

Asthma is a chronic inflammatory disease with multiple phenotypes. There is still a major gap in the understanding of its complex causality. Obstructive sleep apnea (OSA) is a common condition that has been implicated as a risk factor for asthma exacerbations.
ObjectivesThis study aims to characterize patients with the diagnosis of asthma and suspected OSA; identify the presence of OSA and review, on the current literature, the association between asthma and OSA, as an overlap syndrome.
Materials and methodsThe authors present a retrospective study that included patients diagnosed with asthma that underwent sleep study in a 3 year period. Demographic, clinical data, body mass index (BMI), sleep study parameters and treatments were analyzed.
ResultsThe sample consisted of 47 patients. The majority of population was females (68%) and the mean age was 55.65±13.04 years. The most common nighttime symptom was snoring (93.6%). Regarding BMI, values above the normal limit were observed in 89.36% of the patients. 68% underwent polysomnography and the others cardiorespiratory polygraphy. In 57.4% of the patients, OSA was confirmed with a higher prevalence in males (73.3%) compared to females (50%). The therapeutic approach in 81.8% of these patients was home ventilation therapy.
ConclusionThe combination of asthma and OSA has become increasingly more frequent. In the described study, the prevalence of OSA was 57.4%, value that is in fact higher than in general population. After the therapeutic approach, all patients referred improvement of symptoms. It is therefore essential that OSA is investigated in patients with asthma when there is poor control of symptoms, in order to achieve a better control.
Asthma is a chronic inflammatory disease with multiple phenotypes related to genetic predisposition and various environmental interactions. There is still a major gap in the understanding of its complex causality and, consequently, in the primary prevention of the disease.1 Most patients with asthma have mild-to-moderate disease that can be easily controlled with conventional treatment. However, some have uncontrolled asthma despite moderate to high doses of inhaled corticosteroids and long acting β2 agonist and/or leukotriene modifier combinations. Factors that influence asthma control, such as environmental exposure, comorbidities, adherence, and inhalation technique, should be identified and adequately addressed.2
Quality of sleep in patients with asthma is poorer, compared to those with chronic obstructive pulmonary disease. Whereas some comorbid conditions, such as rhinitis and gastroesophageal reflux disease (GER), are well recognized to aggravate asthma, little is known about the potential role of obstructive sleep apnea.3 OSA is characterized by episodes of complete or partial upper airway obstruction during sleep. It is known that it induces intermittent hypoxemia, carbon dioxide retention and changes in hemodynamic responses during sleep.
The first study examining asthma and OSA was a case report by Hudgel and Shrucard, in 1979.4 Since then, asthma and OSA are increasingly troublesome public health issues. Mounting evidence implicates OSA as a risk factor for asthma exacerbations,5 therefore it is imperative to look further into the connection between these two entities.
ObjectiveThis study aims to characterize the patients (demographic analysis, symptoms, body mass index (BMI)) admitted in a Pulmonology Department with the diagnosis of asthma and suspected OSA. It also aims to review the existing literature on a possible association between asthma and OSA, as an overlap syndrome like the known combination “OSA and COPD”. Assess the effect of treatment of OSA on asthma symptoms was also an objective of the literature review.
Materials and methodsThe authors present a retrospective study carried out in a period of three years in an Immunoallergology Department which included patients followed in an outpatient clinic and diagnosed with asthma. During this period, patients diagnosed with asthma underwent a structured survey during the consultation, in order to ascertain symptoms suggestive of OSA, namely symptoms of daytime sleepiness, snoring, choking or gasping during sleep, recurrent awakenings, unrefreshed sleep, daytime fatigue, and impaired concentration. All patients were also evaluated using the Epworth Sleepiness Scale.
The patients who reported characteristic symptoms of OSA underwent overnight sleep study. According to the American Association of Sleep Medicine 2009 Guidelines, the patients with high risk of OSA underwent cardiorespiratory study in the absence of significant comorbidities. The remaining patients underwent polysomnography study (PSG). Patients with negative cardiorespiratory study were subsequently subjected to PSG for diagnostic confirmation.
