




Gender differentials in tuberculosis (TB) have been reported worldwide. Men are more likely to be diagnosed with TB than women, with a male-to-female ratio of 1.6:1, globally.1 Different factors have been proposed to explain this gender gap including biological differences in disease and disease presentation and different access to health care specifically in developing countries.2–4 Additionally, men are more likely to report risk factors associated with TB exposure.2,4–7
The aim of this study was to estimate TB incidence by age and sex in Portugal and to analyse factors influencing the risk of active TB among men and women by age group.
This was a retrospective cohort study conducted in Portugal (January/2010–December/2014). The resident population data was provided by Statistics Portugal and the TB cases and their clinical, demographic and social characteristics by the National TB Surveillance System (2010–2014).
A statistical analysis was performed using SPSS® 22.0. Categorical variables were presented as counts and proportions and compared using the Chi-square test. Continuous variables with normal distribution were described by mean and standard deviation (SD) and were compared using the Student's t-test for two independent samples. Statistical significance was achieved at a significance level of 0.05. Male-to-female ratio, TB notification rates and corresponding 95% confidence intervals (95% CI) were computed, and multivariable logistic regression was used to estimate odds ratio (OR) and 95% CI.
In the study period, 12,314 patients were notified, mean age 47.3±18.9 years, 65.8% male (n=8097). TB notification rate was significantly higher in males compared to females after the second decade of life. In males, the highest notification rate was 52.2 per 100,000 inhabitants (95% CI 49.9–54.5) in the 40–49 age group and in females it was 23.4 (95% CI 21.7–25.2) in the 20–29 age group (Fig. 1a).
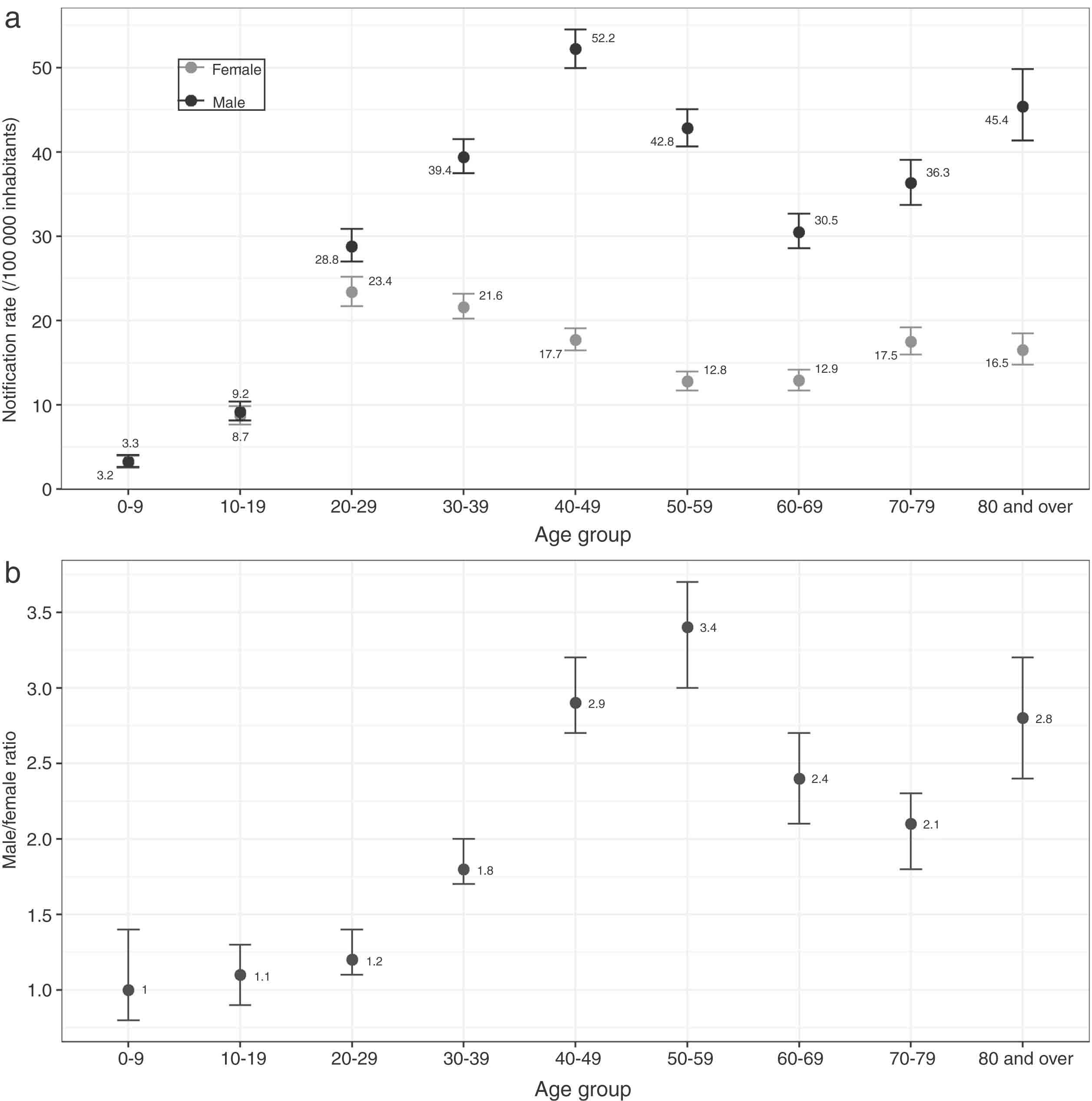
After the second decade of life there was a progressive increase in the male-to-female ratio that reached the highest value in the 50–59 age group (male:female ratio=3.4; 95% CI 3.0–3.7) (Fig. 1b). After a decrease in the sex ratio, sex differences increased again later in life (≥80 years).
