

Second-hand tobacco smoke (SHS) is a major indoor pollutant that causes serious health problems for all exposed, especially children. Children are often exposed to SHS at home, due to parental or other households’ or guests’ smoking. This study describes Portuguese children's exposure to SHS at home (total and by Portuguese main regions).
In 2010/2011, a questionnaire was applied to a sample of Portuguese children in the 4th grade (N=3187, mean age 9.05±0.7 years, 51.1% male). Descriptive analysis, chi-square tests and crude odds ratios were performed.
Of the participants, 62.9% of those with smoking parents and 19.2% of those with non-smoking parents were exposed to SHS at their home. Parental smoking varied significantly among regions and was significantly associated with children's exposure to SHS at home.
Children's exposure to SHS at home was high, especially if their parents smoke. Children living in Lisbon Region presented the highest SHS exposure rate. The association of SHS exposure with geographic regions suggests the influence of social and contextual factors on smoking behaviour and on tobacco control effectiveness. Our findings highlight the need to effectively prevent children's SHS exposure at their home and to develop tailored tobacco control measures by region.
Second-hand smoke (SHS) is the smoke released into the environment mainly by burning cigarette tobacco. It is composed of a complex mixture of thousands of gases and micro-particles, including nicotine and several carcinogens, toxic and irritating substances. In 1992, the U.S. Environmental Protection Agency (EPA)1 declared SHS as a group A amongst human carcinogens, concluding that there is no safe limit to this exposure. In 2000, the World Health Organization (WHO) European Office published the indoor air quality guidelines also concluding that it is not possible to define a safe limit for SHS exposure.2
Exposure to SHS causes lung cancer and cardiovascular diseases and has a particularly negative impact on pregnancy and on children's health, namely, causing reduced intrauterine growth, spontaneous abortion, preterm birth, low birth weight, sudden death syndrome, ear problems, and respiratory diseases.2,3,4
Children are particularly vulnerable to SHS since they have a less developed airways system and a still immature immune system.5,6,7 Prevalence of chronic respiratory symptoms, such as cough, wheezing and dyspnoea, is higher among children exposed to SHS.4,7,8 These children have also a greater risk of lower respiratory tract infections (pneumonia and bronchiolitis), asthma attacks, and recurrent otitis media.4,5,8,9
Children's exposure to SHS is quite often the result of the tobacco smoked by their parents at home and/or from permissiveness towards the smoking behaviour of others indoors.10 Another important risk of this parental behaviour is the proven influence on the likelihood of children becoming smokers in the future.11,12
Despite these consequences, the WHO estimates that worldwide about half of the children (700 million) are exposed to SHS, mainly in their own homes.9,13 Two Portuguese studies revealed that 38% and 41% of the children were daily or occasionally exposed to SHS caused by their parents’ smoke.14–16
To better prevent children's exposure to SHS we need more information about the parents, other cohabitants and houseguests smoking habits. This study describes smoking habits in Portugal and children's exposure to SHS at home. It was carried out by region to get a more detailed view of the situation and to support decisions on prevention of this risk for children's health.
Material and methodsStudy design and sampling procedureThis is a cross-sectional study conducted in the school year of 2010/2011 based on a self-administered questionnaire filled in by 3187 Portuguese children in the 4th grade (mean age 9.05±0.7 years; 51.1% male).
Convenience and random sampling methods were combined to select the participants of this study. Nine municipalities (Angra do Heroísmo, Braga, Covilhã, Évora, Faro, Funchal, Lisboa, Porto, Viana do Castelo) representing the seven main regions of Portugal (NUTs II: Azores, Alentejo, Algarve, Centre, Lisbon, Madeira and North) were chosen for the sake of convenience. Considering the number of 4th grade students from the nine municipalities as a total population, and estimating that each class has 20 students, a proportional number of classes per each municipality were randomly chosen to participate in the study. The students’ response rate per municipality was between 69.2% (Funchal) and 91.9% (Angra do Heroísmo) with an average of 77.5%.
QuestionnaireThe questionnaire that was used had been developed and validated for this study. It contained multiple choice questions and four open-ended questions to measure the following variables:
Socio-demographic variables: Age, Sex, Fathers’ and Mothers’ Education level and Socio-economic level.
Children's exposure to SHS at home: Smoker family members (“does not smoke”, “yes, sometimes”, “yes, every day” or “I don’t know/I do not have any”), Family members and visitors’ permission to smoke at home (“does not smoke”, “yes, every day”, “yes, sometimes” and “does not smoke at home” or “I don’t know/I do not have any/does not live in my house”) and rules concerning smoking inside the house (“smoking is not allowed in any part of the house”; “smoking is allowed in some parts/rooms of the house”; “smoking is allowed in any parts/rooms of the house” and “smoking is allowed only on special occasions”).
