









Evidence suggests lungs as the organ most affected by coronavirus disease 2019 (COVID-19). The literature on previous coronavirus infections reports that patients may experience persistent impairment in respiratory function after being discharged. Our objective was to determine the prevalence of restrictive pattern, obstructive pattern and altered diffusion in patients post-COVID-19 infection and to describe the different evaluations of respiratory function used with these patients.
MethodsA systematic review was conducted in five databases. Studies that used lung function testing to assess post-infection COVID-19 patients were included for review. Two independent reviewers analysed the studies, extracted the data and assessed the quality of evidence.
ResultsOf the 1973 reports returned by the initial search, seven articles reporting on 380 patients were included in the data synthesis. In the sensitivity analysis, we found a prevalence of 0.39 (CI 0.24–0.56, p < 0.01, I2 = 86%), 0.15 (CI 0.09–0.22, p = 0.03, I2 = 59%), and 0.07 (CI 0.04–0.11, p = 0.31, I2 = 16%) for altered diffusion capacity of the lungs for carbon monoxide (DLCO), restrictive pattern and obstructive pattern, respectively.
ConclusionPost-infection COVID-19 patients showed impaired lung function; the most important of the pulmonary function tests affected was the diffusion capacity.
On March 11, 2020, the World Health Organization (WHO) declared coronavirus disease 2019 (COVID-19) to be a pandemic, with approximately 20% of patients infected requiring hospitalisation and 6% in critical care and needing invasive ventilatory assistance.1 Early epidemiological reports showed that 8.2% of total cases presented with rapid and progressive respiratory failure, similar to acute respiratory distress syndrome (ARDS).2
Recent evidence suggests that the lungs are the organ most affected by COVID-193 with different pathophysiological events that include diffuse alveolar epithelium destruction, hyaline membrane formation, capillary damage and bleeding, alveolar septal fibrous proliferation, and pulmonary consolidation.4 A characteristic of COVID-19 is the extensive injury to alveolar epithelial cells and endothelial cells with secondary fibroproliferation,5 indicating a potential for chronic vascular and alveolar remodelling leading to lung fibrosis and/or pulmonary hypertension.6 These findings generate concerns regarding the assessment of lung injury for discharged patients.4
Different types of functional respiratory evaluations can be carried out objectively, the most commonly used are pulmonary function tests (PFTs), such as spirometry, diffusion capacity and lung volumes,7 However, other tests that complement lung function tests, such as the evaluation of respiratory muscles or airway resistance, can help to improve the study of the properties of the lung and allow us to determine the consequences of acute or chronic respiratory disease objectively.
The abnormalities of chest computed tomography (CT), as described in the epidemiological reports, can lead to pulmonary fibrosis and, for this reason, can be analysed together with pulmonary function.3,8 Recent clinical guidelines suggest following up patients with severe pneumonia due to COVID-19 with full PFTs 12 weeks after discharge.9 In the case of mild to moderate pneumonia, the PFTs must be conducted after abnormal chest x-rays. In both cases, if any abnormality in lung function, together with a CT abnormality, is found, the patient must be referred to a specialist in interstitial lung disease.9
The first reports on lung function related to COVID-19 indicated that patients have a restrictive defect and a small airways dysfunction that can be persistent and not related to the disease severity.10 Additionally, Mo et al. reported an impairment of diffusion capacity followed by restrictive ventilatory defects, which are both associated with the severity of the disease.4 The literature on previous coronavirus infections, such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), is concordant with these reports and suggests that patients may experience persistent impairment lasting for months or even years after being discharged.11,12
Because it is essential to detect alterations in pulmonary function for the diagnosis and follow-up of patients with respiratory and functional sequelae produced by COVID-19, we decided to carry out a systematic review and meta-analysis aimed to determine the prevalence of restrictive pattern, obstructive pattern and altered diffusion in patients post-COVID-19 infection and to describe the different evaluations of respiratory function used with these patients.
MethodsProtocols and registrationWe performed a systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.13 The meta-analysis was designed and performed in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE).14 The review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42020198178).