Since TB notification rate was significantly higher in males after the second decade of life, we analysed the distribution of TB risk factors by sex from that age onwards (Table 1). Compared with women, male patients aged ≥20 years had higher odds of silicosis (OR 20.23; 95% CI 7.47–54.84), imprisonment (14.94; 6.58–33.92), alcohol abuse (6.27; 5.14–7.65), drug use (3.01; 2.14–4.23), lung cancer (2.76; 1.62–4.70), chronic obstructive pulmonary disease-COPD (2.19; 1.65–2.90), socioeconomic deprivation (1.22; 1.11–1.35), previous TB treatment (1.20; 1.03–1.41), and human immunodeficiency virus (HIV) infection (1.19; 1.01–1.40).
Associations and tuberculosis patients characteristics (age ≥20 years) according to sex (n=11,658).
| Male n=7753 (66.5%) | Female n=3905 (33.5%) | Total n=11658 (100%) | p-Value# | Male vs female (multivariable) OR (95% CI) | |
|---|---|---|---|---|---|
| Socioeconomic factors | |||||
| Age, years [mean (SD)] | 49.5 (16.6) | 48.7 (19.1) | 49.2 (17.5) | 0.390 | † |
| Foreign person [n (%)] | 1183 (15.3) | 656 (16.9) | 1839 (15.8) | 0.034 | 0.96 (0.86–1.08) |
| Imprisonment history [n (%)] | 262 (3.5) | 9 (0.2) | 271 (2.4) | <0.001 | 14.94 (6.58–33.92) |
| Homeless [n (%)] | 143 (1.9) | 22 (0.6) | 165 (1.5) | <0.001 | 1.04 (0.63–1.74) |
| Most deprived (Q4/5)* [n (%)] | 2093 (27.2) | 858 (22.1) | 2951 (25.5) | <0.001 | 1.22 (1.11–1.35) |
| Comorbidities [n (%)] | |||||
| Chronic renal failure (haemodialysis) | 99 (1.3) | 45 (1.2) | 144 (1.2) | 0.426 | † |
| Haematopoietic neoplasms | 52 (0.7) | 27 (0.7) | 79 (0.7) | 0.898 | † |
| HIV infection | 987 (12.7) | 310 (7.9) | 1297 (11.1) | <0.001 | 1.19 (1.01–1.40) |
| Diabetes | 495 (6.4) | 241 (6.2) | 736 (6.3) | 0.655 | † |
| Silicosis | 166 (2.1) | 4 (0.1) | 170 (1.5) | <0.001 | 20.23 (7.47–54.84) |
| Hepatic disease | 478 (6.2) | 110 (2.8) | 588 (5.0) | <0.001 | 1.04 (0.82–1.33) |
| Lung cancer | 95 (1.2) | 11 (0.3) | 106 (0.9) | <0.001 | 2.76 (1.62–4.70) |
| Other cancers | 288 (3.7) | 137 (3.5)) | 425 (3.6) | 0.574 | † |
| COPD | 339 (4.4) | 69 (1.8) | 408 (3.5) | <0.001 | 2.19 (1.65–2.90) |
| Previous TB treatment | 755 (9.7) | 273 (7.0) | 1028 (8.8) | <0.001 | 1.20 (1.03–1.41) |
| Addictions [n (%)] | |||||
| Alcohol abuse | 1428 (19.7) | 126 (3.3) | 1554 (14.1) | <0.001 | 6.27 (5.14–7.65) |
| Drug abuse | 972 (13.4) | 158 (4.2) | 1130 (9.7) | <0.001 | 3.01 (2.14–4.23) |
In bold, factors significantly associated with male sex in multivariable analysis.
