

As delayed intubation may worsen the outcome of coronavirus disease 2019 (COVID-19) patients treated with continuous positive airway pressure (CPAP), we sought to determine COVID-specific early predictors of CPAP failure.
MethodsIn this observational retrospective multicentre study, we included all COVID-19 patients treated with out-of-ICU CPAP, candidates for intubation in case of CPAP failure. From these patients, we collected demographic and clinical data.
ResultsA total of 397 COVID-19 patients were treated with CPAP for respiratory failure, with the therapeutic goal of providing intubation in case of CPAP failure. Univariable analysis showed that, age, lactate dehydrogenase (LDH) and white cell counts were all significantly lower in patients with successful CPAP treatment compared to those failing it and undergoing subsequent intubation. The percentage changes between baseline and CPAP application in the ratio of partial pressure arterial oxygen (PaO2) and fraction of inspired oxygen (FiO2), PaO2, respiratory rate and ROX index were higher in patients experiencing successful CPAP compared to those failing it. FiO2 and male gender were also significantly associated with intubation. Multivariable analysis adjusting for age, gender, Charlson comorbidity index, percentage change in PaO2/FiO2 or PaO2 and FiO2 separately, lactate, white blood cell count, LDH and C-reactive protein levels led to an area under the curve of 0.818 and confirmed that age, LDH and percentage increase in PaO2/FiO2 are predictors of intubation.
ConclusionsIn COVID-19 patients requiring CPAP, age, LDH and percentage change in PaO2/FiO2 after starting CPAP are predictors of intubation.
The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can cause a different spectrum of illnesses, ranging from asymptomatic infection to atypical acute respiratory distress syndrome in 4–16% of cases.1,2 When hypoxemic acute respiratory failure (ARF) occurs, supplemental oxygen is the first-line medication. For ARF patients developing hypoxemia despite receiving conventional oxygen therapy, with no indications for invasive mechanical ventilation (IMV), international guidelines recommend the use of high flow nasal cannula (HFNC) instead of conventional oxygen therapy or noninvasive positive pressure ventilation (NPPV).3 If HFNC is not available and there is no urgent indication for endotracheal intubation, current guidelines recommend a trial of NPPV with close monitoring and short-interval assessment for deterioration, even though this procedure is supported by very low-quality evidence.3 Furthermore, in acute respiratory distress syndrome (ARDS) patients, the effectiveness of noninvasive continuous positive airway pressure (CPAP) remains largely undocumented.
The Italian Respiratory Society (SIP/IRS) and the Italian Thoracic Society (AIPO-ITS) have recently issued a clinical management algorithm for the treatment of COVID-19 patients requiring oxygen escalation through helmet CPAP. More recently, a multicentre observational study has shown that CPAP along with HFNC and NPPV can be readily applied outside of the ICU environment during COVID-19.4 However, intubation after CPAP failure has been shown to occur in 22–25%5 of patients, and other studies on noninvasive ventilation have reported that delayed intubation might worsen patient survival.6 For this reason, the use of CPAP in COVID-19 patients is still under debate. Hence, the identification of early predictors of CPAP failure represents an urgent unmet clinical need.
In the present study, we identify for the first time early factors associated with intubation in COVID-19 patients treated with CPAP out-of-ICU and candidate for intubation in case of CPAP failure. This information may help clinical decision making in these challenging pandemic times.
MethodsStudy designThe present study is a large multicentre, retrospective observational study performed from March 1st to April 15th, 2020, in six hospitals of Eastern Piedmont in Northern Italy. The participating hospitals were the following: “Maggiore della Carità”, Novara, “SS. Antonio Biagio e Cesare Arrigo”, Alessandria, “S. Andrea”, Vercelli, “VCO ASL”, Domodossola, “Nuovo Ospedale degli Infermi”, Biella. The study was performed in accordance with the Declaration of Helsinki. The Ethics Committee approval was obtained for all the participating centres (CE 87/20, CE 112/20, CE 111/20, CE 110/20, ASO.RianGen.20.02, AslVC.RianGen.20.01).
Patient enrolment and data collectionPatients who met the following inclusion criteria were included in the study: 1) age ≥18 years; 2) hypoxemic ARF due to COVID-19 requiring out-of-ICU CPAP—i.e., respiratory distress despite Venturi mask oxygen therapy and partial pressure of oxygen to inspiratory oxygen fraction below 200 mmHg; 3) full treatment therapeutic goal—i.e., patients scheduled to receive intubation in the case of CPAP failure.
Exclusion criteria were: 1) intubation on the same day as that of CPAP initiation; 2) CPAP administered as prophylactic treatment after extubation, 3) do-not-intubate order, i.e., when CPAP was ceiling of treatment.