ProcedureThe project and the questionnaire were approved by the Portuguese Ministry of Education. Once authorization was granted by the Governing Body of each School Group, head teachers were contacted and guidelines were given about obtaining parental or guardian authorization and about administration of the questionnaire. The questionnaires were administered according to a protocol in the classrooms by trained teachers or by members of the project team.
Data analysisThe data gathered were analyzed through the statistical software IBM SPSS Statistics version 20 for Windows. Frequencies, contingency tables, chi-squared tests and logistic regressions were used to perform the data analysis. Bi-variable analyses were conducted using chi-square to compare categorical variables and crude odds ratios (ORs) when appropriate. A two-sided p value less than 0.05 was considered statistically significant.
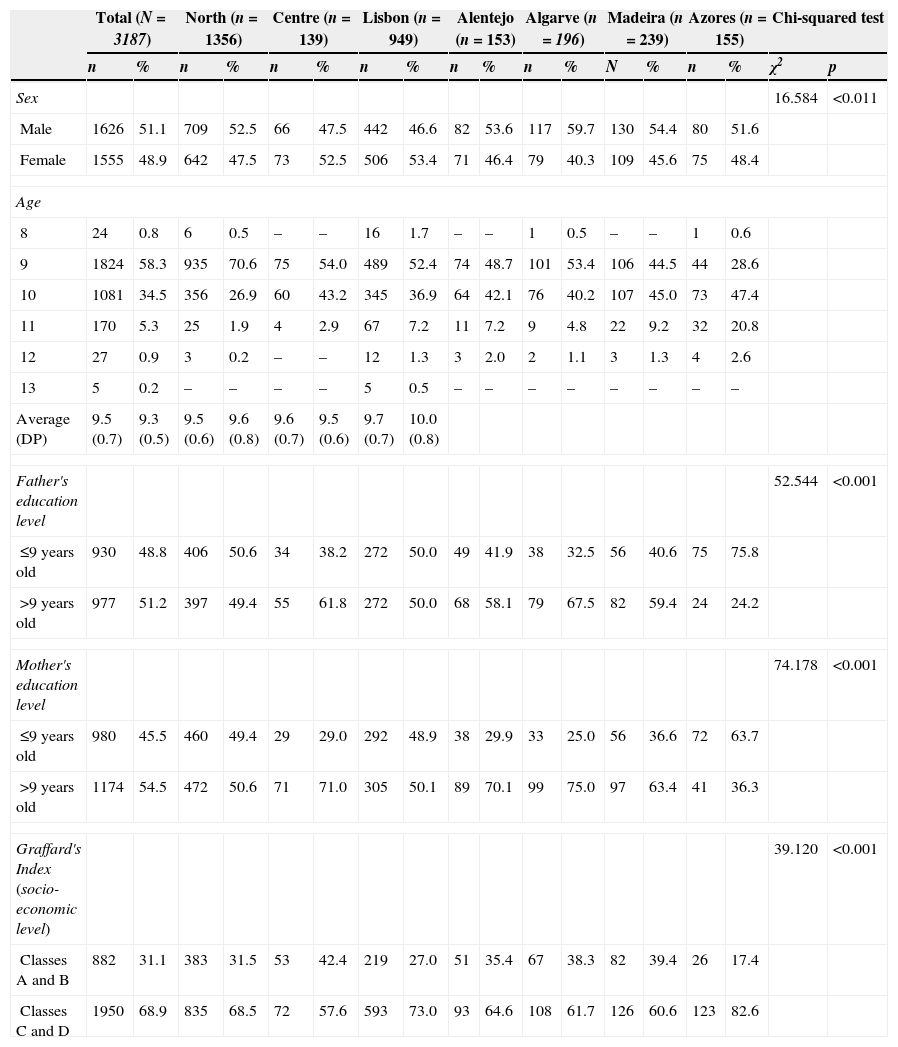
ResultsParticipant socio-demographic characteristics and their distribution throughout the Portuguese regions (NUTs II) are presented in Table 1. Fathers’ education level was inferior or equal to the 9th grade in 48.8% of the cases. Mothers’ education level was inferior or equal to the 9th grade in 45.5% of the cases. In terms of socioeconomic level, 68.9% of the cases were classified in the lowest level (classes C and D) and the remaining in the classes A and B. Observed differences according to sex, fathers’ and mothers’ education level and socioeconomic level by Portuguese regions were statistically significant.