Criteria for considering studies in this reviewWe included randomised controlled trials (RCTs) and observational studies (cross-sectional, longitudinal, case-control and cohort) of patients with a confirmed diagnosis of COVID-19. The studies included aimed to determine the use of PFTs to assess post-infection COVID-19 patients. The selected studies had to follow the ATS / ERS clinical guidelines.7 In the case of studies that include spirometry, the restrictive pattern had to be confirmed by lung volumes. To analyse the obstructive and restrictive pattern, the studies had to be based on clinical guidelines, such as the ATS / ERS.7 However, in clinical practice, an FEV1 / FVC ratio of less than 0.7 has been used, so this relationship was also considered.15
Search strategies and data resourcesWe reviewed the Embase, PubMed/MEDLINE, Web of Science, CINAHL, and Cochrane Register of Clinical Trials (CENTRAL) databases on July 15, 2020. We conducted manual searches with the followings terms for condition: “SARS-CoV-2” OR “COVID-19” OR “2019 novel coronavirus infection” OR “COVID19” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “2019-nCoV disease” OR “2019 novel coronavirus disease” OR “2019-nCoV infection”. We used the following search terms for the main outcome: “respiratory assessment” OR “lung function” OR “pulmonary function” OR “spirometry” OR “total lung capacity” OR “vital capacity” OR “forced expiratory volume” OR “forced vital capacity” OR “maximal voluntary ventilation” OR “diffusing capacity for carbon monoxide” OR “transfer factor of the lung for carbon monoxide” OR “forced oscillation technique” OR “maximal inspiratory pressure” OR “maximal expiratory pressure” OR “TLC” OR “VC” OR “FVC” OR “FEV” OR “DLCO” OR “TLCO” OR “MIP” OR “MEP” OR “MVV” (Supplementary file S1). We imposed no language or publication restrictions.
The terms selected were combined using Boolean logical operators (OR, AND, NOT). We also conducted a manual search of the references included in the selected articles. All references were analysed using Rayyan web software.16
Reviewing procedure and data extractionThe selected articles were reviewed independently by investigators with experience in meta-analysis and training in literature review. First, the titles and abstracts of all identified studies were reviewed by two investigators (LSN, LVC). Studies deemed not relevant based on the review of the title and abstract were excluded. Any disagreements were solved by a third reviewer (RTC). Second, the full-text versions of the articles selected in the first stage were read and checked against the eligibility criteria (RTC, LVC) again. Any disagreements were solved by a third reviewer (JV). Additional unpublished data were obtained from study authors when possible.
Methodological quality assessmentAn assessment of the methodological quality of the primary articles was carried out using the Quality Assessment Tools from the National Heart, Lung and Blood Institute (NHLBI).17 Each tool contains criteria against which internal validity and risk of bias are evaluated. The criteria were evaluated as “Yes”, “No”, or “Other” (not reported, not applicable, or not determinable), and an overall rating was provided for each study based on the items rated with an affirmative answer: ≥ 75% = good, 50–75% = fair, < 50% = poor. Two authors carried out this evaluation independently (XAR, LVC), and discrepancies were resolved by consensus. For discrepancies that could not be resolved, a third author (HP) was consulted.
Data synthesis and analysisWe used MetaXL software version 5.3 (EpiGear International, Sunrise Beach, Queensland, Australia) for our meta-analysis and generation of a forest plot that showed combined estimates with a 95% confidence interval. We pooled the prevalence of the studies structured around individual outcomes using the double arcsine transformation method.18 We obtained combined measurements of effect for each primary outcome through meta-analysis under a random-effect model due to the expected heterogeneity between studies in prognostic reviews.19 Statistical heterogeneity was measured through the I2 statistic and classified as low (I2 < 25%), moderate (I2 25–50%), or high (I2 > 50%).20 Subgroup analysis, according to the outcome assessment and severity, was carried out. Sensitivity analysis was also carried out to assess the change in pooled prevalence due to the selective exclusion of studies.
ResultsStudy selectionThe initial search yielded 1973 potential studies (1971 from selected databases and 2 from manual searches). In total, 228 duplicate records were deleted. We screened 1745 titles and abstracts and excluded 1677 records which did not meet our inclusion criteria. Sixty-nine of these were assessed as full-text. Of these, 30 studies were excluded for being wrong publication type, 16 for wrong study design, nine for wrong outcome, six for being wrong protocol and one for wrong population. Ultimately, seven studies met the criteria for eligibility and were included in the review.4,6,10,21–24 The flow chart of the study selection process is shown in Fig. 1.
