



Obstructive sleep apnea (OSA) affects approximately 1–3% of pediatric population and is associated with significant morbidity. As adenotonsillar hypertrophy (ATH) is its primary cause in children, elective adenotonsillectomy is the first treatment of choice. Noninvasive ventilation (NIV) has been increasingly considered as an option, mainly for children with complex diseases, ineligible or waiting for surgeries, or after surgery failure.
ObjectivesTo describe the experience in the management of children with complex OSA, and to evidence the feasibility and advantages of NIV.
MethodsThis was a retrospective cohort study of 68 children on NIV, in whom complex OSA was the main indication for ventilation, in a Pediatric Respiratory Unit at a University Hospital between January 1997 and March 2012. Demographic and clinical data were collected on the underlying diagnosis, therapeutic interventions prior to NIV, NIV related issues and outcome.
ResultsForty (59%) children were male, median age at starting NIV was 6 years and 7 months, with interquartile range (IQR) of 15–171 months. Twenty‐two (32%) were infants and 25 (37%) adolescents.
The most common diagnosis was congenital malformations and genetic disorders in 34 (50%) patients. Nine patients had cerebral palsy, 8 were post treatment for central nervous system tumors and 6 had inborn errors of metabolism. Three children had ATH and three obesity. The majority of patients (76%) had exclusively obstructive OSA and started CPAP. Ten patients had minor complications. Twenty‐two patients stopped NIV due to clinical improvement, 8 were non‐compliant and 8 patients died. NIV median duration was 21.5 months (IQR: 7–72).
ConclusionsNIV is feasible and well tolerated by children with OSA associated with complex disorders, and has been shown to have few complications even in infants and toddlers.
A apneia obstrutiva do sono (OSA) afeta aproximadamente 1–3% da população pediátrica e está associada com uma morbidade significativa. Como a hipertrofia adenotonsiliana (ATH) é a sua principal causa, a adenocele eletiva é a primeira opção terapêutica. A ventilação não invasiva (VNI) tem sido cada vez mais considerada como uma opção, principalmente para as crianças com doenças complexas, inelegíveis, à espera de cirurgias ou após falência do tratamento cirúrgico.
ObjetivosDescrever a experiência no tratamento de crianças com OSA complexo e avaliação da viabilidade e das vantagens do NIV.
MétodosEstudo de coorte retrospetivo de 68 crianças em NIV, onde o complexo OSA foi a principal indicação para ventilação, numa Unidade Respiratória Pediátrica de um Hospital Universitário entre janeiro de 1997 e março de 2012. Os dados demográficos e clínicos recolhidos englobaram o diagnóstico subjacente, as intervenções terapêuticas prévias à NIV, as intercorrências relacionadas com a NIV e a evolução clínica.
ResultadosQuarenta (59%) crianças eram do sexo masculino, idade média no início da NIV foi de 6 anos e 7 meses, com intervalo interquartil (IQR) de 15–171 meses. Vinte e duas (32%) eram crianças e 25 (37%) adolescentes.
O diagnóstico mais comum foram as malformações congénitas e as doenças genéticas em 34 (50%) pacientes. Nove pacientes tiveram paralisia cerebral, 8 sequelas de pós‐tratamento para tumores do sistema nervoso central e seis sofriam de erros inatos do metabolismo. Três crianças sofriam de ATH e três de obesidade. A maioria dos pacientes (76%) sofria exclusivamente de OSA obstrutiva e iniciou CPAP. Dois doentes sofriam complicações menores. Vinte e dois doentes pararam o NIV, devido a melhoria clínica, 8 eram não‐conformes e 8 morreram. A duração média do NIV foi 21,5 meses (IQR: 7–72).
ConclusõesA NIV é uma terapia viável e bem tolerada em crianças com OSA e doenças complexas, com poucas complicações, incluíndo em bebés e crianças pequenas.
Pediatric obstructive sleep respiratory disorder has a broad clinical spectrum, from simple snoring to the most severe obstructive sleep apnea (OSA).
OSA occurs in 1–3% of children,1–3 and is defined by airway obstruction, either partial and prolonged or complete and intermittent, interfering with sleep patterns and ventilation.