Socio-demographic characteristics, by total and region.
| Total (N=3187) | North (n=1356) | Centre (n=139) | Lisbon (n=949) | Alentejo (n=153) | Algarve (n=196) | Madeira (n=239) | Azores (n=155) | Chi-squared test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | N | % | n | % | χ2 | p | |
| Sex | 16.584 | <0.011 | ||||||||||||||||
| Male | 1626 | 51.1 | 709 | 52.5 | 66 | 47.5 | 442 | 46.6 | 82 | 53.6 | 117 | 59.7 | 130 | 54.4 | 80 | 51.6 | ||
| Female | 1555 | 48.9 | 642 | 47.5 | 73 | 52.5 | 506 | 53.4 | 71 | 46.4 | 79 | 40.3 | 109 | 45.6 | 75 | 48.4 | ||
| Age | ||||||||||||||||||
| 8 | 24 | 0.8 | 6 | 0.5 | – | – | 16 | 1.7 | – | – | 1 | 0.5 | – | – | 1 | 0.6 | ||
| 9 | 1824 | 58.3 | 935 | 70.6 | 75 | 54.0 | 489 | 52.4 | 74 | 48.7 | 101 | 53.4 | 106 | 44.5 | 44 | 28.6 | ||
| 10 | 1081 | 34.5 | 356 | 26.9 | 60 | 43.2 | 345 | 36.9 | 64 | 42.1 | 76 | 40.2 | 107 | 45.0 | 73 | 47.4 | ||
| 11 | 170 | 5.3 | 25 | 1.9 | 4 | 2.9 | 67 | 7.2 | 11 | 7.2 | 9 | 4.8 | 22 | 9.2 | 32 | 20.8 | ||
| 12 | 27 | 0.9 | 3 | 0.2 | – | – | 12 | 1.3 | 3 | 2.0 | 2 | 1.1 | 3 | 1.3 | 4 | 2.6 | ||
| 13 | 5 | 0.2 | – | – | – | – | 5 | 0.5 | – | – | – | – | – | – | – | – | ||
| Average (DP) | 9.5 (0.7) | 9.3 (0.5) | 9.5 (0.6) | 9.6 (0.8) | 9.6 (0.7) | 9.5 (0.6) | 9.7 (0.7) | 10.0 (0.8) | ||||||||||
| Father's education level | 52.544 | <0.001 | ||||||||||||||||
| ≤9 years old | 930 | 48.8 | 406 | 50.6 | 34 | 38.2 | 272 | 50.0 | 49 | 41.9 | 38 | 32.5 | 56 | 40.6 | 75 | 75.8 | ||
| >9 years old | 977 | 51.2 | 397 | 49.4 | 55 | 61.8 | 272 | 50.0 | 68 | 58.1 | 79 | 67.5 | 82 | 59.4 | 24 | 24.2 | ||
| Mother's education level | 74.178 | <0.001 | ||||||||||||||||
| ≤9 years old | 980 | 45.5 | 460 | 49.4 | 29 | 29.0 | 292 | 48.9 | 38 | 29.9 | 33 | 25.0 | 56 | 36.6 | 72 | 63.7 | ||
| >9 years old | 1174 | 54.5 | 472 | 50.6 | 71 | 71.0 | 305 | 50.1 | 89 | 70.1 | 99 | 75.0 | 97 | 63.4 | 41 | 36.3 | ||
| Graffard's Index (socio-economic level) | 39.120 | <0.001 | ||||||||||||||||
| Classes A and B | 882 | 31.1 | 383 | 31.5 | 53 | 42.4 | 219 | 27.0 | 51 | 35.4 | 67 | 38.3 | 82 | 39.4 | 26 | 17.4 | ||
| Classes C and D | 1950 | 68.9 | 835 | 68.5 | 72 | 57.6 | 593 | 73.0 | 93 | 64.6 | 108 | 61.7 | 126 | 60.6 | 123 | 82.6 | ||
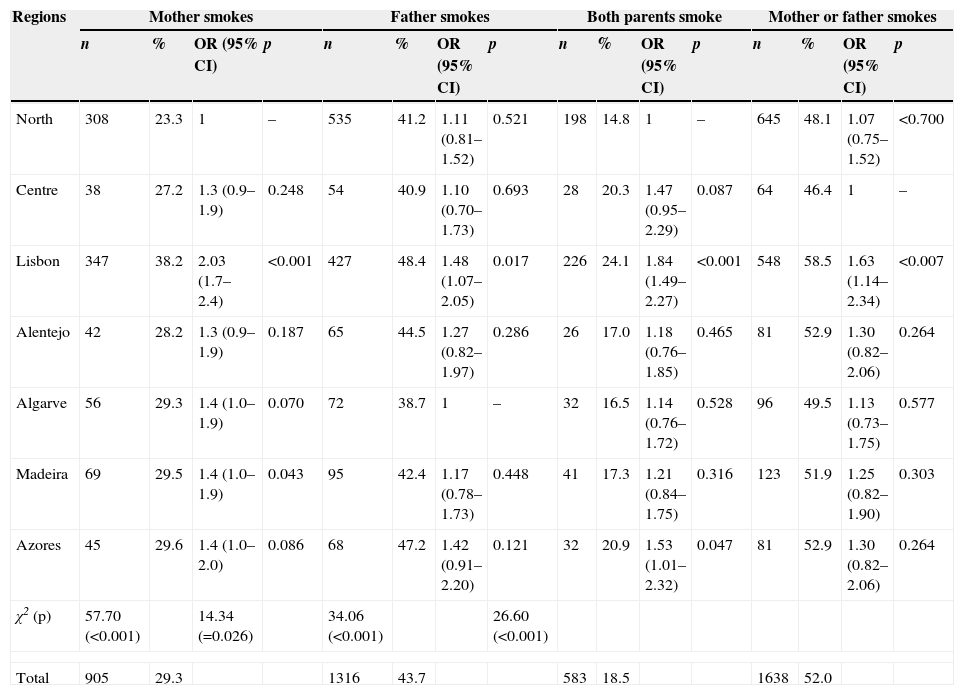