Characteristics of the included studies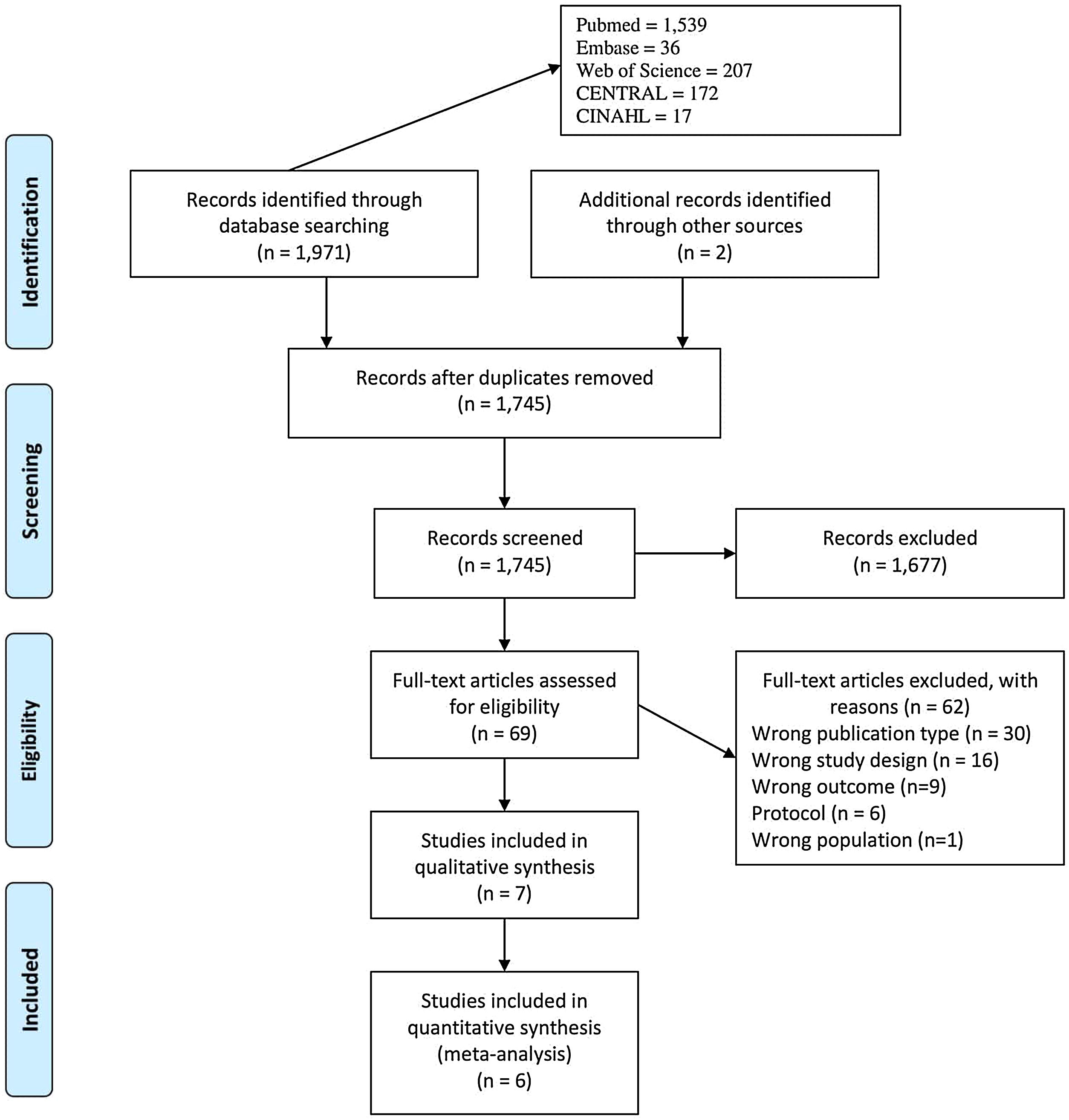
Six studies were conducted in China4,10,21–24 and one in France.6 The designs of the studies included one RCT,21 three retrospectives,6,22,24 and three prospectives (Table 1).10,21,23
Description of included articles.
| Author | Country | Design | Participants Male/Female | Age (years) | BMI (kg/m2) | Smoking | Respiratory comorbidities | Time of assessment | Quality rating* |
|---|---|---|---|---|---|---|---|---|---|
| Frija-Masson et al, 2020 | France | Retrospective | 50 | 54 (46−62) | 27 (24.6−32.5) | Active 5 (10%) | Emphysema 2 (4%) | 30 days after symptoms onset | Fair |
| 28 M/22F | Former 9 (18%) | Asthma 2 (4%) | |||||||
| Sarcoidosis 1 (2%) | |||||||||
| Huang et al, 2020 | China | Retrospective | 57 | 46.7 ± 13.7 | 23.9 ± 3.5 | History of smoking 9 (15.7%) | No patient was reported having chronic respiratory diseases | 30 days after discharge from the hospital | Poor |
| 26 M/31F | |||||||||
| Li et al, 2020 | China | Prospective | 18 | NR | NR | History of smoking 3 (16.6%) | History of tuberculosis 1 (5.5%) | Near to discharge and two weeks after | Poor |
| NR | |||||||||
| Liu et al, 2020 | China | RCT | 72 | 69.1 ± 7.8 | 23 ± 3.7 | NR | NR | NR | Fair |
| 49 M/23F | |||||||||
| Mo et al, 2020 | China | Prospective | 110 | 49.1 ± 14.0 | 23.5 ± 2.8 | Smoker 13 (11.8%) | Asthma 1 (0.9%) | 27.9 ± 7 days after the onset of disease | Fair |
| 55 M/55F | Chronic bronchitis 1 (0.9%) | ||||||||
| Bronchiectasis 1 (0.9%) | |||||||||
| You et al, 2020 | China | Prospective | 18 | 50.7 ± 12.1 | 26.4 ± 2.8 | NR | No patient was reported having chronic respiratory diseases | 38 ± 13.4 days after hospital discharge | Poor |
| 10 M/8F | |||||||||
| Zhao et al, 2020 | China | Retrospective | 55 | 47.7 ± 15.5 | NR | Active 2 (3.6%) | No underlying pulmonary diseases were observed on admission | 3 months after hospital discharge. | Fair |
| 22 M/23F | Former 2 (3.6%) |
Abbreviations: BMI: Body mass index; NR: Not reported; RCT: Randomised controlled trial.