Demographic and clinical data, BMI, sleep study parameters of the enrolled patients were gathered and analyzed using Microsoft Office Excel 2007®. Using the available data, a revision of the current literature was made, and MEDLINE and PubMed databases from 2000 to the present were searched for relevant articles regarding the association of OSA and asthma as an overlap syndrome. Particularly, articles describing pathophysiologic conditions occurring in OSA that may be linked to asthma pathogenesis were used for this review, as well as articles referring to the therapeutic approach in these patients.
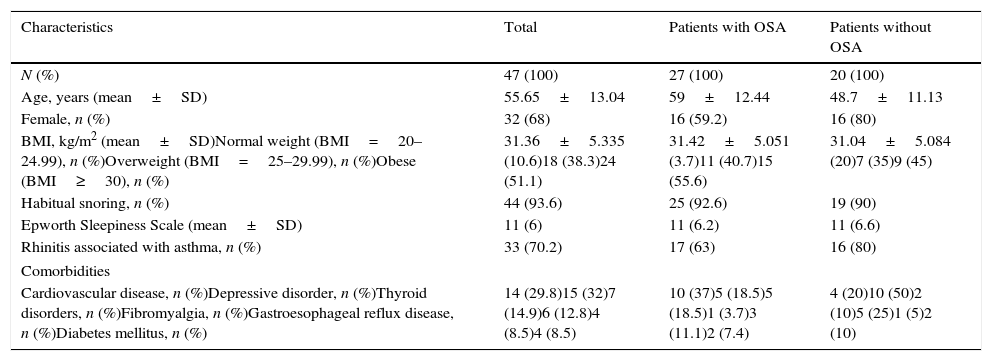
ResultsThe sample consisted of 47 patients with asthma and symptoms suggestive of OSA, with female predominance (68%). Table 1 shows some demographic and clinical characteristics of the patients divided into two groups: patients with OSA and without OSA. It was observed that patients with OSA were older than those without OSA (59 years vs 48.7 years), fact that was statistically significant (p=0.0158 with 95% confidence interval). It is also important to refer that regarding BMI, values above the normal limit were observed in 42 (89.36%) patients, 28 (87.5%) females and 14 (93.3%) males. However, in both groups, similar values of BMI were observed. In the group with OSA, 40.7% were overweight and 55.6% were obese. In the group without OSA, 35% were overweight and 45% were obese. In this group it was registered a higher number of patients with normal BMI (3.7% vs 20%).
Demographic and physiologic characteristics, smoking history and comorbidities of the enrolled patients.
| Characteristics | Total | Patients with OSA | Patients without OSA |
|---|---|---|---|
| N (%) | 47 (100) | 27 (100) | 20 (100) |
| Age, years (mean±SD) | 55.65±13.04 | 59±12.44 | 48.7±11.13 |
| Female, n (%) | 32 (68) | 16 (59.2) | 16 (80) |
| BMI, kg/m2 (mean±SD)Normal weight (BMI=20–24.99), n (%)Overweight (BMI=25–29.99), n (%)Obese (BMI≥30), n (%) | 31.36±5.335 (10.6)18 (38.3)24 (51.1) | 31.42±5.051 (3.7)11 (40.7)15 (55.6) | 31.04±5.084 (20)7 (35)9 (45) |
| Habitual snoring, n (%) | 44 (93.6) | 25 (92.6) | 19 (90) |
| Epworth Sleepiness Scale (mean±SD) | 11 (6) | 11 (6.2) | 11 (6.6) |
| Rhinitis associated with asthma, n (%) | 33 (70.2) | 17 (63) | 16 (80) |
| Comorbidities | |||
| Cardiovascular disease, n (%)Depressive disorder, n (%)Thyroid disorders, n (%)Fibromyalgia, n (%)Gastroesophageal reflux disease, n (%)Diabetes mellitus, n (%) | 14 (29.8)15 (32)7 (14.9)6 (12.8)4 (8.5)4 (8.5) | 10 (37)5 (18.5)5 (18.5)1 (3.7)3 (11.1)2 (7.4) | 4 (20)10 (50)2 (10)5 (25)1 (5)2 (10) |
All the evaluated patients reported night symptoms, the most common was snoring (93.6%) and no differences were registered between the two groups. The patients also referred choking or gasping during sleep (57.4%), excessive daytime sleepiness (EDS) (36.2%), morning headaches (29.8%) and unrefreshing sleep (19.1%). Concerning the Epworth Sleepiness Scale, 22 (46.81%) patients had a score higher than 10 and the mean value was 11.