More than half (52.0%) of the children had at least one smoking mother or father (Table 2), consequently, these children were potentially exposed to SHS in their own homes. The differences between the various regions regarding the prevalence of a smoking mother or father were statistically significant (χ2=26.6; p<0.001) and vary from 46.4% in the Centre Region to 58.5% in the Lisbon Region (OR=1.6; p=0.007).
Prevalence of smokers among mothers, fathers, both parents and mother or father, by region and total.
| Regions | Mother smokes | Father smokes | Both parents smoke | Mother or father smokes | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | OR (95% CI) | p | n | % | OR (95% CI) | p | n | % | OR (95% CI) | p | n | % | OR (95% CI) | p | |
| North | 308 | 23.3 | 1 | – | 535 | 41.2 | 1.11 (0.81–1.52) | 0.521 | 198 | 14.8 | 1 | – | 645 | 48.1 | 1.07 (0.75–1.52) | <0.700 |
| Centre | 38 | 27.2 | 1.3 (0.9–1.9) | 0.248 | 54 | 40.9 | 1.10 (0.70–1.73) | 0.693 | 28 | 20.3 | 1.47 (0.95–2.29) | 0.087 | 64 | 46.4 | 1 | – |
| Lisbon | 347 | 38.2 | 2.03 (1.7–2.4) | <0.001 | 427 | 48.4 | 1.48 (1.07–2.05) | 0.017 | 226 | 24.1 | 1.84 (1.49–2.27) | <0.001 | 548 | 58.5 | 1.63 (1.14–2.34) | <0.007 |
| Alentejo | 42 | 28.2 | 1.3 (0.9–1.9) | 0.187 | 65 | 44.5 | 1.27 (0.82–1.97) | 0.286 | 26 | 17.0 | 1.18 (0.76–1.85) | 0.465 | 81 | 52.9 | 1.30 (0.82–2.06) | 0.264 |
| Algarve | 56 | 29.3 | 1.4 (1.0–1.9) | 0.070 | 72 | 38.7 | 1 | – | 32 | 16.5 | 1.14 (0.76–1.72) | 0.528 | 96 | 49.5 | 1.13 (0.73–1.75) | 0.577 |
| Madeira | 69 | 29.5 | 1.4 (1.0–1.9) | 0.043 | 95 | 42.4 | 1.17 (0.78–1.73) | 0.448 | 41 | 17.3 | 1.21 (0.84–1.75) | 0.316 | 123 | 51.9 | 1.25 (0.82–1.90) | 0.303 |
| Azores | 45 | 29.6 | 1.4 (1.0–2.0) | 0.086 | 68 | 47.2 | 1.42 (0.91–2.20) | 0.121 | 32 | 20.9 | 1.53 (1.01–2.32) | 0.047 | 81 | 52.9 | 1.30 (0.82–2.06) | 0.264 |
| χ2 (p) | 57.70 (<0.001) | 14.34 (=0.026) | 34.06 (<0.001) | 26.60 (<0.001) | ||||||||||||
| Total | 905 | 29.3 | 1316 | 43.7 | 583 | 18.5 | 1638 | 52.0 | ||||||||
In this sample, 43.7% of the fathers and 29.3% of the mothers were smokers. The prevalence of smoking fathers differs by region (χ2=24.3; p=0.026) from 38.7% in Algarve to 48.4% in Lisbon. Also among mothers, the smoking prevalence varies significantly by region, from 23.3% in the North to 38.2% in Lisbon (χ2=57.7; p<0.001).