Data are shown as Mean ± standard deviation, Median (Inter-quartile range), n (%).
In total, 380 post-infection COVID-19 patients were enrolled in the included studies. Sample sizes varied between 1810,23 and 1104 participants. The studies included 162 females and 190 males with mean age varied between 46.7 ± 13.7 and 69.1 ± 7.8 years. One study did not report the gender and mean age of the patients.23 Five studies reported that between 6% and 18% of patients had a history of smoking,4,6,22–24 while two studies did not report this.10,21 Three studies reported respiratory comorbidities,4,6,23 including emphysema,6 asthma,4,6 sarcoidosis,6 tuberculosis,23 chronic bronchitis4 and bronchiectasis.4
Time of assessmentThere was a wide range in the time of assessment. Two authors reported that respiratory assessment were conducted one month after symptom onset.4,6 a further two authors reported that they were conducted one month after discharge,10,22 One author reported that they were conducted three months after discharge.24 another reported two assessment times, close to discharge and two weeks after discharge,23 and one author did not report the time of assessment.21
Methodological quality assessmentThe methodological quality of the studies was determined to be “fair” in four studies4,6,21,24 and “poor” in three studies10,22,23 (Supplementary file S2). In our analysis of design, we used the NHLBI’s Quality Assessment of Controlled Intervention Studies tool in one study rated as “fair”.21 We used the NHLBI’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies in six studies, with three being rated as “fair”4,6,24 and three being rated as “poor”.10,22,23
Main findingsSpirometry and lung volumesSeven studies reported the spirometry test (Table 2, Supplementary file S3).4,6,10,21–24 All studies showed forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), and FEV1/FVC ratio.4,6,10,21–24 The interpretation by severity of COVID-19 is shown in Table 3. Three studies indicated maximal mid-expiratory flow (MMEF)%,4,10,23 and one reported maximal voluntary ventilation (MVV).10 Six studies reported lung volumes.4,6,10,22–24 The most-reported parameters were TLC,4,6,22,24 residual volume (RV)4,22 and vital capacity (VC).10,23 Only one study reported tidal volume, expiratory reserve volume, inspiratory reserve volume and inspiratory capacity.10
Pulmonary function tests of included studies.
| Frija-Masson et al, (n = 50) | Huang et al, (n = 57) | Li et al, (n = 18) | Liu et al, (n = 72) | Mo et al, (n = 110) | You et al, (n = 18) | Zhao et al, (n = 55) | |
|---|---|---|---|---|---|---|---|
| Spirometry | |||||||
| FVC, L | NR | NR | NR | 1.78 ± 0.58 | NR | NR | NR |
| FVC, % of predicted | 93 (85−99) | 101 ± 15.9 | 91.5 ± 17.3 | NR | 93.6 ± 12.3 | 105.1 ± 23.3 | NR |
| FEV1, L | NR | NR | NR | 1.11 ± 0.11 | NR | NR | NR |
| FEV1, % of predicted | 93 (83−100) | 97.9 ± 14.9 | 89.4 ± 15.7 | NR | 92.7 ± 11.6 | 101 ± 19.5 | NR |
| FEV1/FVC | 0.81 (0.75−0.87) | 81.2 ± 6.1 | 80.5 ± 7.0 | 60.5 ± 6.2 | 80.7 ± 5.8 | 77.9 ± 8.1 | NR |
| Lung volumes | |||||||
| TLC, % of predicted | 91.5 (81−103) | 93.9 ± 12.8 | NR | NR | 86.3 ± 11.3 | NR | NR |
| Diffusion capacity | |||||||
| DLCO, % of predicted | 80 (70−92) | 78.4 ± 13.6 | NR | 60.5 ± 11.7 | 78.2 ± 14.3 | NR | NR |
| DLCO/VA, % of predicted | 94 (78−108) | NR | NR | NR | 92.1 ± 16.7 | NR | NR |
| PFT Interpretation | |||||||
| Restrictive, n (%) | 13 (26) | 7 (12.3)## | 5 (27.7) | NR | 10 (9.09)# | 3 (16.7)# | 6 (10.9) |
| 27 (25)## | 4 (7.3) | ||||||
| Obstructive, n (%) | 2 (4) | 6 (10.5) | 1 (5.5) | NR | 5 (4.55)* | 3 (16.7)* | NR |
| Altered difusion, n (%) | 22 (44) | 30 (52.6)** | NR | NR | 51 (47.22)** | NR | 9 (16.4)** |
| Time of assessment | 30 days after symptoms onset | 30 days after discharge from the hospital | Near to discharge and two weeks after | NR | 27.9 ± 7 days after the onset of disease | 38 ± 13.4 days after hospital discharge | 3 months after hospital discharge |
Abbreviations: DLCO: Diffusion capacity of the lungs for carbon monoxide; FVC: Forced vital capacity; FEV1: Forced expiratory volume in the first second; NR: Not reported; TLC: Total lung capacity. Data are shown as Mean ± SD, Median (Inter-quartile range), n (%).