Adenotonsillar hypertrophy (ATH) is the most frequent cause in children, but craniofacial malformations, as well as neuromuscular diseases and obesity have been increasingly considered.4
In childhood, OSA has important repercussions on somatic growth, the cardiovascular system and neurocognitive development.5–7 Early diagnosis and intervention are essential to prevent complications and improve quality of life.8,9
Identification of clinical criteria (respiratory pauses, hard or noisy breathing or excessive daytime somnolence) and predisposing clinical conditions10 support the diagnosis of OSA, but polysomnography (PSG) is currently considered the gold standard.11,12
As the main cause of OSA in childhood is ATH, adenotonsillectomy is the most commonly recommended treatment for uncomplicated cases.10,13,14 There is, however, growing evidence of surgery failure15 and there are a significant number of children with craniofacial defects who need alternative therapies. These children represent a group with complex OSA, requiring innovative surgical and medical approaches.
In children with chronic conditions or complex OSA, NIV has been increasingly used since 1984,16,17 when surgery is contraindicated or ineffective, or as a supportive treatment until appropriate stage for surgical intervention, allowing for clinical stabilization and growth.18–20
NIV efficacy and tolerance in children have been reported in a few studies18,21,22 and clearly the experience of qualified teams with appropriate support facilities warrants high quality care.10,23,24
The main objective of this study is to describe our experience in a tertiary Portuguese pediatric center in the management of children with complex OSA, for whom noninvasive positive‐pressure ventilation was an effective therapeutic alternative.
MethodsA retrospective case series study was performed through chart review of all cases of children submitted to NIV, in which complex OSA was the main indication for ventilation. Eligible cases were identified from internal clinical database in the period of January 1997 to March 2012. Children with other indications for NIV were excluded.
Demographic data were collected, including primary and secondary clinical diagnoses, sleep studies results, modes of ventilation, adherence, complications and efficacy related to NIV. Clinical data concerning sleep disordered breathing including difficult or noisy breathing, respiratory pauses, unsettled sleep, excessive sweating, excessive daytime somnolence, morning headache and failure to thrive were assessed.All patients underwent sleep studies: continuous transcutaneous monitoring of O2 and CO2 (Tc CO2), complemented with capillary blood gases from the begining through 2004, on an inpatient basis, formal sleep studies at the sleep laboratory (cardio‐respiratory studies (CRS) from 2004 and PSG after 2008).
OSA was diagnosed based on clinical signs of sleep disordered breathing as described ahead and, whenever available, by an apnea/hypopnea index (AHI)≥1.
OSA plus hypoventilation syndrome was considered when there was hypoventilation associated to obstructive events (Tc CO2median>45mmHg or morning p CO2>45mmHg).
For PSG and CRS, average saturation and AHI were collected. An AHI≥1/h was considered abnormal.
In this study NIV was defined as any noninvasive ventilatory support delivered by flow generators suitable for ambulatory use, whenever CPAP or bi‐level positive airway pressure (BiPAP) was applied. The decision on ventilatory modality relied on the presence of isolated OSA or associated hypoventilation, CPAP was the choice in the former cases and BiPAP in the latter. BiPAP was also used in isolated OSA to increase tolerance when high pressures were needed.
In all patients NIV was started in the pediatric respiratory ward or in the pediatric sleep laboratory, depending on the clinical status of the patient and availability. In the ward, pressures were progressively increased until elimination of snoring and improvement in the respiratory pattern and pulse oximetry. In the laboratory, the pressures were titrated according to international guidelines.11–13 In both settings the initial pressure was always above 4cm H2O and resulted in the elimination of respiratory events and normalization of pulse oximetry, TcCO2 and morning blood gases.
Families and patients underwent training in mask fitting, equipment management and adverse effects prevention. Their ability to maintain NIV at home was evaluated. A 24‐h phone number was available for additional information. A first follow‐up appointment was booked for 2–3 weeks after starting following NIV.
Adherence to treatment was evaluated by subjective estimation of daily NIV hours, based upon information provided by caregivers registered in the clinical file. Adherence was classified as insufficient where the NIV time was less than 3hours per night.
The recording and analysis of data were performed on SPSS® statistics for Windows®, version 19.0©. Quantitative absolute and relative data are expressed as mean and standard deviation or median and interquartile range (IQR) for data not normally distributed.
ResultsDuring the study period, 68 children with OSA started NIV, representing 41.2% of all the pediatric patients under NIV program at the Pediatric Respiratory Unit.
Forty (59%) patients were male, median age at starting NIV was 6 years and 7 months (IQR: 15–171 months).