The therapeutic goal of CPAP was collegially discussed in various multidisciplinary team meetings together with the patients and their families, taking into account comorbidities,7 quality of life and patient preferences.
For all enrolled patients, we collected demographic characteristics and blood sample exams performed on admission—i.e., white blood cell count, lymphocytes count, creatinine, alanine transaminase, aspartate transaminase, lactate dehydrogenase (LDH), C-reactive protein, D-dimer, ferritin. We also recorded the values of arterial blood gas (ABG), respiratory rate and inspiratory oxygen fraction (FiO2) delivered by a Venturi mask before and after 2–24 h of CPAP application. The ABG percentage change (Δ%) was calculated as follows: (parameter during CPAP - parameter during Venturi mask / parameter during Venturi mask) * 100. Charlson comorbidity index (CCI)8 was computed on the first day of hospital admission. Intubation was defined as CPAP failure. The drugs administered during the hospital stay have been also registered.
Continuous positive airway pressure (CPAP) settingsAs previously described,6 CPAP was delivered through helmets (Intersurgical, Mirandola (MO), Italy; Dimar, Medolla, MO, Italy) through flowmeter (60−70 L/min) and face masks (Intersurgical, Mirandola, MO, Italy; Dimar, Medolla, MO, Italy; Fisher&Paykel, Auckland, New Zealand; ResMed, San Diego, CA, USA; Philips Respironics, Murrysville, PA, USA) via flowmeters or Boussignac systems (typically 30−70 L/min). FiO2 was set by regulating oxygen and air flow. Anti-bacterial/viral filters were applied to the expiratory port. CPAP was started in all patients with respiratory distress despite oxygen therapy by Venturi mask up to FiO2 50% and a partial pressure of oxygen to inspiratory oxygen fraction below 200 mmHg, not necessitating immediate endotracheal intubation. Initial CPAP setting was between 10 and 12 cmH2O, thereafter, CPAP pressure could be increased up to 15 cmH2O or decreased, according to patient’s needs, tolerance and any side-effects. PEEP and FiO2 were set to obtain a SpO2 between 92−96%, or 88–92% if the patient suffered of chronic pulmonary obstructive disease or severe restrictive diseases, as suggested by the Italian respiratory societies. CPAP was delivered on an as-needed basis. When respiratory parameters improved, CPAP support was gradually reduced with a progressive increase of CPAP time off until full discontinuation.
Respiratory intermediate care unit organizationAs previously described,6 respiratory intermediate care units were organized as follows. The nurse-to-patient ratio varied from a maximum of 1:6 both during day and night to a minimum of 1:8 and 1:12 during day and night, respectively. In three hospitals, the medical staff was mixed, including internists, pneumologists, emergency physicians, cardiologists and ICU physicians, while in the other three hospitals the medical team was the same as before COVID-19 pandemic, i.e., internists. CPAP was predominantly prescribed by the anaesthesiologists involved in the COVID-19 ward team, and less commonly by pneumologists and emergency physicians, or by consulting ICU physicians. Most of the physicians were already trained for CPAP use; those who were not received a specific rapid ad-hoc training. Ward monitoring included SpO2, non-invasive blood pressure and ECG, applied continuously or at a defined time points depending on the severity of the patient. Blood gas analysis was performed when clinically relevant. Patients received daily visits from the consulting physician who prescribed CPAP if not continuously involved in the team.
Criteria for intubationPhysicians from the six ICU involved in the present study, stated they agreed and followed the criteria for intubation9,10i.e., cardiac or respiratory arrest; inability to protect the airway; coma or psychomotor agitation; unmanageable secretions or uncontrolled vomiting; life-threatening arrhythmias or electrocardiographic signs of ischemia; hemodynamic instability defined as systolic arterial pressure <90 mmHg despite adequate filling or use of vasoactive agents; intolerance to all interfaces; dyspnea during CPAP, respiratory rate >30 breaths/min; peripheral oxygen saturation (SpO2) below 92% during CPAP despite 60% FiO2 and acidosis with a pH < 7.35.
Statistical analysisDescriptive statistics were used to summarize the main demographic characteristics, and the results of laboratory findings of all patients were included in the study. Categorical variables were reported as absolute frequencies and percentages, while numerical variables were given as median and interquartile range (IQR). Univariable and multivariable Poisson regression model with robust standard error were performed to calculate the relative risks (RR) and the corresponding 95% confidence intervals (95% CI) of the association between the results of laboratory findings, clinical parameters, Δ% of the ABG values and risk of intubation. Given the high correlation between the Δ% of some ABG parameters, several multivariable models were performed to separately evaluate the role of these variables. The other variables (i.e., age, gender, CCI, LDH, C-reactive protein, white blood cell and lymphocyte count) were included in all models. Estimates were further adjusted by study center. The C-index was used to assess the predictive ability of the multivariable models and its 95% CI based on 150 bootstrap samples was calculated as well. A secondary analysis was performed on the ABG values obtained during Venturi mask oxygen therapy and CPAP.