Among the participants, 18.5% both parents were smokers. The differences between regions in this category were statistically significant (χ2=34.1; p<0.001) and vary between 14.8% in the North to 24.1% in Lisbon.
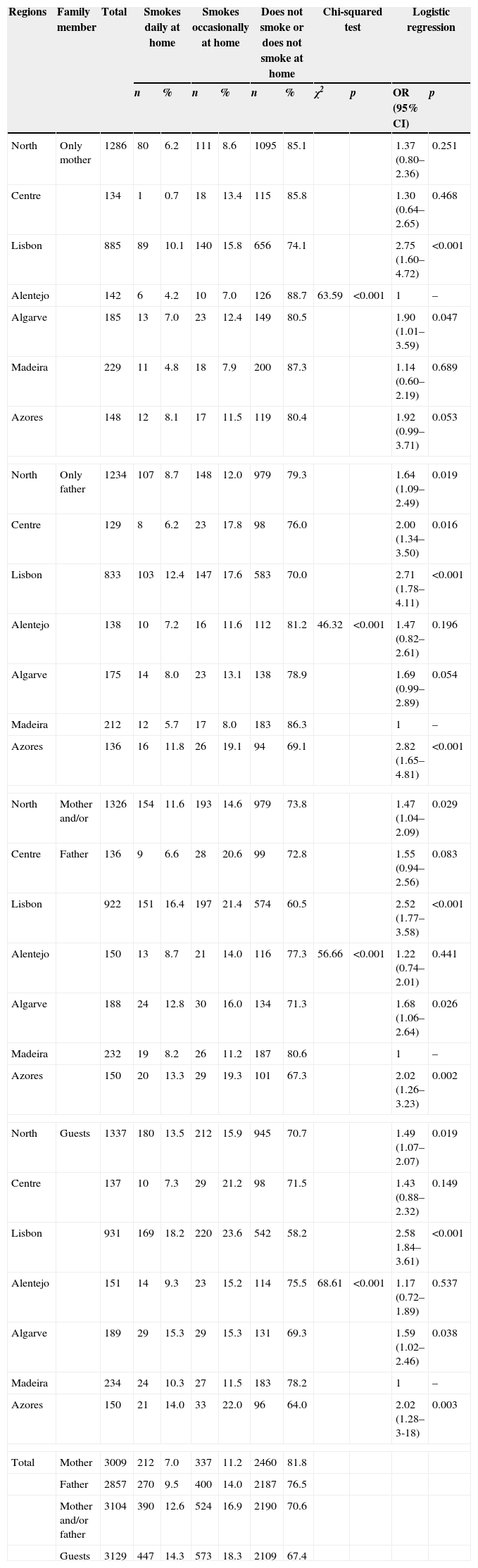
Children's exposure to SHS at home is presented in Table 3. In the total sample, 29.5% of the participants claimed they were exposed to SHS caused by a smoking parent–mother and/or father (16.9% occasionally and 12.6% on a daily basis). The exposure to the fathers’ smoke (23.5% in total and 30.0% in Lisbon) is more common than the exposure to the mothers’ smoke (18.2% in total and 25.9% in Lisbon). A smoking guest was the most frequent cause of children's exposure to SHS and affected around a third of the participants (32.6%, 18.3% occasionally and 14.3% daily).