Two main age distribution groups were identified, 22(32%) infants and 25 (37%) adolescents (Fig. 1).

A progressive increase in the number of patients entering the program yearly was found, with 61.7% of them starting NIV in 2005 or later (Fig. 2).

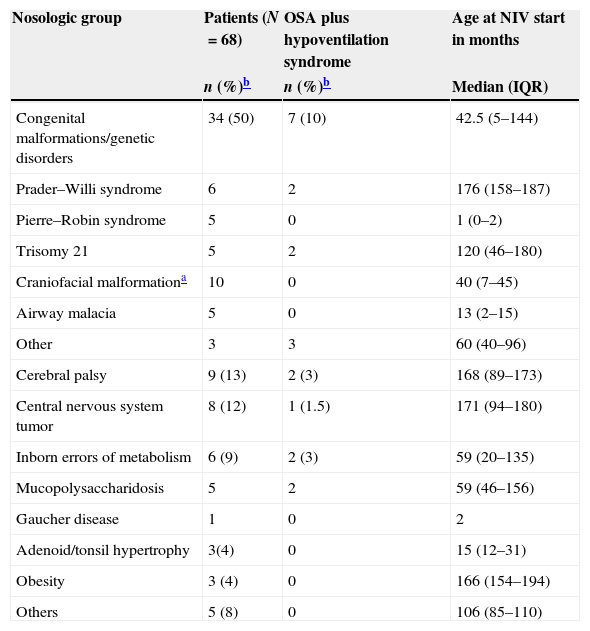
The most frequent diagnoses were congenital malformations and genetic disorders in 34 (50%) patients, cerebral palsy in 9 (13%) and inborn errors of metabolism in 6 (9%). Eight (12%) patients were referred to the center because of OSA after treatments for central nervous system (CNS) tumors. Obesity and ATH were found as a primary diagnosis for 3 patients each (4%). The complete distribution of the pathologies is illustrated in Table 1.
Distribution of patients according to primary diagnosis, presence of associated hypoventilation and age at NIV start.
| Nosologic group | Patients (N=68) | OSA plus hypoventilation syndrome | Age at NIV start in months |
|---|---|---|---|
| n (%)b | n (%)b | Median (IQR) | |
| Congenital malformations/genetic disorders | 34 (50) | 7 (10) | 42.5 (5–144) |
| Prader–Willi syndrome | 6 | 2 | 176 (158–187) |
| Pierre–Robin syndrome | 5 | 0 | 1 (0–2) |
| Trisomy 21 | 5 | 2 | 120 (46–180) |
| Craniofacial malformationa | 10 | 0 | 40 (7–45) |
| Airway malacia | 5 | 0 | 13 (2–15) |
| Other | 3 | 3 | 60 (40–96) |
| Cerebral palsy | 9 (13) | 2 (3) | 168 (89–173) |
| Central nervous system tumor | 8 (12) | 1 (1.5) | 171 (94–180) |
| Inborn errors of metabolism | 6 (9) | 2 (3) | 59 (20–135) |
| Mucopolysaccharidosis | 5 | 2 | 59 (46–156) |
| Gaucher disease | 1 | 0 | 2 |
| Adenoid/tonsil hypertrophy | 3(4) | 0 | 15 (12–31) |
| Obesity | 3 (4) | 0 | 166 (154–194) |
| Others | 5 (8) | 0 | 106 (85–110) |
Comorbidities were present in 38 (56%), gastro‐esophageal reflux (GER) in 17, obesity in 13, rhinitis in 7 and asthma in 5 patients. Some patients had association of comorbidities.
In 52 (76%) patients respiratory sleep disorders were considered exclusively obstructive and CPAP was prescribed.
Sixteen patients (24%) started on bilevel NIV, in four to increase tolerance when high pressures were needed to surpass the airway obstruction and in twelve patients because of mixed ventilatory conditions (OSA plus hypoventilation syndrome): 5 with secondary obesity (2 Prader–Willi, 2 trisomy 21, 1 CNS tumor) and the rest because of significant hypotonic disorder or restrictive respiratory pattern.
In all patients the interface for positive pressure delivering was nasal mask or prongs.
NIV was started electively in 42 (62%) patients and in acute setting in 26 (38%) after respiratory exacerbation or as transition from invasive ventilation, most transferred from Pediatric or Neonatal Intensive Care Units.