Only statistically significant variables in the univariable analysis (p<0.05) were inserted in multivariable analysis and used to calculate OR.
The EDI (European Deprivation Index) score was categorized into five quintiles (first-least deprived, fifth-most deprived).8 In this analysis Q4 and Q5 were aggregated.
COPD, chronic obstructive pulmonary disease; CI, confidence interval; HIV, human immunodeficiency virus; OR, odds ratio; SD, standard deviation; TB, tuberculosis.
Additionally, we analysed sex differences in specific age groups (20–49, 50–69 and ≥70 years). In all previously mentioned age groups, male patients were more likely to suffer from alcohol abuse [(OR 5.63; 95% CI 4.38–7.24), (6.77; 4.73–9.70), (9.38; 3.76–23.40), respectively]. In the 20–49 and 50–69 age groups, men had higher odds of having silicosis [(9.67; 2.30–40.71), (13.60; 3.30–56.01), respectively], drug addiction [(3.42; 2.36–4.95), (4.14; 1.24–13.83), respectively], and to be socioeconomically deprived [(1.24; 1.08–1.41), (1.27; 1.05–1.55). The odds of COPD was higher in males aged 50–69 years and ≥70 years [(2.30; 1.40–3.81), (2.74; 1.79–4.19), respectively]. Men aged 20–49 years were also more likely to have a history of imprisonment (13.62; 5.98–31.02) and HIV infection (1.22; 1.01–1.47) compared with women of the same age. The odds of having lung cancer (2.93; 1.22–6.99), hepatic disease (1.74; 1.08–2.80) and previous TB treatment (1.47; 1.07–2.01) was higher in men 50–69 years (versus women of the same age).
Our study showed that the factors influencing the risk of TB were more frequent in male patients older than 20 and that coincided with the observed increase in the male-to-female ratio. The predominance of more comorbidities and risk factors for TB in men was reported previously.2,6 Alcohol abuse was higher in men than women in all age groups. Other risk factors and comorbidities varied according to age: HIV infection and imprisonment history were more frequent in younger men, lung cancer in middle aged men, and COPD was more frequent in middle aged and older men. Smoking is the most important risk factor for COPD and lung cancer and is also associated with pulmonary TB.5,7 Generally, men smoke more than women. Consequently, smoking is a larger contributor to the TB disease burden for men.7
One limitation of this study was that we did not analyse other factors that could be associated with differences in TB notification rate, such as health-care seeking behaviour. Another limitation was the lack of information regarding patients’ smoking habits. Although we have reasons to believe that men had a higher smoking consumption than women, since COPD was more frequent among the first, we could not properly measure the prevalence of smoking by gender in our study population. Finally, as we only compared the distribution of these risk factors in a population of TB patients, we can only conjecture that these may explain the gender gap in TB notification rate.
In conclusion, the predominance of males among TB patients is striking in the Portuguese population. Our results suggest that the higher prevalence of TB risk factors among men may contribute to this male predominance.
FundingThis study was funded by FEDER through the Operational Programme Competitiveness and Internationalization and National Funding from the Foundation for Science and Technology – FCT (Portuguese Ministry of Science, Technology and Higher Education) under the EPIUnit – Instituto de Saúde Pública, Universidade do Porto, Porto, Portugal (POCI-01-0145-FEDER-006862; Ref. UID/DTP/04750/2013).
Conflicts of interestThe author has no conflicts of interest to declare.