All hypothesis tests were two-tailed and a P-value of 0.05 was considered statistically significant. Statistical analysis was performed using SAS (version 9.4; SAS Institute Cary, NC, USA).
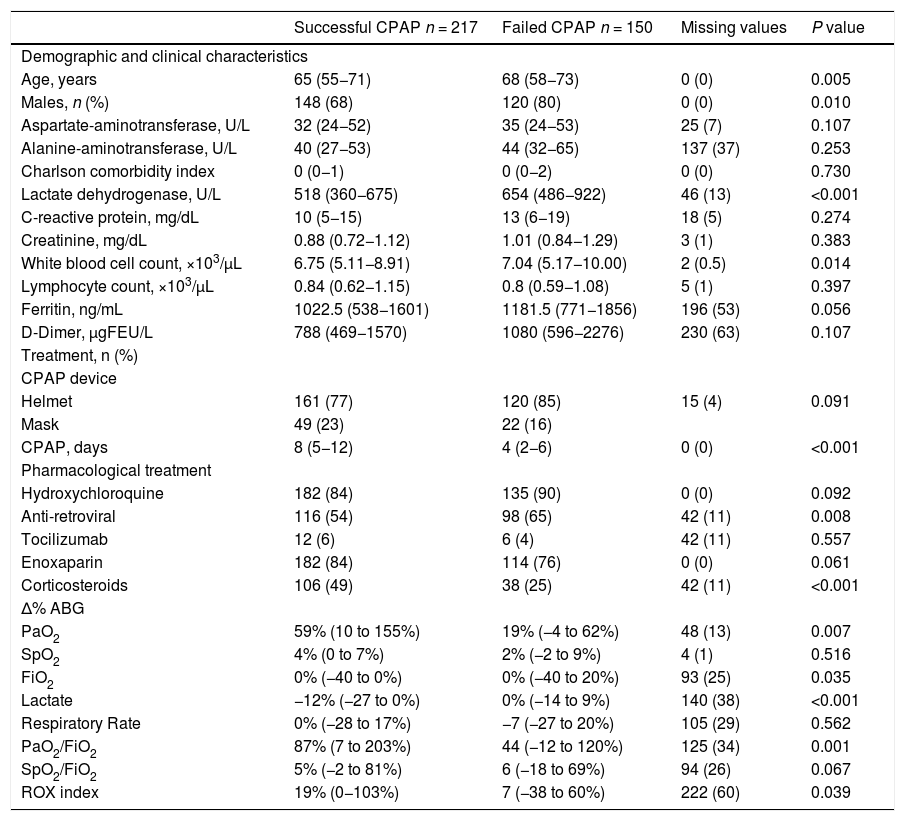
ResultsFrom March 1st to April 15th, 2020, a total of 397 patients were enrolled in the study. Of these, 30 (7.6%) patients were excluded from the study as they had been intubated on the same day as that of CPAP initiation. Two-hundred-seventeen patients were successfully treated with CPAP, while 150 patients failed CPAP and were thus subjected to endotracheal intubation. Table 1 shows the distribution of demographic and clinical characteristics of the patients stratified by “successful CPAP” or “failed CPAP” as well as the P-value derived from the univariable models. Table 1 s shows the same data stratified by centre. Among demographic and clinical patients’ characteristics, age (65 vs. 68 years, P = 0.005), gender (male 68% vs. 80%, P = 0.010), LDH (518 vs. 654 U/L, P < 0.001) and white blood cells (6.75 vs. 7.04 × 103/µL, P = 0.01) resulted significantly different between successful and failed CPAP. Helmet was applied in 77% and 85% of CPAP successes and failures, respectively. Fifteen patients received CPAP trough both helmet and mask. CPAP duration was significantly different among CPAP successes and failures (8 vs. 4 days, P < 0.0001). Most patients received hydroxychloroquine and prophylactic enoxaparin. Noteworthy, steroids were administered more frequently in the CPAP success group (49% vs. 25%, P < 0.0001).