NIV was started without previous ear, nose and throat (ENT) or craniofacial surgery in 55 (81%) patients. Nine of them had surgery during follow‐up, and after intervention it was possible to stop ventilation in 5. Thirteen children (19%) started NIV after ENT surgery failure.
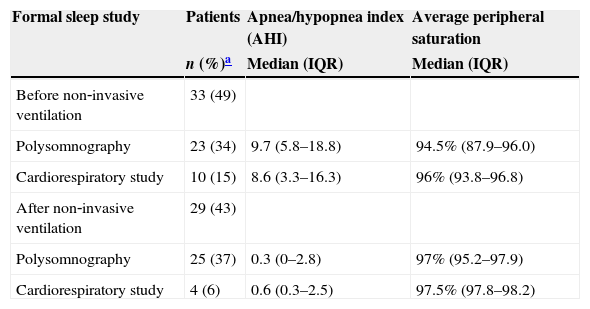
Prior to the implementation of NIV, 33 (49%) patients performed a formal sleep study (PSG or CRS). These results are shown in Table 2.
Formal sleep studies before and after NIV.
| Formal sleep study | Patients | Apnea/hypopnea index (AHI) | Average peripheral saturation |
|---|---|---|---|
| n (%)a | Median (IQR) | Median (IQR) | |
| Before non‐invasive ventilation | 33 (49) | ||
| Polysomnography | 23 (34) | 9.7 (5.8–18.8) | 94.5% (87.9–96.0) |
| Cardiorespiratory study | 10 (15) | 8.6 (3.3–16.3) | 96% (93.8–96.8) |
| After non‐invasive ventilation | 29 (43) | ||
| Polysomnography | 25 (37) | 0.3 (0–2.8) | 97% (95.2–97.9) |
| Cardiorespiratory study | 4 (6) | 0.6 (0.3–2.5) | 97.5% (97.8–98.2) |
IQR: interquartile range.
The median duration on NIV (data from 62/68 patients) was 21.5 (IQR: 7–72) months. Thirty (44%) patients are still on NIV. In 22 (32%) NIV was successfully withdrawn, 17 (77%) of which due to spontaneous resolution of clinical condition and 5 after relevant surgery. Eight patients (12%) died as result of their main diagnosis: CNS tumor,3 mucopolysaccharidosis,2 Prader–Willi syndrome,1 cerebral palsy1 and tongue sarcoma.1 Eight patients (12%) were lost to follow‐up.
According to information provided by the parents, subjective evidence of adherence was considered good in 53 (78%) children. No objective measures of adherence were applied.
Minor complications of NIV were recorded in ten (14.7%) patients: local skin irritation was reported in 3, conjunctivitis in 4 and skin breakdown in 3. In two (3%) slight facial deformation was found.
All patients with sustained NIV had clinical improvement, as reported in clinical files.
Twenty‐nine (43%) patients performed PSG or CRS after the implementation of NIV, in order to monitor their response to treatment. The results are shown in Table 2.
DiscussionOur study shows, as other series have done,24–27 that OSA is a common indication for NIV in pediatric patients. This therapeutic support has been increasingly used in selected pediatric populations, as our data also confirm, with most of the patients (61.7%) starting NIV in 2005 and thereafter.
There was a wide age range distribution for starting NIV, clearly related to the different timings of ventilation support needed for different disorders. We found a significant number of infants, being about a third of the patients. In this age group airway malacia and Pierre–Robin syndrome were the most frequent diseases found, usually with transient NIV and a good prognosis. This emphasizes the fact that NIV is being increasingly used in small children, with good tolerance and efficacy8,22,28 allowing somatic growth to occur and in some cases avoiding tracheostomy.29As described in other series, we verified a slight male predominance (58.8%).30,31
Half of patients had congenital malformations or genetic disorders as the main cause of OSA. This multiplicity of diagnosis has been previously described by others,8,9,23,24 the most relevant features being craniofacial malformations and airway malacia. The reason for opting for NIV in these complex patients is easily understood, as most of these disorders have several simultaneous factors contributing to OSA, as well as isolated adenoid hypertrophy, and hence have suboptimal results or no indication for surgical approach. The accumulated experience with this heterogeneous group of patients depends on the specificity of our institution, a tertiary university hospital, where a multidisciplinary approach is possible and often warrants support for these complex patients with multiple medical needs. CPAP is very helpful in isolated OSA, improving the quality of sleep, daytime functioning and caregiver concern32 but BiPAP is preferred when there is associated hypoventilation. As described before,32 the main benefits obtained in these patients could be different from otherwise healthy children and focused on palliation of symptoms and quality of life improvement, for patients and their families.