#Author reported values lower 80% predicted FVC.
##Author reported values lower 80% predicted TLC.
*Author reported values lower 70% predicted FEV1/FVC.
**Author reported values lower 80% predicted DLCO.
Pulmonary function tests (PFT) interpretation by severity.
| Frija-Masson et al, 2020& | Huang et al, 2020 | Mo et al, 2020 | You et al, 2020 | |||||
|---|---|---|---|---|---|---|---|---|
| PFT Interpretation | Non-severe | Severe | Non-severe | Severe | Non-severe | Severe | Non-severe | Severe |
| n = 29 | n = 16 | n = 40 | n = 17 | n = 91 | n = 19 | n = 12 | n = 6 | |
| Restrictive, n (%) | 5 (17.2) | 8 (50) | 2 (5)# | 4 (23.5)# | 8 (8.8)# | 2 (10.53)# | 1 (8.3) | 2 (33.3) |
| 3 (7.5)## | 4 (23.5)## | 18 (19.8)## | 9 (47.37)## | |||||
| Obstructive, n (%) | NR | NR | NR | NR | 5 (5.5)* | 0 (0)* | 3 (16.7) | 0 (0) |
| Altered difusión, n (%) | 7 (24.2) | 5 (31.25) | 17 (42.5)** | 13 (76.5)** | 35 (38.5)** | 16 (84.21)** | NR | NR |
| Time of assessment | 30 days after symptoms onset | 30 days after discharge from the hospital | 27.9 ± 7 days after the onset of disease | 38 ± 13.4 days after hospital discharge | ||||
#Author reported values lower 80% predicted FVC.
##Author reported values lower 80% predicted TLC.
*Author reported values lower 70% predicted FEV1/FVC.
**Author reported values lower 80% predicted DLCO.
&Only 45 patients were classified by severity.
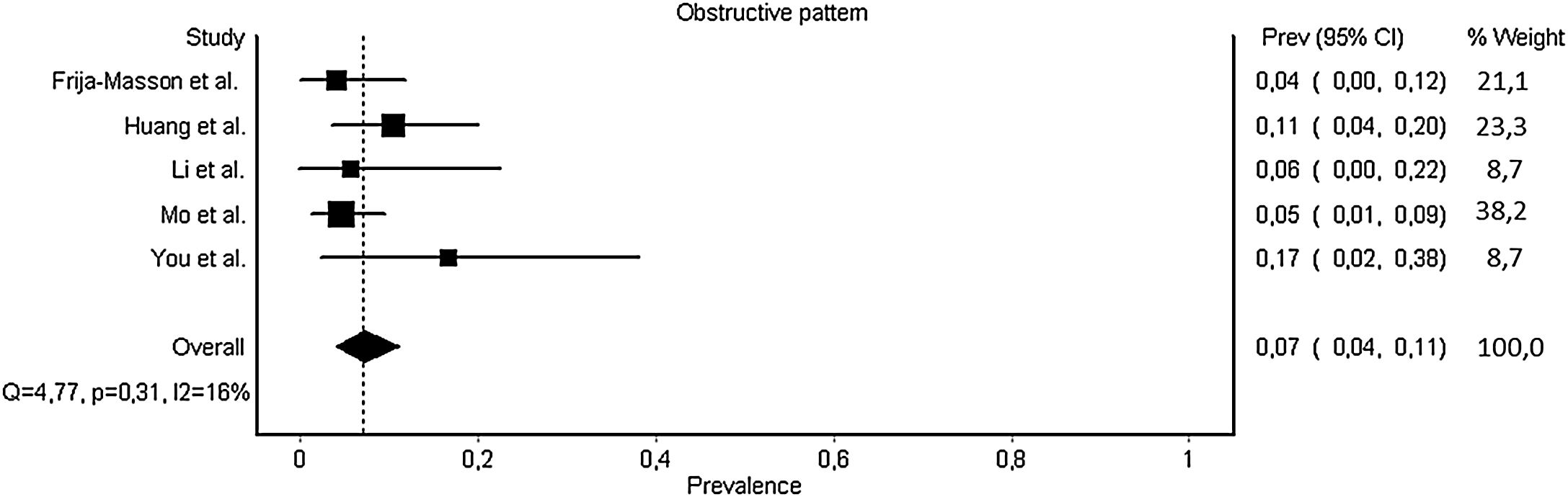
One study did not report patterns of PFT abnormality;21 therefore, in sensitivity analysis, we analysed six studies4,6,10,22–24 and found a prevalent restrictive pattern of 0.15 (CI 0.09–0.22, p = 0.03, I2 = 59%) (Fig. 2). In the case of obstructive pattern, prevalence was 0.07 (CI 0.04–0.11, p = 0.31, I2 = 16%) (Fig. 3). We did not analyse severity for restrictive and obstructive patterns because there were insufficient articles.