Characteristics and variation of arterial blood gas parameters in patients with successful or failed CPAP.
| Successful CPAP n = 217 | Failed CPAP n = 150 | Missing values | P value | |
|---|---|---|---|---|
| Demographic and clinical characteristics | ||||
| Age, years | 65 (55−71) | 68 (58−73) | 0 (0) | 0.005 |
| Males, n (%) | 148 (68) | 120 (80) | 0 (0) | 0.010 |
| Aspartate-aminotransferase, U/L | 32 (24−52) | 35 (24−53) | 25 (7) | 0.107 |
| Alanine-aminotransferase, U/L | 40 (27−53) | 44 (32−65) | 137 (37) | 0.253 |
| Charlson comorbidity index | 0 (0−1) | 0 (0−2) | 0 (0) | 0.730 |
| Lactate dehydrogenase, U/L | 518 (360−675) | 654 (486−922) | 46 (13) | <0.001 |
| C-reactive protein, mg/dL | 10 (5−15) | 13 (6−19) | 18 (5) | 0.274 |
| Creatinine, mg/dL | 0.88 (0.72−1.12) | 1.01 (0.84−1.29) | 3 (1) | 0.383 |
| White blood cell count, ×103/µL | 6.75 (5.11−8.91) | 7.04 (5.17−10.00) | 2 (0.5) | 0.014 |
| Lymphocyte count, ×103/µL | 0.84 (0.62−1.15) | 0.8 (0.59−1.08) | 5 (1) | 0.397 |
| Ferritin, ng/mL | 1022.5 (538−1601) | 1181.5 (771−1856) | 196 (53) | 0.056 |
| D-Dimer, μgFEU/L | 788 (469−1570) | 1080 (596−2276) | 230 (63) | 0.107 |
| Treatment, n (%) | ||||
| CPAP device | ||||
| Helmet | 161 (77) | 120 (85) | 15 (4) | 0.091 |
| Mask | 49 (23) | 22 (16) | ||
| CPAP, days | 8 (5−12) | 4 (2−6) | 0 (0) | <0.001 |
| Pharmacological treatment | ||||
| Hydroxychloroquine | 182 (84) | 135 (90) | 0 (0) | 0.092 |
| Anti-retroviral | 116 (54) | 98 (65) | 42 (11) | 0.008 |
| Tocilizumab | 12 (6) | 6 (4) | 42 (11) | 0.557 |
| Enoxaparin | 182 (84) | 114 (76) | 0 (0) | 0.061 |
| Corticosteroids | 106 (49) | 38 (25) | 42 (11) | <0.001 |
| Δ% ABG | ||||
| PaO2 | 59% (10 to 155%) | 19% (−4 to 62%) | 48 (13) | 0.007 |
| SpO2 | 4% (0 to 7%) | 2% (−2 to 9%) | 4 (1) | 0.516 |
| FiO2 | 0% (−40 to 0%) | 0% (−40 to 20%) | 93 (25) | 0.035 |
| Lactate | −12% (−27 to 0%) | 0% (−14 to 9%) | 140 (38) | <0.001 |
| Respiratory Rate | 0% (−28 to 17%) | −7 (−27 to 20%) | 105 (29) | 0.562 |
| PaO2/FiO2 | 87% (7 to 203%) | 44 (−12 to 120%) | 125 (34) | 0.001 |
| SpO2/FiO2 | 5% (−2 to 81%) | 6 (−18 to 69%) | 94 (26) | 0.067 |
| ROX index | 19% (0−103%) | 7 (−38 to 60%) | 222 (60) | 0.039 |
Values are reported as median (interquartile range) or number (percentage).
CPAP continuous positive airway pressure, FEU fibrinogen-equivalent unit, n number, ABG arterial blood gas, PaO2 partial pressure of oxygen, SpO2 oxygen saturation, FiO2 inspired oxygen fraction.
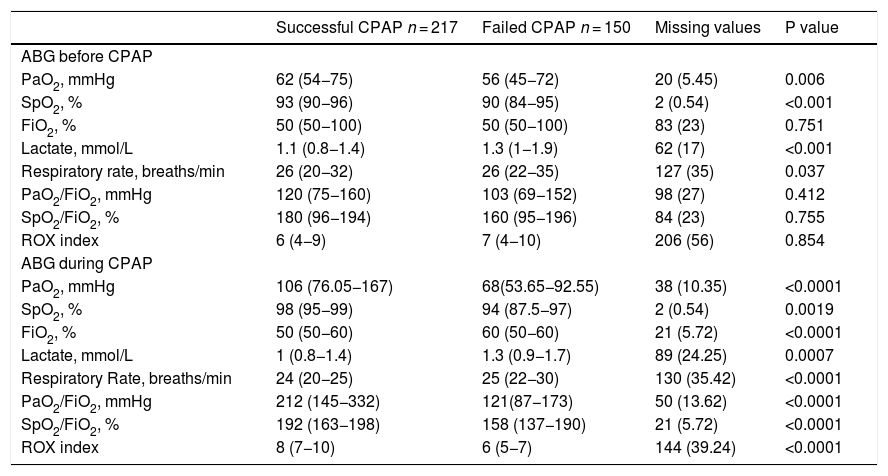
Among respiratory variables, ΔPaO2 (59% vs. 19%, P = 0.007), ΔFiO2 (0% vs. 0%, P = 0.035), Δlactate (-12% vs. 0%, P < 0.001), ΔPaO2/FiO2 (87 vs. 44%, P = 0.001), ΔROX index (19 vs.7%, P = 0.039), resulted significantly different between CPAP success and failure. Table 2 reports ABG values obtained during Venturi mask oxygen therapy prior to CPAP initiation and those obtained at 2–24 h after CPAP, while Table 2s reports ABG values stratified by centres.