In terms of the medication use, 21.3% of the patients only recurred to quick relief medication, such as short-acting inhaled beta-agonists. Most patients (53.2%) presented with symptoms of controlled asthma, under fixed inhaled association between long-acting beta-agonists and low-dose inhaled corticosteroids. 19.1% of the patients, needed the association of a leukotriene modifier, as well as medium or high-dose of inhaled corticosteroids. And finally the most symptomatic patients (6.4%) were under oral corticosteroids.
Regarding the lung function testes, spirometry revealed values within the normal range in 69% of the patients. In the remaining patients, an obstructive pattern was detected, according to the values of the FEV1/CVF ratio. The mean value of this parameter was 77.8% (±12.5%). The values of FEV1 varied between 35.1% and 127.8%, the mean value was 95% (±22.7%). The obstruction was considered mild in 8% of the patients, moderate in 10% and severe in 5%. CPT was normal in all patient, as expected. DLCO was determined only in 36% of the patients, and in all cases the value was within normal range.
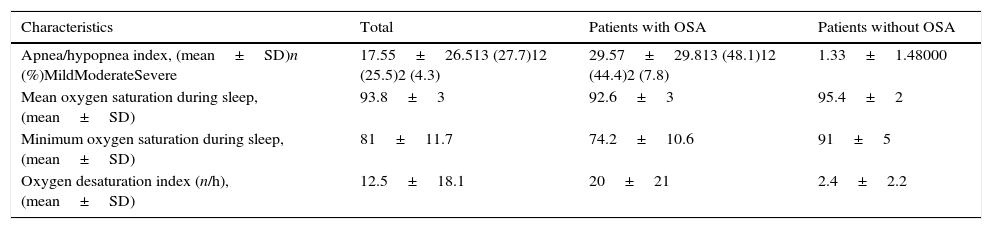
Of the 47 patients, 32 (68%) underwent overnight PSG and 15 (32%) cardiorespiratory polygraphy. In 27 (57.4%) patients it was diagnosed OSA, with higher prevalence in males (73.3%) compared to females (50%). The results of the sleep studies are shown in Table 2. As expected, the Apnea Hypopnea Index (AHI) was higher in the group of patients with OSA. The percentage of patients with mild or moderate OSA was similar and only 2 patients presented an AHI>30. The other results, expectedly, revealed lower mean and minimum oxygen saturation during sleep in the group of patients with OSA, and higher oxygen desaturation index.
Diagnostic sleep study results of the enrolled patients.
| Characteristics | Total | Patients with OSA | Patients without OSA |
|---|---|---|---|
| Apnea/hypopnea index, (mean±SD)n (%)MildModerateSevere | 17.55±26.513 (27.7)12 (25.5)2 (4.3) | 29.57±29.813 (48.1)12 (44.4)2 (7.8) | 1.33±1.48000 |
| Mean oxygen saturation during sleep, (mean±SD) | 93.8±3 | 92.6±3 | 95.4±2 |
| Minimum oxygen saturation during sleep, (mean±SD) | 81±11.7 | 74.2±10.6 | 91±5 |
| Oxygen desaturation index (n/h), (mean±SD) | 12.5±18.1 | 20±21 | 2.4±2.2 |
The therapeutic approach in most patients consisted on general sleep hygiene measures, such as weight loss, avoidance of alcohol for 4–6h prior to bedtime, positional therapies, regular hours of sleep and optimal treatment of asthma and rhinitis. Despite these measures, 22 patients initiated positive airway pressure therapy, 21 patients with continuous or automatic positive airway pressure (CPAP/APAP) and one patient with bilevel positive airway pressure (BPAP). These patients had severe, moderate or mild OSA with associated comorbidities or were quite symptomatic.
Clinical follow-up was performed 3 and 6 months after the beginning of the therapeutic measures. Interestingly, all the patients, in both groups, reported improvement of the symptoms, especially in the nighttime complaints. They also referred improvement in quality of sleep, less use of reliever medications, fewer exacerbation episodes, and improvement in neuro-cognitive complaints.