Prevalence of children's SHS exposure at home, considering family member smoking status, by region and total.
| Regions | Family member | Total | Smokes daily at home | Smokes occasionally at home | Does not smoke or does not smoke at home | Chi-squared test | Logistic regression | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | χ2 | p | OR (95% CI) | p | |||
| North | Only mother | 1286 | 80 | 6.2 | 111 | 8.6 | 1095 | 85.1 | 1.37 (0.80–2.36) | 0.251 | ||
| Centre | 134 | 1 | 0.7 | 18 | 13.4 | 115 | 85.8 | 1.30 (0.64–2.65) | 0.468 | |||
| Lisbon | 885 | 89 | 10.1 | 140 | 15.8 | 656 | 74.1 | 2.75 (1.60–4.72) | <0.001 | |||
| Alentejo | 142 | 6 | 4.2 | 10 | 7.0 | 126 | 88.7 | 63.59 | <0.001 | 1 | – | |
| Algarve | 185 | 13 | 7.0 | 23 | 12.4 | 149 | 80.5 | 1.90 (1.01–3.59) | 0.047 | |||
| Madeira | 229 | 11 | 4.8 | 18 | 7.9 | 200 | 87.3 | 1.14 (0.60–2.19) | 0.689 | |||
| Azores | 148 | 12 | 8.1 | 17 | 11.5 | 119 | 80.4 | 1.92 (0.99–3.71) | 0.053 | |||
| North | Only father | 1234 | 107 | 8.7 | 148 | 12.0 | 979 | 79.3 | 1.64 (1.09–2.49) | 0.019 | ||
| Centre | 129 | 8 | 6.2 | 23 | 17.8 | 98 | 76.0 | 2.00 (1.34–3.50) | 0.016 | |||
| Lisbon | 833 | 103 | 12.4 | 147 | 17.6 | 583 | 70.0 | 2.71 (1.78–4.11) | <0.001 | |||
| Alentejo | 138 | 10 | 7.2 | 16 | 11.6 | 112 | 81.2 | 46.32 | <0.001 | 1.47 (0.82–2.61) | 0.196 | |
| Algarve | 175 | 14 | 8.0 | 23 | 13.1 | 138 | 78.9 | 1.69 (0.99–2.89) | 0.054 | |||
| Madeira | 212 | 12 | 5.7 | 17 | 8.0 | 183 | 86.3 | 1 | – | |||
| Azores | 136 | 16 | 11.8 | 26 | 19.1 | 94 | 69.1 | 2.82 (1.65–4.81) | <0.001 | |||
| North | Mother and/or | 1326 | 154 | 11.6 | 193 | 14.6 | 979 | 73.8 | 1.47 (1.04–2.09) | 0.029 | ||
| Centre | Father | 136 | 9 | 6.6 | 28 | 20.6 | 99 | 72.8 | 1.55 (0.94–2.56) | 0.083 | ||
| Lisbon | 922 | 151 | 16.4 | 197 | 21.4 | 574 | 60.5 | 2.52 (1.77–3.58) | <0.001 | |||
| Alentejo | 150 | 13 | 8.7 | 21 | 14.0 | 116 | 77.3 | 56.66 | <0.001 | 1.22 (0.74–2.01) | 0.441 | |
| Algarve | 188 | 24 | 12.8 | 30 | 16.0 | 134 | 71.3 | 1.68 (1.06–2.64) | 0.026 | |||
| Madeira | 232 | 19 | 8.2 | 26 | 11.2 | 187 | 80.6 | 1 | – | |||
| Azores | 150 | 20 | 13.3 | 29 | 19.3 | 101 | 67.3 | 2.02 (1.26–3.23) | 0.002 | |||
| North | Guests | 1337 | 180 | 13.5 | 212 | 15.9 | 945 | 70.7 | 1.49 (1.07–2.07) | 0.019 | ||
| Centre | 137 | 10 | 7.3 | 29 | 21.2 | 98 | 71.5 | 1.43 (0.88–2.32) | 0.149 | |||
| Lisbon | 931 | 169 | 18.2 | 220 | 23.6 | 542 | 58.2 | 2.58 1.84–3.61) | <0.001 | |||
| Alentejo | 151 | 14 | 9.3 | 23 | 15.2 | 114 | 75.5 | 68.61 | <0.001 | 1.17 (0.72–1.89) | 0.537 | |
| Algarve | 189 | 29 | 15.3 | 29 | 15.3 | 131 | 69.3 | 1.59 (1.02–2.46) | 0.038 | |||
| Madeira | 234 | 24 | 10.3 | 27 | 11.5 | 183 | 78.2 | 1 | – | |||
| Azores | 150 | 21 | 14.0 | 33 | 22.0 | 96 | 64.0 | 2.02 (1.28–3-18) | 0.003 | |||
| Total | Mother | 3009 | 212 | 7.0 | 337 | 11.2 | 2460 | 81.8 | ||||