Detailed arterial blood gas parameters before and during CPAP in patients stratified by successful CPAP.
| Successful CPAP n = 217 | Failed CPAP n = 150 | Missing values | P value | |
|---|---|---|---|---|
| ABG before CPAP | ||||
| PaO2, mmHg | 62 (54−75) | 56 (45−72) | 20 (5.45) | 0.006 |
| SpO2, % | 93 (90−96) | 90 (84−95) | 2 (0.54) | <0.001 |
| FiO2, % | 50 (50−100) | 50 (50−100) | 83 (23) | 0.751 |
| Lactate, mmol/L | 1.1 (0.8−1.4) | 1.3 (1−1.9) | 62 (17) | <0.001 |
| Respiratory rate, breaths/min | 26 (20−32) | 26 (22−35) | 127 (35) | 0.037 |
| PaO2/FiO2, mmHg | 120 (75−160) | 103 (69−152) | 98 (27) | 0.412 |
| SpO2/FiO2, % | 180 (96−194) | 160 (95−196) | 84 (23) | 0.755 |
| ROX index | 6 (4−9) | 7 (4−10) | 206 (56) | 0.854 |
| ABG during CPAP | ||||
| PaO2, mmHg | 106 (76.05−167) | 68(53.65−92.55) | 38 (10.35) | <0.0001 |
| SpO2, % | 98 (95−99) | 94 (87.5−97) | 2 (0.54) | 0.0019 |
| FiO2, % | 50 (50−60) | 60 (50−60) | 21 (5.72) | <0.0001 |
| Lactate, mmol/L | 1 (0.8−1.4) | 1.3 (0.9−1.7) | 89 (24.25) | 0.0007 |
| Respiratory Rate, breaths/min | 24 (20−25) | 25 (22−30) | 130 (35.42) | <0.0001 |
| PaO2/FiO2, mmHg | 212 (145−332) | 121(87−173) | 50 (13.62) | <0.0001 |
| SpO2/FiO2, % | 192 (163−198) | 158 (137−190) | 21 (5.72) | <0.0001 |
| ROX index | 8 (7−10) | 6 (5−7) | 144 (39.24) | <0.0001 |
Values are reported as median (interquartile range) or number (percentage).
CPAP continuous positive airway pressure, ABG arterial blood gas, n number, PaO2 partial pressure of oxygen, SpO2 oxygen saturation, FiO2 inspired oxygen fraction.
The values of PaO2, SpO2, lactate and RR, recorded during Venturi mask oxygen therapy, as well as those of PaO2, SpO2, FiO2, lactate, RR, PaO2/FiO2 and SpO2/FiO2, measured during CPAP, resulted significantly associated with CPAP failure.