DiscussionIt is known that asthma symptoms tend to be more severe at night and that asthma-related deaths are most likely to occur during the night or early morning. Nocturnal symptoms occur in 60–74% of asthma patients and are markers of inadequate control of the disease.4 The mechanisms by which nocturnal asthma develops remain unclear and may vary from patient to patient.6 The results of our study confirm this fact and show the presence of nocturnal symptoms in all patients, whether they were diagnosed with OSA or not. In fact, 90% of patients without OSA reported frequent snoring complaints.
In this study, sleep studies showed that the prevalence of OSA in the group of investigated patients was 57.4%, which is consistent with already known fact that symptoms of sleep-disordered breathing, especially OSA, are common in asthmatic patients and are associated with asthma severity. Teodorescu et al.7 found that in a population-based prospective epidemiologic study beginning in 1988, asthma was associated with an increased risk of new-onset OSA. In this study, 22 of 81 participants (27%) with asthma experienced incident OSA over their first observed 4-year follow-up interval compared with 75 of 466 participants (16%) without asthma.
Byun et al.8 selected 167 adults with the following complaints: habitual snoring, EDS, choking during sleep, sleep fragmentation, nonrestorative sleep, daytime fatigue and difficulty concentrating. Those patients were referred for clinical evaluation and ApneaLink, and only 32 were assessed by full PSG. The prevalence of OSA depended on AHI cut-off values; AHI values of ≥5/h, ≥10/h, ≥15/h and ≥30/h corresponded to 111 (66%), 71 (42.5%), 52 (31%) and 20 (12%) patients, respectively. Of the patients who had an AHI>5 events/h, 37 (33.6%) had been diagnosed with moderate to severe asthma. They concluded that moderate to severe asthma showed strong correlations with OSA in addition to the well-known predictors of age and male gender.
In patients with asthma, OSA acts as a mechanism that contributes to the lack of asthma control,9 because the reduction in airway caliber in nocturnal asthma is often associated with sleep fragmentation, early morning awakening, difficulty maintaining sleep, and EDS. Increased abdominal pressure during periods of OSA contributes to GER, bronchial hyperreactivity, and bronchial inflammation. Patients with difficult-to-control asthma can have an increase of the number of respiratory events and oxyhemoglobin desaturation, especially during rapid eye movement sleep.4
Julien et al.10 tested the hypothesis that the prevalence and severity of OSA is greater among patients with severe compared to those with moderate asthma and controls without asthma. In this study, OSA was present in 23 of 26 (88%) patients with severe asthma, 15 of 26 (58%) patients with moderate asthma, and 8 of 26 (31%) controls without asthma. It was also verified that greater asthma severity translated to a higher value of AHI; in his study, it was reported that patients with severe asthma had a mean AHI value of 23.6 events/h, those with moderate asthma had an AHI of 19.5 events/h, and those with mild asthma had an AHI of 9.9 events/h (p<0.001). Mean nocturnal oxygen saturation was significantly lower in the patients with severe asthma than in the controls. This is also reported in our study, where mean oxygen saturation during sleep in patients with OSA was 92.6% vs 95.4% in the patients without OSA. The high prevalence of OSA in patients with severe asthma suggests that recognition and treatment of OSA plays an important role in improving asthma control.10 Teodorescu et al.11 also found that asthma patients who were using low-dose inhaled corticosteroids regularly, those who were using medium-dose inhaled corticosteroids regularly, and those who were using high-dose inhaled corticosteroids regularly were, respectively, 2.29 times, 3.67 times, and 5.43 times as likely to develop OSA as were those who were not using inhaled corticosteroids.