| Father | 2857 | 270 | 9.5 | 400 | 14.0 | 2187 | 76.5 | |||||
| Mother and/or father | 3104 | 390 | 12.6 | 524 | 16.9 | 2190 | 70.6 | |||||
| Guests | 3129 | 447 | 14.3 | 573 | 18.3 | 2109 | 67.4 | |||||
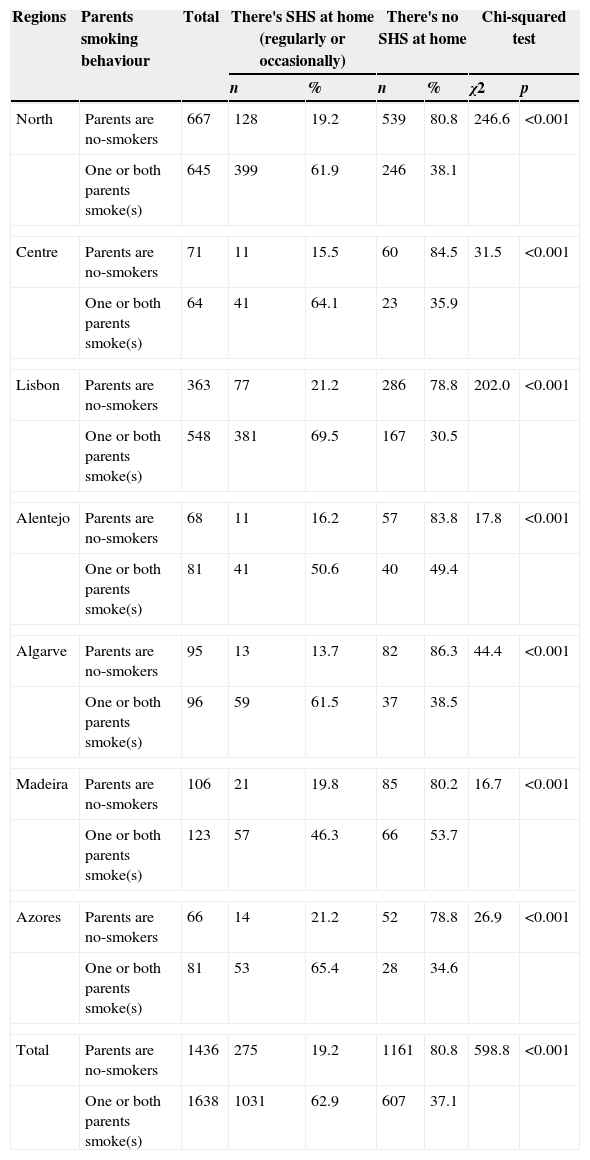
Comparing children with non-smoking parents and with smoking parents (Table 4), we found great differences in the prevalence of children's exposure to SHS at home. These differences are statistically significant in the total sample and in all regions considered. For instance, in relation to the total sample, of the children with non-smoking parents, 19.2% were exposed to SHS at home, whereas of the children with smoking parents, the prevalence rate of those exposed was 63.3% (χ2=598.8; p<0.001). On the other hand, in the subgroup with smoking parents, 37.1% of the participants declared that they were not exposed to SHS at home.
Prevalence of children's SHS exposure at home, comparing cases with non smoking parents and cases with smoking parents, by region and total.
| Regions | Parents smoking behaviour | Total | There's SHS at home (regularly or occasionally) | There's no SHS at home | Chi-squared test | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | χ2 | p | |||
| North | Parents are no-smokers | 667 | 128 | 19.2 | 539 | 80.8 | 246.6 | <0.001 |
| One or both parents smoke(s) | 645 | 399 | 61.9 | 246 | 38.1 | |||
| Centre | Parents are no-smokers | 71 | 11 | 15.5 | 60 | 84.5 | 31.5 | <0.001 |
| One or both parents smoke(s) | 64 | 41 | 64.1 | 23 | 35.9 | |||
| Lisbon | Parents are no-smokers | 363 | 77 | 21.2 | 286 | 78.8 | 202.0 | <0.001 |
| One or both parents smoke(s) | 548 | 381 | 69.5 | 167 | 30.5 | |||
| Alentejo | Parents are no-smokers | 68 | 11 | 16.2 | 57 | 83.8 | 17.8 | <0.001 |
| One or both parents smoke(s) | 81 | 41 | 50.6 | 40 | 49.4 | |||
| Algarve | Parents are no-smokers | 95 | 13 | 13.7 | 82 | 86.3 | 44.4 | <0.001 |
| One or both parents smoke(s) | 96 | 59 | 61.5 | 37 | 38.5 | |||
| Madeira | Parents are no-smokers | 106 | 21 | 19.8 | 85 | 80.2 | 16.7 | <0.001 |
| One or both parents smoke(s) | 123 | 57 | 46.3 | 66 | 53.7 | |||
| Azores | Parents are no-smokers | 66 | 14 | 21.2 | 52 | 78.8 | 26.9 | <0.001 |
| One or both parents smoke(s) | 81 | 53 | 65.4 | 28 | 34.6 | |||
| Total | Parents are no-smokers | 1436 | 275 | 19.2 | 1161 | 80.8 | 598.8 | <0.001 |
| One or both parents smoke(s) | 1638 | 1031 | 62.9 | 607 | 37.1 | |||
This study aims to describe children's exposure to SHS at home based on a sample of Portuguese children attending the 4th school grade. The study presents data from the total sample and from the main Portuguese administrative regions (NUTs II): Alentejo, Algarve, Azores, Centre, Lisbon, Madeira and North. The SHS at home is caused by the smoking of parents, other family members and guests.