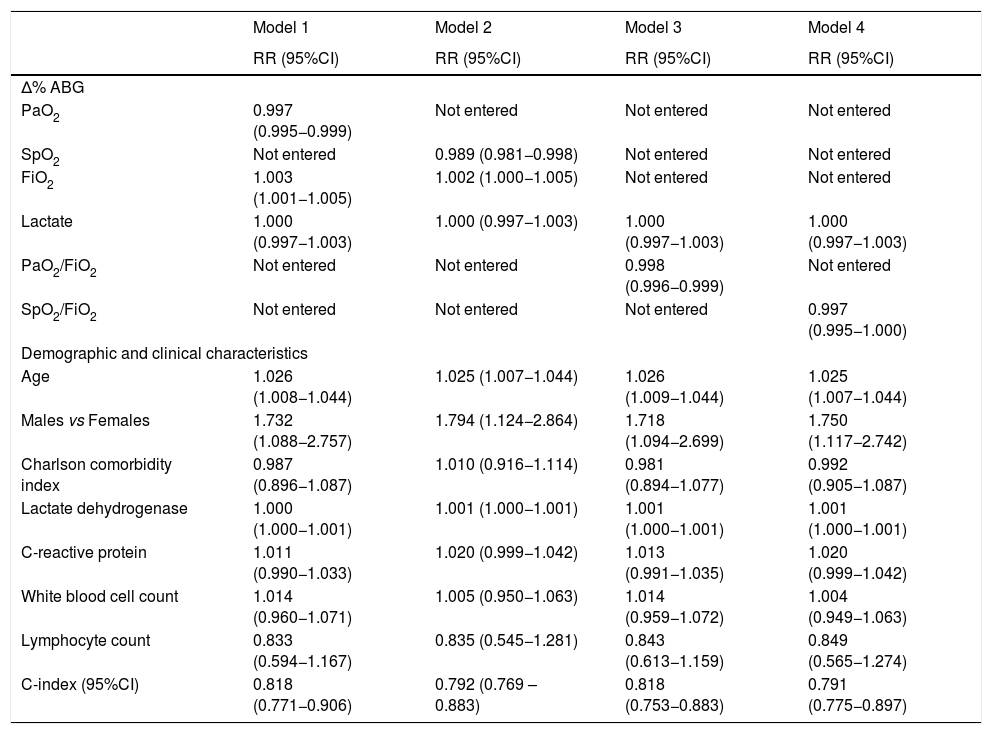
Multivariable analysis of both clinical data on admission and the Δ% ABG values between Venturi mask and CPAP, allowed us to develop 4 models (Table 3). The best models were those obtained by adjusting for age, gender, CCI, white blood cell and lymphocyte count, LDH and C-reactive protein levels, Δlactate and either ΔPaO2/FiO2 or ΔPaO2 and ΔFiO2, separately, both leading to an area under the curve of 0.818.
Results from multivariable analysis according to different models.
| Model 1 | Model 2 | Model 3 | Model 4 | |
|---|---|---|---|---|
| RR (95%CI) | RR (95%CI) | RR (95%CI) | RR (95%CI) | |
| Δ% ABG | ||||
| PaO2 | 0.997 (0.995−0.999) | Not entered | Not entered | Not entered |
| SpO2 | Not entered | 0.989 (0.981−0.998) | Not entered | Not entered |
| FiO2 | 1.003 (1.001−1.005) | 1.002 (1.000−1.005) | Not entered | Not entered |
| Lactate | 1.000 (0.997−1.003) | 1.000 (0.997−1.003) | 1.000 (0.997−1.003) | 1.000 (0.997−1.003) |
| PaO2/FiO2 | Not entered | Not entered | 0.998 (0.996−0.999) | Not entered |
| SpO2/FiO2 | Not entered | Not entered | Not entered | 0.997 (0.995−1.000) |
| Demographic and clinical characteristics | ||||
| Age | 1.026 (1.008−1.044) | 1.025 (1.007−1.044) | 1.026 (1.009−1.044) | 1.025 (1.007−1.044) |
| Males vs Females | 1.732 (1.088−2.757) | 1.794 (1.124−2.864) | 1.718 (1.094−2.699) | 1.750 (1.117−2.742) |
| Charlson comorbidity index | 0.987 (0.896−1.087) | 1.010 (0.916−1.114) | 0.981 (0.894−1.077) | 0.992 (0.905−1.087) |
| Lactate dehydrogenase | 1.000 (1.000−1.001) | 1.001 (1.000−1.001) | 1.001 (1.000−1.001) | 1.001 (1.000−1.001) |
| C-reactive protein | 1.011 (0.990−1.033) | 1.020 (0.999−1.042) | 1.013 (0.991−1.035) | 1.020 (0.999−1.042) |
| White blood cell count | 1.014 (0.960−1.071) | 1.005 (0.950−1.063) | 1.014 (0.959−1.072) | 1.004 (0.949−1.063) |
| Lymphocyte count | 0.833 (0.594−1.167) | 0.835 (0.545−1.281) | 0.843 (0.613−1.159) | 0.849 (0.565−1.274) |
| C-index (95%CI) | 0.818 (0.771−0.906) | 0.792 (0.769 – 0.883) | 0.818 (0.753−0.883) | 0.791 (0.775−0.897) |
ABG arterial blood gas, PaO2 partial pressure of oxygen, SpO2 oxygen saturation, FiO2 inspired oxygen fraction, RR relative risk, CI confidence interval. All models are adjusted by centre.
From the model analysis, we found that age (RR, 1.026; 95% CI, 1.009−1.044, model 3), gender (RR, 1.718; 95% CI, 1.094−2.699, model 3), LDH (RR, 1.001; 95%CI, 1.000−1.001, model 3), and PaO2/FiO2 (RR, 0.998; 95%CI, 0.996−0.999, model 3), were independent predictors of intubation.
