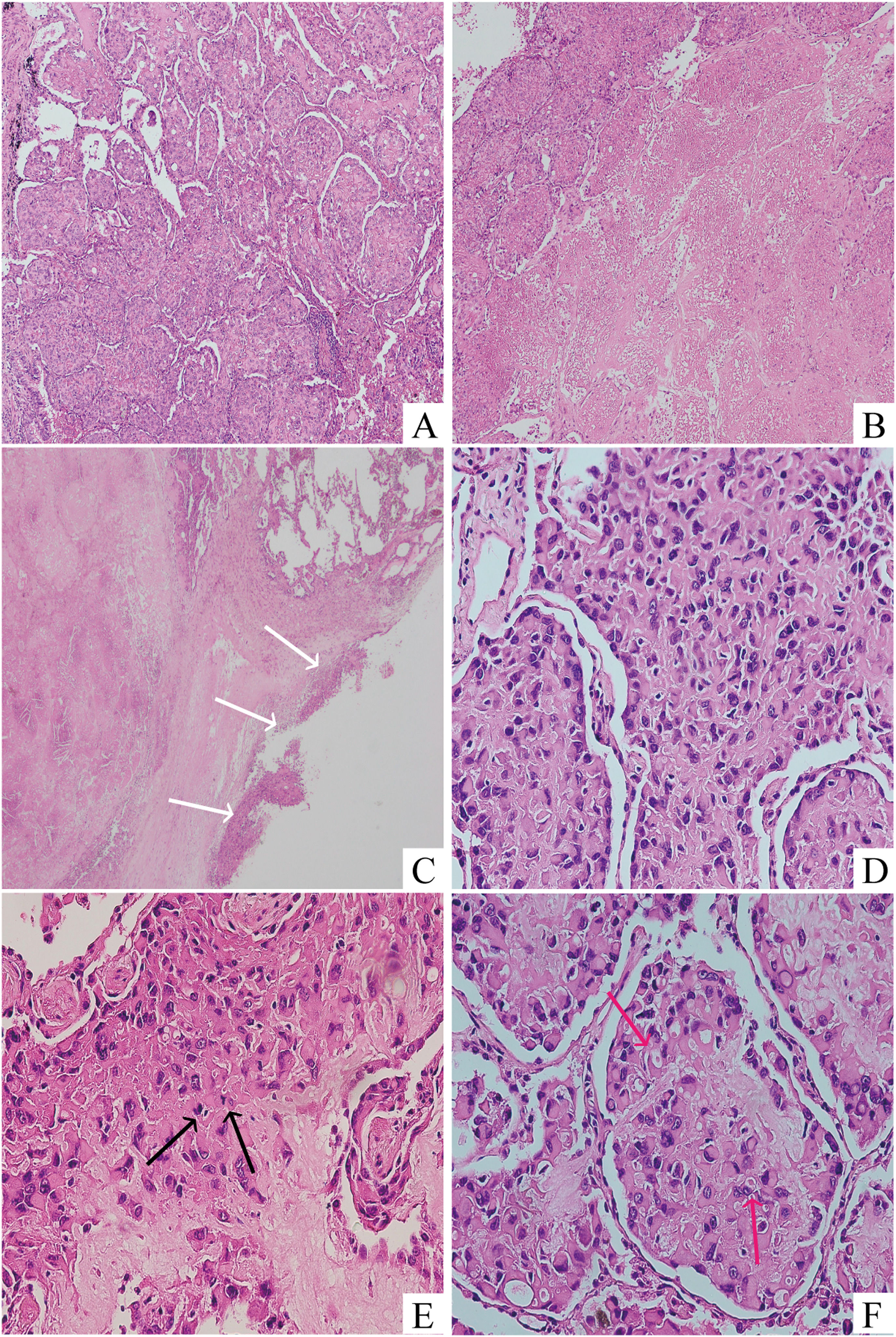
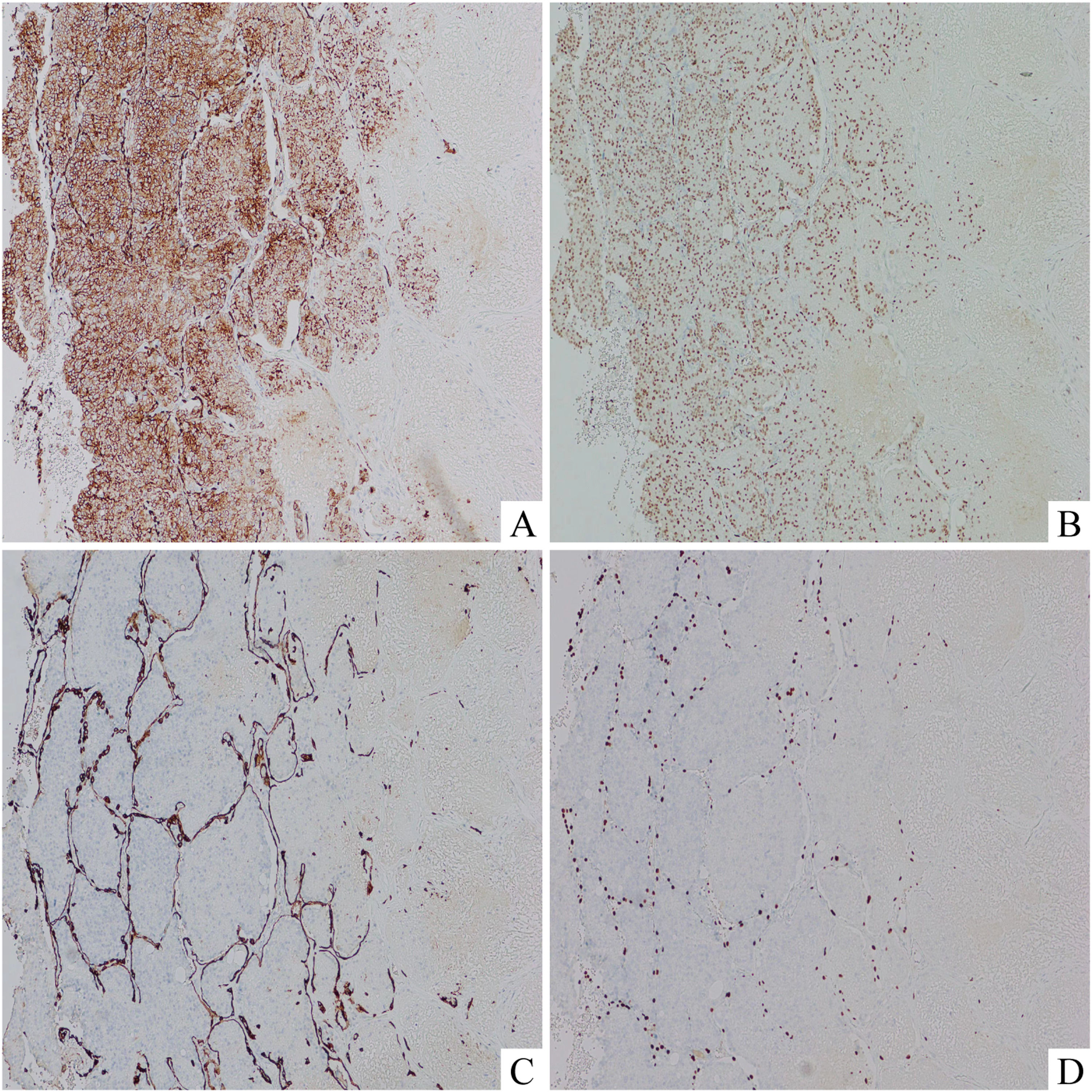
A 44-year-old female patient presented to our respiratory clinic with a pulmonary nodule detected upon physical examination. The patient had no history of smoking or lung disease. Thoracic computed tomography (CT) revealed an irregular mass in the dorsal segment of the left lung lower lobe with shallow lobulation and spiculation, measuring approximately 18 × 15 mm (Fig. 1A). The patient underwent a lobectomy, and upon intraoperative consultation, the tumour appeared greyish, medium-textured, poorly demarcated, and immediately adjacent to the pleura with pleural indentation. The mass centre was hypocellular and the peripheral areas were hypercellular (Fig. 1B), The peripheral tumour cells displayed a solid sheet growth pattern with necrosis (Fig. 1C). The neoplastic cells were eosinophilic epithelioid, with abundant cytoplasm, nuclear deviation, and clear nuclear pleomorphism (Fig. 1D). After intraoperative consultation, the condition was diagnosed as lung adenocarcinoma. Permanent section analysis showed results similar to those of the frozen sectioned material. Nevertheless, tumour cells grew primarily within the alveolar space; extensive necrosis and focal parietal pleural invasion were observed (Fig. 2A–C). Eosinophilic epithelioid tumour cells pervaded in a transparent matrix with obvious atypia and mitotic figures (Fig. 2D and E). Intracytoplasmic vacuolisation was discovered in some tumour cells, indicating primitive angiogenesis. Additionally, some of these tumour cells can be observed with intracytoplasmic lumen and erythrocyte inside, indicating their vascular nature (Fig. 2F). Immunohistochemically, diffuse neoplasm cells stained for CD34 (Fig. 3A) and ERG (Fig. 3B) were observed, whereas the keratin marker AE1/AE3 (Fig. 3C) and TTF-1 (Fig. 3D) were negative. Based on these radiological, histological and immunohistochemical findings, a diagnosis of malignant pulmonary epithelioid hemangioendothelioma was established. After surgery, the patient underwent complementary radiotherapy. No tumour recurrence or metastasis had occurred at the six-month postoperative follow-up.