In this sample, 43.7% of the fathers and 29.3% of the mothers were smokers. Comparing this with the prevalence for the group 35–44 years old obtained in the latest National Health Survey, the results of this study are similar for men (43.7% and 44.6%) and are substantially higher for women (29.3% and 20.9%).17
More than half of the participants had a smoking parent (mother or father) and for almost a fifth both parents smoked, thus increasing the risk of exposure to SHS and the severity of this exposure. These data were substantially different within the various regions studied, thus reinforcing the hypothesis that people's social context is an important determinant of parents smoking behaviour and of children's exposure to SHS at home.
A guest who smokes is the most common cause for children's exposure to SHS at home, suggesting that rules concerning smoking at home are more easily ignored when the family has visitors. Children's exposure to SHS at home due to the smoking of their parents (mother, father or both) is also common, including 30% of the study participants. Children's exposure to SHS resulting from the smoking of the father is slightly higher than that resulting from the smoking of the mother, but the percentage of smoking mothers who smoke at home was higher than the one of smoking fathers. These results put even more stress on the risks of female smoking and the need for more information and more awareness campaigns on this issue targeted to women.
The results show that a substantial proportion of smoking parents do not smoke at home. This is an important finding, confirming that it is possible to be a smoker and, yet, partially protect children and the family house from SHS – only partially since smokers pollute their house even when they do not smoke there because they carry toxic tobacco substances on their clothes and body (third-hand smoke).13
Of the parents who smoke at home, the majority smoke only occasionally, which might be seen as a sign that they are aware of the risks and that they are actively trying to avoid them. Investing in increasing the awareness of the smoking parents about the SHS risks may expand this home-protecting behaviour.
Comparing the subgroups with smoking and non-smoking parents, we found great differences in children's exposure to SHS. On the one hand, even in cases with non-smoking parents about a fifth of the children was exposed to SHS at home and, on the other hand, in cases with smoking parents more than a third seems to be protected from SHS exposure at home. These results confirm the need to raise awareness about this risk among general population and to insist on measures to prevent it.
The analysis by region reveals both significant and coherent differences. Lisbon has the highest prevalence of children exposed to SHS at home. In relation to the National Health Survey, Lisbon is also the Portuguese region with the highest prevalence of women who smoke.17 Lisbon is the main region of Portugal, so, these results may work as a negative forecast, suggesting that the Portuguese situation may worsen in the coming years.
This study has some limitations. First of all, the sample only includes children attending the 4th school grade, which is an important limitation to take into account. The sample size is quite small in some regions and the sampling method is limited, which means that the sample is not always totally representative at regional and at national levels. The data gathering was based on children's self-report without a biological validation, which is another limitation of the study: these limitations are the result of budgetary restrictions. Despite these limitations, this is the first study performed in Portugal with a large sample of the population attending the 4th school grade which includes participants from all of the seven main regions of Portugal, thus allowing a good description of the situation regarding Portuguese children's exposure to SHS at home.
To conclude, Portuguese children's exposure to SHS was high, especially when their parents smoke. SHS exposure association with geographic regions suggests the influence of social and contextual factors on smoking behaviour and on tobacco control. Our findings highlight the need of effective prevention measures to avoid children's SHS exposure at home and to promote a more equitable society.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would also like to thank all schools and teachers who collaborated in the study implementation and all students who took part in the study.
This work was supported by FEDER through the Programa Operacional Factores de Competitividade – COMPETE (FCOMP-01-0124-FEDER-009117), and by FCT – Fundação para a Ciência e a Tecnologia (Ref. PTDC/CPE-CED/098281/2008).