DiscussionOur study, comprising 367 COVID-19 positive patients treated with out-of-ICU CPAP due to hypoxemic ARF and candidate to intubation in case of CPAP failure, shows that gender, LDH on admission and percentage of increase in PaO2/FiO2 between Venturi mask and CPAP are independent predictors of CPAP failure once corrected for the major clinical variablesi.e., age, CCI, white blood cell and lymphocyte count and C-reactive protein levels on admission.
A number of investigations seeking to find relevant outcome predictors among hospitalized patients with COVID-19 have shown that, on admission, increased D-dimer concentration11 and neutrophil-to-lymphocyte ratio12 as well as enhanced levels of C-reactive protein,13 creatinine13 and cardiac troponin I14 are all associated with a higher risk of intubation. Similarly, a body mass index (BMI) ≥35 kg/m,15 increasing age,15 male sex,15 comorbid status,13 respiratory rate,13 and SpO213 have been shown to be independently associated with worse in-hospital outcomes.
To the best of our knowledge, there has only been one out-of-ICU study, performed in high-dependency units, evaluating some potential predictors associated with CPAP failure, defined as death or intubation, in CPAP-treated patients (n = 157).5 The results of this study show that severity of pneumonia on admission and enhanced baseline IL-6 levels are both associated with death and intubation.5 Of note, 41.4% of the patients included in that study had a do-not-intubate order.
Here, we report the first large multicenter study on predictors of intubation in out-of-ICU COVID-19 patients (n = 367) candidate for intubation in the case of CPAP failure. Among the clinical and laboratory characteristics considered, we show that male gender is associated with a higher risk of intubation, in good agreement with what reported by previous studies on COVID-19 patients admitted to hospital16–18 or ICU.19
Our results identify LDH as a bona fide predictor of out-of-ICU CPAP failure. LDH is a ubiquitous intracellular enzyme, which catalyzes the interconversion of pyruvate and lactate, with concomitant interconversion of NADH and NAD+. High LDH values, resulting from multiple organ injury and decreased oxygenation paralleled by upregulation of the glycolytic pathway,20 have been associated with worse outcomes in patients with viral infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).21–24 In line with our findings, elevated LDH values have been recently shown to be associated with increased risk of severe COVID-19 pneumonia and mortality.25
A known predictor of intubation in NPPV-treated patients is PaO2/FiO2 <200 mmHg, 1 h after NPPV initiation.26 In our study, during Venturi mask oxygen therapy, the PaO2/FiO2 values were similar in both the “failed CPAP” and “successful CPAP” patient groups. In contrast, during CPAP therapy, those patients who failed had a median PaO2/FiO2 value of 121 mmHg, while those who succeeded had one above 200 mmHg.
In our study cohort, the intubation rate was 45%, also taking into account those patients (n = 30) excluded from the study because intubated on the same day CPAP was started. This intubation rate is similar to that observed in non-COVID-19 ARF patients treated with NPPV,26 but almost twice as high as that reported by two large studies on CPAP-treated COVID-19 patients (25%4 and 22%5), comprising both “do-not-intubate” and “candidate for intubation” patients. In the cohort of patients included in the study by Franco et al.,4 the severity of hypoxemic ARF, as assessed by PaO2/FiO2 is lower than in our investigation, which might explain the lower rate of CPAP failure. In the study by Aliberti et al.,5 when "do-not-intubate" patients are excluded, as in our study, the intubation rate increases up to 37%.
Finally, though beyond the aims of the present investigation, it is worth mentioning that droplets and large aerosols generated by all the respiratory therapies included CPAP in patients with COVID-19 may represent a risk factor for healthcare worker contamination despite using the recommended personal protection equipment.27,28 In a multicentre observational study, in healthcare workers treating 670 consecutive patients with confirmed COVID-19 with CPAP, NPPV or HFNC, 11.4% tested positive for infection.4 In our study, although we were not able to collect data on healthcare workers positive swabs, all strategies aimed at containing healthcare workers contamination i.e., appropriate personal protection equipment and to minimize droplet spread from CPAP i.e., minimize leaks, exhalation filter, have been undertaken.
One limitation of our study is that we were not able to assess the predictive value of the respiratory rate and ROX index and of immune system activation markers (e.g., ferritin, D-dimer) in our models due to the large number of missing data. We were also unable to record some other potential early predictors of intubation, such as ventilation-related markers (e.g., expiratory tidal volume). Missing data cause weakness in detecting statistically significant association. Nonetheless, we found LDH and PaO2/FiO2 to be associated with higher intubation probability, which, assuming that what is missing is random, corroborates their value as outcome predictors. Evidence in medical treatment at the time the study was conducted, was not against hydroxychloroquine and not yet in favor of corticosteroids as subsequently. Therefore, our data need to be confirmed in patients treated differently. Lastly, ABG after CPAP was performed over a time period ranging from 2 to 24 h, which under normal circumstances may be considered a very long time span, but it was not regarded as such in our case because we were operating during the early phase of the COVID-19 pandemic.