 scan displayed an irregular mass with superficial lobulation and burr sign located at the dorsal segment of the left lung lower lobe (white arrow). (B) Intraoperative consultaion revealed that the centre of the nodule was hypocellular and the peripheral areas consisted of abundant tumour cells (Hematoxylin and eosin stain, 40 ×). Epithelioid tumour cells with nuclear deviation were arranged in solid sheets with (C) necrosis (Hematoxylin and eosin stain, 200 ×) (black arrow) and (D) marked atypia (Hematoxylin and eosin stain, 400 ×).")
Thoracic CT (A) scan displayed an irregular mass with superficial lobulation and burr sign located at the dorsal segment of the left lung lower lobe (white arrow). (B) Intraoperative consultaion revealed that the centre of the nodule was hypocellular and the peripheral areas consisted of abundant tumour cells (Hematoxylin and eosin stain, 40 ×). Epithelioid tumour cells with nuclear deviation were arranged in solid sheets with (C) necrosis (Hematoxylin and eosin stain, 200 ×) (black arrow) and (D) marked atypia (Hematoxylin and eosin stain, 400 ×).
 the alveolar space (Hematoxylin and eosin stain, 100 ×) with (B) significant necrosis (Hematoxylin and eosin stain, 100 ×) and (C) focal parietal pleural invasion (Hematoxylin and eosin stain, 40 ×) (white arrow). The neoplastic cells exhibited (D) marked nuclear pleomorphism (Hematoxylin and eosin stain, 400 ×) and (E) numerous mitotic figures (5 mitoses per 10 high-power fields; Hematoxylin and eosin stain, 400 ×) (black arrow). (F) Intracellular vacuolisation and intracellular erythrocytes (red arrow), which represented primitive vascular lumens, were observed (Hematoxylin and eosin stain, 400 ×).(For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)")
Histological examination of the lesion revealed the eosinophilic epithelioid tumour cells grew within (A) the alveolar space (Hematoxylin and eosin stain, 100 ×) with (B) significant necrosis (Hematoxylin and eosin stain, 100 ×) and (C) focal parietal pleural invasion (Hematoxylin and eosin stain, 40 ×) (white arrow). The neoplastic cells exhibited (D) marked nuclear pleomorphism (Hematoxylin and eosin stain, 400 ×) and (E) numerous mitotic figures (5 mitoses per 10 high-power fields; Hematoxylin and eosin stain, 400 ×) (black arrow). (F) Intracellular vacuolisation and intracellular erythrocytes (red arrow), which represented primitive vascular lumens, were observed (Hematoxylin and eosin stain, 400 ×).(For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
 and ERG (B, × 200). However, all tumour cells were negative for AE1/AE3 (C, × 200) and TTF-1 (D, × 200).")
Epithelioid hemangioendothelioma (EHE) was first described by Dail et al. in 1975 and was thought to be epithelial in origin. In 1982, Weiss and Enzinger introduced the term “epithelioid hemangioendothelioma” to describe tumours of similar vascular origin in soft tissues. The term “malignant” EHE (MEHE) is proposed for tumours with a distinctive nuclear heterogeneity, mitotic activity (>1 mitosis per 10 high-power fields (HPF)), tumour necrosis, and spindle cell component.2 Patients with PEHE are usually asymptomatic or have nonspecific respiratory symptoms. Therefore, PEHE is often detected incidentally on imaging.3 Typical radiological images of patients with PEHE show various irregular nodules with punctate calcifications. PEHE presents as a single isolated nodule or mass similar to primary lung adenocarcinoma is extremely unusual.4 PEHE needs to be differentiated from many tumours. The principal points of histological differentiation between PEHE and primary lung adenocarcinoma, apart from immunohistochemistry, are the pleomorphism of the nuclei and the prominent mitotic figures.2 However, the present case of PEHE presented radiologically as a single nodule and histologically showed significant heterogeneity, marked mitotic activity, and neoplastic necrosis, all of which resembled lung adenocarcinoma. This extremely rare condition may be a radiologic and pathological diagnostic pitfall.