Diffusion capacity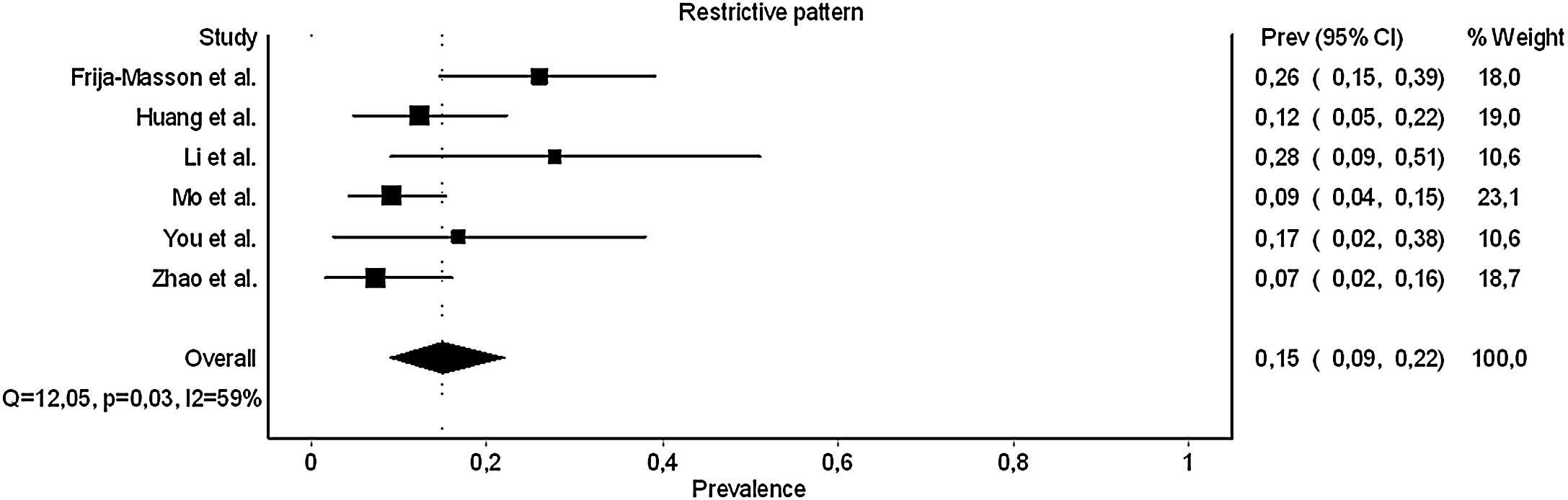
Five studies reported diffusion capacity of the lungs for carbon monoxide (DLCO) (Table 2, Supplementary file S3).4,6,21,22,24 Two studies reported DLCO/VA.4,6 The interpretation by severity is shown in Table 3. In sensitivity analysis, we include three studies4,6,22 and found a prevalence of altered diffusion capacity of 0.39 (CI 0.24–0.56, p < 0.01, I2 = 86%) (Fig. 4). In the analysis of severity, we excluded one study that had not performed this sub-analysis.24 The prevalence found was 0.66 (CI 0.31–0.94, p < 0.01, I2 = 82%) for severe patients and 0.36 (CI 0.28–0.46, p = 0.27, I2 = 25%) for non-severe patients.