ConclusionsOur results reveal that gender, LDH on hospital admission and percentage of increase in PaO2/FiO2 changing from Venturi mask to CPAP therapy are independent predictors of intubation in out-of-ICU CPAP-treated COVID-19 patients.
Authors’ contributionsRV, NDV, FDC and GC, had the idea for and designed the study, had full access to all of the data in the study, took responsibility for the integrity of the data, contributed to the design of the study and to the interpretation of data for the work and drafted the paper. FBA and LS had the idea for and designed the study, had full access to all of the data in the study and, took the responsibility for the accuracy and the data analysis and drafted the paper. PN contributed to the design of the study and to the interpretation of data for the work and drafted the paper. FR, CP, CM, DC, CO, ES, LC, TC, MT, LG, MAM, GA, SB, MB, SBai, PB, SBa, VB, SC, FC, VD, LDC, MMae, MM, FMo, RP, MP, VR, DR, LV, and FV contributed to the acquisition, integrity and analysis of the data. FM contributed to the interpretation of data for the work. All authors 1) agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; 2) revised the work critically for important intellectual content; and 3) gave final approval of the version to be published.
Competing interestsFR reports personal fees for lectures from Philips Respironics, outside the submitted work.
CO has a patent, No. 102016000114357, with royalties paid from Intersurgical SpA.
DC reports personal fees from Nestlé Healthcare nutrition, outside the submitted work.
FM received fees for lectures from GE Healthcare, Hamilton Medical, Seda Spa; consulting agreement between University of Pavia and Hamilton Medical.
PN reports personal fees from Intersurgical SpA, Resmed, Philips, Novartis, MSD, Getinge, Orion Pharma and non-financial support from Draeger, outside the submitted work. In addition, PN has a pending patent, No. 102020000008305, filed to the Università di Padova, and a patent, No. 102016000114357, with royalties paid from Intersurgical S.p.A.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
We would like acknowledge the help of Dr. Arsura Marcello in reviewing and revising the manuscript for English grammar and syntax.
Authors request that names of the individual members of the COVID-19 Eastern Piedmont Network be searchable through their individual PubMed records.
COVID-19 Eastern Piedmont Network:
Gianluca Airoldi1, MD; Marta Baggiani2, MD; Sara Baino2, MD; Piero Balbo3, MD; Simona Bazzano4, MD; Valeria Bonato5, MD; Silvio Borrè6, MD; Sara Carbonati2, Luigi Castello2,7, MD; Tiziana Cena4, MD; Federico Crimaldi2, MD; Veronica Daffara2, MD; Luca De Col8, MD; Luca Grillenzoni9, MD; Matteo Maestrone2, MD; Mario Malerba2,10, MD; Maria Adele Moschella11, MD; Federica Moroni2, MD; Raffaella Perucca4, MD; Mario Pirisi2,12, MD; Valentina Rondi2, MD; Daniela Rosalba2, MD; Erminio Santangelo2, MD; Martina Taverna5,MD; Letizia Vanni2, MD; Francesca Vigone2, MD; Francesco Mojoli13, MD.
1Ospedale Ss. Trinità, Medicina Interna, Borgomanero, Italy.
2Università del Piemonte Orientale, Dipartimento di Medicina Traslazionale, Novara, Italy.
3Azienda Ospedaliero Universitaria “Maggiore della Carità”, Pneumologia, Novara, Italy.
4Azienda Ospedaliero Universitaria “Maggiore della Carità”, Anestesia e Terapia Intensiva, Novara, Italy.
5Azienda Ospedaliera SS. Antonio e Biagio e Cesare Arrigo, Department of Anesthesia and Intensive Care, Alessandria, Italy, EU.
6Azienda Ospedaliera Sant’Andrea, Malattie Infettive, Vercelli, Italy
7Azienda Ospedaliero Universitaria “Maggiore della Carità”, Medicina d’Urgenza, Novara, Italy.
8Ospedale degli Infermi, Anestesia e Rianimazione, Biella, Italy.
9Ospedale degli Infermi, Medicina D’Urgenza, Biella, Italy.
10Azienda Ospedaliera Sant’Andrea, Pneumologia, Vercelli, Italy.
11Presidio Ospedaliero Domodossola, Medicina Interna ASL VCO, Domodossola, Italy.
12Azienda Ospedaliero Universitaria “Maggiore della Carità”, Clinica Medica, Novara, Italy
13University of Pavia, Fondazione IRCCS Policlinico San Matteo, Anaesthesia and Intensive Care, Viale Camillo Golgi, 19 - 27100 Pavia, Italy.
The following is Supplementary data to this article:


