


Cartwright in 1984 defined positional obstructive sleep apnea (OSA) patients as those in whom the apnea-hypopnea index (AHI) was at least twice as high while sleeping in the supine as in the non-supine position. Several authors intended, since then, to propose better classification systems, but the first (and simplest) is still used nowadays.1 In general, the prevalence of positional variant is higher in mild to moderate OSA, where it can reach 65–69%, but varies from 9 to 69%. It is inversely correlated to OSA severity, body mass index (BMI) and age. This classification intended to better identify whose patients did not require ventilatory support and could be treated with positional therapy (PT), a more economical and practical treatment. Traditionally, it has been used a tennis ball inside a pocket sewed in the back of a nightshirt as the positional “device”.2 Nevertheless, ineffectiveness, backache, discomfort and no improvement in sleep quality or daytime alertness have been responsible for poor compliance and subsequent disappointing long-term results of positional therapy.
With this in mind, we carried out a study to determine the effectiveness of usual conservative measures and PT with tennis ball technique (TBT) and to verify the compliance to this therapy in our population.
A total of 93 positional OSA patients were retrospectively identified after a cardiorespiratory sleep study with 7 channels in our center, in which the supine AHI was at least twice as high as in a non-supine position. Booklets were provided to patients with information on hygiene, dietary and sleep rules, snoring and TBT. These patients were reassessed in a follow-up visit in average in 3–6 months, and a follow-up sleep study was then performed, under positional therapy with TBT. Sleep related parameters, subject's characteristics and Epworth Sleepiness Scale (ESS) were evaluated.
Forty six (49.5%) patients performed the follow-up night study with the TBT. There were 36 men (78.3%), with average age of 54,8 years and mean BMI of 29.3kg/m2. Of these 46 patients, only 26 (56.5%) said to correctly use the tennis ball every or almost every night, considered as high adherence patients group. We found differences between the two groups of patients (high and low adherence). They did not significantly differ in parameters such as age, gender, or BMI, however, the low adherence patients had more comorbidities: higher prevalence of diabetes mellitus and ischemic vascular disease (Table 1). Results of the follow-up study showed an improvement in all parameters, with mean total AHI decrease from 15.0/h to 9.3/h and mean supine AHI from 34.2/h to 24.3/h. Time spent in supine position fell from 40% to 17.1%, oxygen desaturation index (ODI) from 14.8/h to 8.8/h and minimum SpO2 increased from 82.2% to 85.6% (Table 2). More than half of the non-compliant patients (n=11; 55%) needed other therapeutic options, mainly continuous positive airway pressure (CPAP) (n=10). Only 2 compliant patients needed other therapies (1 CPAP and 1 mandibular advancement device).
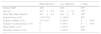
Patients demographic and clinical characteristics related to therapeutic adherence.
| High adherence | Low adherence | p value | |
|---|---|---|---|
| Gender (M/F) | 20/6 | 16/4 | NSa |
| Age (yr) | 56.5±9.4 | 56.1±9.1 | NSb |
| Body Mass Index (Kg/m2) | 28.5±3.8 | 30.2±4.7 | NSb |
| Hypertension, n (%) | 15 (57.7%) | 13 (65%) | NSa |
| Diabetes mellitus, n (%) | 3 (11.5%) | 6 (30%) | P<0.05a |
| Ischemic vascular disease, n (%) | 0 | 4 (20%) | P<0.05a |
| Heart Failure, n (%) | 0 | 2 (10%) | NSa |
| Oncologic disease, n (%) | 0 | 2 (10%) | NSa |
Sleep respiratory variables in baseline and follow-up study.
| Baseline study | Follow-up study | p value | |
|---|---|---|---|
| Epworth sleepiness scale | 11.0±3.6 | 7.9±3.6 | <0.001a |
| Total AHI (events/h) | 15.0±7.6 | 9.3±7.0 | <0.001a |
| Supine AHI (events/h) | 34.2±18.8 | 24.3±19.4 | <0.01a |
| Supine time (%) | 40.0±15.5 | 17.1±14.1 | <0.001a |
| Oxygen desaturation index (events/h) | 14.8±6.6 | 8.8±6.8 | <0.001a |
| Minimal SpO2 | 82.2±5.1 | 85.8±3.7 | <0.001a |
| Mean SpO2 | 93.7±1.6 | 94.2±1.5 | <0.01a |
In our results, PT and other conservative measures were effective, with good clinical outcomes when enforced. There was a significant decrease in sleepiness accessed by ESS, and improvement in the overall sleep respiratory parameters. However, there is a high level of noncompliance with 20 patients (43.5%) reporting low adherence. Nevertheless, these results (56.5% of compliance) seem better than other studies. Oksenberg et al., reported only 38% of compliance with TBT at six months.3 The compliant patients in that study were older, and the main reason for stopping was discomfort. Our results showed no differences in age, but we found non-compliant patients to have more comorbidities and more severe illnesses, as oncologic and cardiovascular diseases. These patients may underestimate the burden of OSA, considering it as a minor health problem. Just half of the low adherent patients accepted CPAP therapy.
Results in long-term tend to be even worse, as demonstrated by Bignold et al., with only 6% of patients still using the TBT after 2.5 years.4 As so, currently, several new devices to replace the TBT are becoming available on the international market.5 However the efficacy of these modalities has not been studied in clinical trials on long-term or been patented.
Our study has some limitations. Data on TBT compliance and patients division in adherence groups was accessed only in a subjective way (interview in follow-up visit). Validated questionnaires on these topics could have been used in a prospective study. Unfortunately, we could not infer why 47 patients did not attend the follow-up study, however most of them attended to the follow-up visit reporting good results with the recommended measures. We can speculate they were relieved by knowing their OSA was not severe, and, at least, changed their lifestyle, not feeling the need for further examination.
In conclusion, despite our relatively small sample, we can infer that TBT is a simple, cheap and an effective form of PT when used in selected patients with clear positional OSA, as shown by good disease control in our adherent patients. Compliance remains an issue, even with the development of new devices.
Conflicts of interestThe authors have no conflicts of interest to declare.