There are several hypotheses that can explain the interaction between OSA and asthma. Obesity is considered one of the causal factors for OSA. It has been suggested that, beyond a certain threshold of obesity, metabolic factors become involved in the pathophysiology of upper airway inflammation, as well as in bronchial hyperreactivity, interfering with the clinical manifestations of asthma.12 In the United States it is estimated that obesity may be responsible for the development of 250,000 new cases of asthma per year13 and it seems that the association between asthma and OSA worsens the clinical picture of asthma, given that OSA can stimulate weight gain. It is known that OSA interferes with lipid homeostasis and systemic inflammation and, when associated with obesity, affects glycemic regulation, interfering with insulin sensitivity, independently of the BMI.4
Peppard et al.14 evaluated adults at two different time points (at baseline and 4 years later). Initial data showed that individuals with BMI≥30kg/m2 (n=268) had an AHI of 7.4 events/h; those with 30<BMI≥25kg/m2 (n=241) had an AHI of 2.6 events/h; and those with BMI<25kg/m2 (n=181) had an AHI of 1.2 events/h. The authors found that increase in weight was positively correlated with the AHI; that is, patients who gain 10% of their body weight tend to show an increase of approximately 32% in the AHI, and a 10% reduction in weight resulted in a 26% reduction in the AHI. In our sample, values above the normal limit of the BMI were observed in 42 (89.36%) patients, 28 (87.5%) females and 14 (93.3%) males. In the group of patients with OSA, those patients with BMI≥30kg/m2 (n=15) had a mean AHI of 32.94 events/h; those with 30<BMI≥25kg/m2 (n=11) had a mean AHI of 20.53 events/h; and the one with BMI<25kg/m2 had an AHI of 6.1 events/h.
Another hypothesis refers to the relationship between OSA, asthma and systemic inflammation. It is known that OSA promotes inflammatory responses, which is demonstrated by a reversible increase in C-reactive protein (CPR). Gozal et al.15 noted that serum levels of CRP decreased proportionally to the AHI, the reduction being more significant in a group of nonobese children. OSA can cause or aggravate proinflammatory states through effects on sympathetic hyperreactivity, oxidative stress, or both.16
It is also believed that the significant increase in negative intrathoracic pressure caused by upper airway obstruction can predispose to retrograde movement of gastric contents. One study showed that 71.4% of patients with OSA had GER (as measured by pH monitoring); of those, 10.4% reported no symptoms.4 It has been reported that OSA-induced GER can play an important role in asthma symptoms. However, this association is not yet fully demonstrated. Dixon et al.13 concluded GER was not associated with any measure of asthma severity. Of common comorbidities, OSA but not GER may contribute to poor asthma control. In our sample, the prevalence of GER in the population with OSA was of 11.1%. However, no statistically significant relationship was establish with the control of asthma or the severity of OSA, due to the small number of patients.
Appropriate and adequate medical treatment should be the first step for asthmatic patients with nighttime symptoms. But they may continue in some patients, against optimal medical treatment. In this condition, other factors responsible for the symptoms should be investigated. Ciftci et al.17 showed the improvement of nocturnal asthma symptoms with CPAP. In this study, 2 months of CPAP treatment improved significantly nighttime symptoms. These findings suggest that OSA might be the responsible. Alkhalil et al.5 describe potential mechanisms whereby CPAP, the first line of therapy for OSA, might modify airway smooth muscle function and asthma control in patients with both disorders. They concluded that use of CPAP can decrease exacerbations, improve quality of life, and reduce the number of cases of difficult-to-control asthma. In our sample, 22 patients initiated positive airway pressure and reported improvement of the nighttime symptoms. The remaining patients also reported symptomatic improvement in response to the measures implemented and subsequently reinforced during follow-up. These included optimal control of asthma and rhinitis, and the usual sleep hygiene measures for snoring, referred above. Despite the ever-increasing population of patients with both disorders, large, prospective, randomized controlled studies are necessary to more fully evaluate CPAP and asthma outcomes.17
In conclusion, although the association between OSA and asthma is common, it is poorly investigated. If untreated, OSA can contribute to the lack of control of asthma, especially nocturnal asthma symptoms. It is important to evaluate the presence of symptoms of OSA in patients presenting with nocturnal asthma, because treatment with CPAP may lead to a substantial clinical improvement. Snoring in patients with asthma raise clinical suspicion of OSA. However, EDS resulting from nocturnal asthma symptoms is also an important sign of OSA.
In our study, there was no difference in symptoms of EDS and snoring in the two groups, therefore, the critical symptoms of OSA were not enough to predict the diagnosis in these patients. Given the high prevalence of OSA in the asthma population, it is important to reinforce that sleep studies should be used to document OSA and are helpful in prescribing proper treatment to achieve a better control of the disease.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.