Other respiratory measures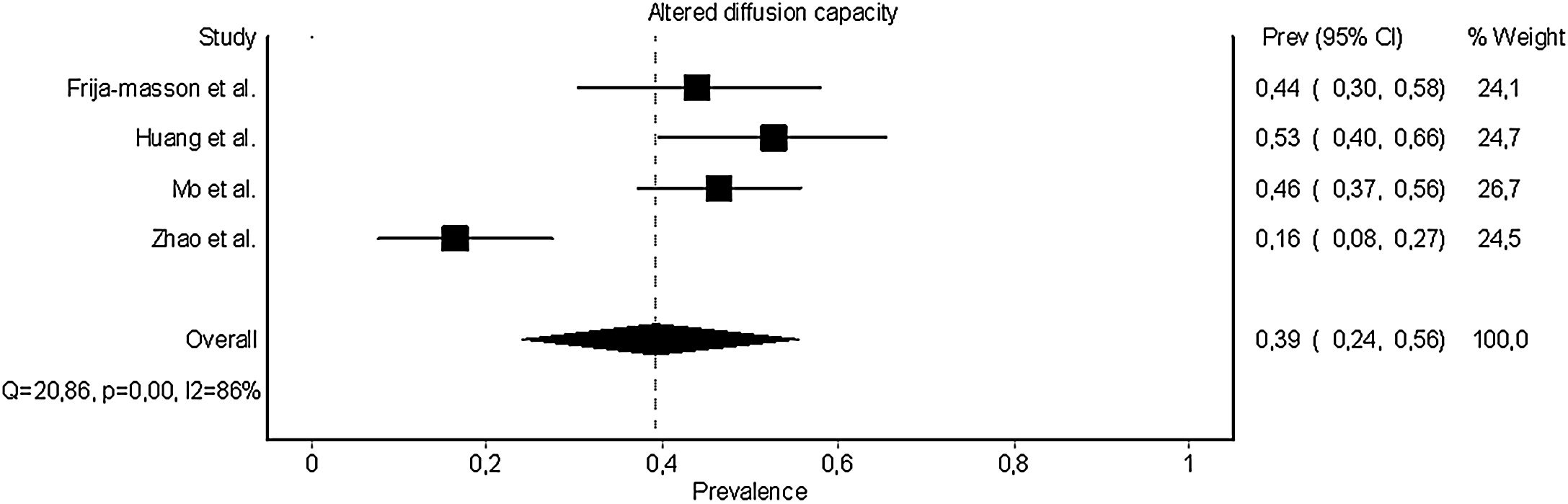
One study reported the use of an impulse oscillation system.22 The parameters reported were airway resistance at an oscillation frequency of 5 Hz (R5) and of 20 Hz (R20).22 The values obtained were 126.6 ± 29.5%pred and 132.8 ± 30.9%pred for R5 and R20, respectively. One study reported on respiratory muscle strength.22 In this study, the parameters reported were maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP).22 The MIP and MEP were 76.2 ± 24.3%pred, and 102.7 ± 32.7%pred, respectively (Supplementary file S3).
DiscussionAltered diffusion capacity, restrictive pattern and obstructive pattern were found in 39%, 15% and 7% of patients, respectively. The assessments most commonly used to assess the respiratory function of patients with COVID-19 were spirometry, lung volumes and diffusion capacity.
We found a high prevalence of altered diffusion capacity. Similar data were found in three studies.4,6,22 in one of which the prevalence was nearly a third smaller than in the other studies.24 A possible explanation for this difference is the time of assessment. Zhao et al., who reported a 16% prevalence, performed the PFTs three months after COVID-19 patients were discharged from hospital.24 Three other studies, which reported a prevalence of between 44% and 56%,4,6,22 performed the PFTs during the first month post-infection.
An important aspect to consider is the ideal time to perform respiratory assessment tests. The British Thoracic Society (BTS) guide recommends the evaluation of PFTs at three months post-discharge, especially at follow-up with patients suspected of having an interstitial disease.9 However, in the reviewed studies, most PFTs were conducted one month after the onset of COVID-19 or one month after discharge. Haste of evaluation may lead to errors in functional diagnosis since we cannot determine how much of this limitation is a result of the disease and how much is due to inflammation from the acute event.
Autopsies of COVID-19 patients revealed different degrees of destruction in alveolar structure, and pulmonary interstitial fibrosis was observed.25 Pathological changes in the lungs could explain the impaired diffusion capacity. This finding, added to the initial reports of lung damage evidenced by CT,8 confirms the need to follow these patients, looking for interstitial diseases specifically, as recommended by some clinical guidelines.9 We found a very high prevalence of altered diffusion capacity (66%) in severe patients, especially those with high inflammatory indicators who are more likely to develop pulmonary fibrosis.26
We found a prevalence of restrictive patterns in 15% of patients. The current guidelines suggest a restrictive pattern if the FEV1/FVC ratio ≥ lower limit normal (LLN) and the FVC is < LLN, which should be confirmed by evaluating the TLC.7 Despite the higher heterogeneity (I2 = 59%), all studies that assessed spirometry also performed lung volumes. The heterogeneity can probably be explained by the different evaluation times and different methodological designs.