Three patients had isolated ATH for whom NIV was a transient support used to stabilize the patients while waiting for surgery, as described in the literature.33
Three patients were started on NIV because of primary obesity, which is increasingly associated to childhood OSA34 and often a cause of persistent OSA after adenotonsillectomy.16
Implementation of CPAP effectively controlled OSA in 52 patients. In the rest, BiPAP was started. Both forms are effective in pediatric OSA,35 and the option is determined by the existence of an OSA plus hypoventilation syndrome or the need for high ventilatory pressures.
Comorbidities, present in more than half of our patients, either alone or in association, are relevant issues. Their identification and treatment are essential because they can interfere with therapeutic choices, adhesion and adverse events of treatment.36 Obesity is the main cause of OSA in adult population, and it also plays a relevant role in childhood OSA, often being responsible for failure to respond to surgical treatment in children without other contributing factors.37 As shown in this series, overweight children and adolescents are a relevant group, including simple and secondary obesity, and in both situations a dietary plan should be part of the therapeutic approach.38
GER or rhinitis must be actively sought and should be medically controlled. Specifically the treatment of allergic rhinitis is an adjuvant measure in controlling AOS,38 and rhinitis can also interfere with NIV compliance, worsening nasal obstruction and mucosal dryness, frequent side effects associated to NIV.
The gold‐standard for OSA diagnosis is the PSG. However, if not readily available, alternative tests like pulse oximetry11 may be indicated. This was the method used in our setting until 2004. From this date on, the existence of CRS and later, of PSG (from 2008) have allowed for a more accurate monitoring for NIV management.
The reason why less than half of the patients33 performed a formal sleep study before implementing NIV (23 PSG and 10 CRS), besides availability, is due to a significant number of children starting treatment in a respiratory exacerbation and hence without previous studies.
In fact in our population NIV was started in a non‐elective manner in 38% of patients, who needed this support to deal with critical OSA and impending respiratory failure.
After starting treatment, clinical improvement was recorded in every child, and withdrawal was feasible in 22 (32%). Over a third (43%) of our population performed a formal sleep study to monitor their response to treatment.
Unlike other pediatric groups with NIV indication, such as neuromuscular patients, some patients with OSA are expected to improve as the result of somatic growth or surgery (when NIV is used as a temporary bridge to the procedure).22
In four of the eight deceased patients, with oncologic diseases, NIV was started to control OSA and also as a palliative measure, improving comfort and decreasing hospital stay. Even if it was not initially the main objective, these patients benefited from greater clinical stability, reducing the burden for themselves and their families. In the pediatric setting, we have to consider NIV as part of a palliative care plan, in which the objective is not the cure but the preservation of comfort and decreasing suffering for both the patient and the family.9,23,39
Adherence to treatment is an important issue in the assessment of NIV in children being closely related to the acceptance and tolerability of the mask and to early detection of minor skin lesions.40 A careful mask fitting was carried out with the patients, allowing them to choose the most comfortable.
Another very important issue on adherence to treatment is education. Families require appropriate training to be able to provide care for the child at home,41 so teaching the caregivers (and when possible, the child) about practical issues, main goals and consequences of withdrawal of the treatment are essential for the success of NIV. The adherence was considered good in over two thirds of our population, but objective measurements of adherence were lacking; hence the data cannot be accurately interpreted.
We registered an abandon rate of 12%, which we considered high, but still lower than that described in the literature. Marcus et al.42 demonstrated that both methods (CPAP and BiPAP) are highly effective, but over a third of their patients had abandoned treatment at 6 months follow‐up.
The main limitation of our study is its retrospective design, which limited the availability of some data and prevents a uniform approach for each patient.
ConclusionThis study described a complex group of patients, in whom NIV was used as an option to treat OSA. We demonstrated its feasibility with a high success rate, documented few complications, and found this treatment to be well‐tolerated and effective in the management of OSA, even in toddlers. As other groups have already shown, the optimal care for these patients can only be given in qualified specialized centers23,24 because the management of these complex patients requires an holistic understanding of the diagnosis, technology involved in diagnosis and therapy, prognosis and long‐term care.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.