Regarding the obstructive pattern, we found a prevalence of 7% in the sensitivity analysis with low heterogeneity (16%). However, the authors of all studies reviewed, reported differences in criteria at the cut-off point of the obstructive alteration: Frija-Masson et al. used the LLN of GLI values6; Mo et al. and You et al. used the FEV1/FVC ratio as the cut-off point in 70%4,10; and Huang et al. used the FEV1/FVC ratio as the cut-off point in 80% and reported mild impairment in 44% of patients, but later reported only 10.5% of patients had an obstructive pattern, without indicating the method used.22 The use of the LLN of reference values to homogenise obstructive pattern findings should be reinforced so that results can be more reliable.7
An important confounding in our obstructive pattern analysis is the presence of chronic respiratory diseases as comorbidities. Frija-Masson found only two patients with obstructive patterns, but these patients had underlying respiratory diseases (one had asthma and one had sarcoidosis).6 Other authors also reported the presence of respiratory comorbidities that could influence PFTs.4,23 For this reason, we analysed this outcome with caution as the data may be overestimated.
We identified other respiratory function assessments, such as respiratory muscle strength, that provide essential information about the state of respiratory pumps and airway resistance, which is important for the confirmation of lung obstruction.22 All these assessments help to improve the respiratory characterisation of COVID-19 patients and have been recommended to characterise the functional limitations generated by this disease.27
Given the heterogeneity of the clinical presentation of COVID-19, it is essential to have simple tools to assess and monitor the impact of symptoms on the respiratory function of patients.28 Considering the large number of COVID-19 survivors who require follow-up, the use of reproducible instruments to identify patients suffering from slow or incomplete recovery will help guide the reasonable use of medical resources.28
Potential biases in the review processThe systematic review process was rigorous. The review was preceded by the publication of a protocol with all review methods described and all review authors were appropriately trained and had experience in review preparation.
Completeness of evidenceWe conducted a comprehensive search of the literature, including full‐text publications, without language restrictions or the use of filters in the search strategy. Although we only included studies published between December 2019 and July 2020, it is unlikely that any have been missed, given that publications on the topic only began to appear in December 2019.
Quality of evidenceThis systematic review followed the standard recommended methodology and was constructed in line with PRISMA guidelines.13 Two independent review authors assessed the inclusion criteria for the studies, extracted data and assessed the risk of bias of the included studies, thus reducing the risk of performance bias in the review and data extraction errors.
Sources of heterogeneityWe found wide heterogeneity in the designs. We were only able to analyse seven studies, and these were not necessarily of good quality. The majority were qualified as “poor”. The most significant concern was the time of assessment. Haste in evaluation may lead to errors in functional diagnosis since we cannot determine how much of this limitation is a result of the disease and how much is due to inflammation from the acute event.
LimitationsThe most important limitation of this study is the high heterogeneity of the selected studies, particularly among the different evaluations used. The criteria for determining the severity of pneumonia differ according to the literature; variations such as based on CT findings, guidelines of COVID-19, or use of ventilatory support. Assessing the methodological quality in the studies reviewed was difficult because different designs were identified. Another significant limitation is that the studies did not report the previous lung function of the patients, so it is not possible to know the real affect generated by the infection. This limitation can be partially remedied since it is compared with reference values; however, it should be considered that there may be a reduction in lung function due to previous respiratory diseases, effects of smoking or environmental pollution.
Finally, the assessment times were different. Although the PFTs follow specific guidelines given by the clinical guidelines of respiratory societies, it is necessary to establish standard evaluation times to facilitate comparison between different populations. In this way, we will be better able to know the real impact on respiratory function generated by COVID-19.
ConclusionPost-infection COVID-19 patients showed altered respiratory function. The most important of the PFTs affected was the diffusion capacity in close to 40% of patients. The results of PFTs must be analysed with caution and considering the respiratory comorbidities and the possible impairment generated by smoking and air pollution. Well-designed studies conducted in post-COVID-19 infection patients, taking into consideration the infection severity and based on the pulmonary function guidelines are required. Future research should be focused on the characterisation of short and long-term respiratory function sequelae to optimise the decision-making in clinical practice. The data collected to date in this systematic review could be a useful starting point for further studies.
FundingNo funding.
Conflicts of interestFB belongs to Scientific Advisory Board (Medical Graphics Corporation Diagnostics). The other authors declare to have no conflict of interest.
CRediT authorship contribution statementR. Torres-Castro: Conceptualization, Formal analysis, Methodology, Writing - original draft, Writing - review & editing. L. Vasconcello-Castillo: Conceptualization, Data curation, Formal analysis, Writing - original draft, Writing - review & editing. X. Alsina-Restoy: Writing - original draft, Writing - review & editing. L. Solis-Navarro: Data curation, Writing - original draft, Writing - review & editing. F. Burgos: Conceptualization, Formal analysis, Writing - original draft, Writing - review & editing. H. Puppo: Conceptualization, Formal analysis, Methodology, Writing - original draft, Writing - review & editing. J. Vilaró: Conceptualization, Writing - original draft, Writing - review & editing.
The following are Supplementary data to this article:







