



Istanbul has the highest incidence of tuberculosis (TB) in Turkey. It is also the largest city, with considerable differences in quality of life across its urban regions. The aim of this study is to investigate the relationship between (i) the diverse quality of life across specific urban regions, (ii) TB incidence rates, inclusive of demographic and clinical characteristics of TB patients, and (iii) adverse treatment outcomes.
MethodsThis retrospective study included 23,845 new TB patients (recorded in the National TB Registry between 2006 and 2010) in Istanbul. Thirty-nine urban districts of Istanbul were ranked into five groups on the basis of an urban quality of life index. Patient data were matched with these groups, and further categorized according to ‘age’, ‘sex’, ‘country of birth’ and ‘antibiotics resistance’. Adverse treatment outcomes and TB incidence rates were extracted from official records. Logistic regression, clustered analyses, 95% CI and p values (STATA) were reported to describe the association between variables.
ResultsSix per cent of total cases had ‘at least one adverse treatment outcome’ (default 3.8%, failure 0.5%, death 1.7% in total cases). ‘An adverse treatment outcome’ was found to be associated with age OR (CI 95%) (1.02 (1.01–1.03)); ‘male sex’ 1.65 (1.28–2.12); ‘other country of birth’ 4.82 (3.05–7.62); 100,000 per ‘over 60’ insidence goups 1.61 (1.32-1.97), the lowest quality of life index 0.65 (0.47-0.83).
ConclusionsPatients with high tuberculosis risk factors living in high incidence regions need to be closely monitored. Patients living in lower ranking regions are more likely to have ‘poor treatment outcomes’.
Istambul tem a mais elevada incidência de tuberculose (TB) na Turquia. É igualmente a sua maior cidade, com diferenças consideráveis na qualidade de vida ao longo das suas regiões urbanas. O objetivo deste estudo é investigar a relação entre i) as diversas qualidades de vida ao longo de regiões urbanas específicas, ii) taxas de incidência de TB, incluindo as características demográficas e clínicas dos doentes, e iii) resultados adversos do tratamento.
MétodosEste estudo retrospetivo incluiu 23.845 novos doentes com TB (registados no Registo Nacional de TB, entre 2006-2010) em Istambul. Os trinta e nove distritos urbanos de Istambul foram classificados em 5 grupos com base no índice de qualidade de vida urbano. Os dados dos doentes foram correspondidos com estes grupos e subsequentemente divididos por categorias de acordo com a «idade», «sexo», «país de nascimento» e «resistência a antibióticos». Os resultados adversos ao tratamento e as taxas de incidência de TB foram retiradas dos registos oficiais. Regressão logística, análises agregadas, valores de CI e p de 95% (STATA) foram usados para descrever a associação entre variáveis.
ResultadosSeis por cento do total de casos tiveram pelo menos um resultado adverso do tratamento (padrão 3,8%; insuficiência 0,5%; morte 1,7% do total de casos). «Um resultado adverso do tratamento» foi considerado como estando associado à idade (CI 95%) (1,02 [1,01-1,03]); «sexo masculino» 1,65 (1,28-2,12); «outro país de nascimento» 4,82 (3,05-7,62); 100.000 por grupos de incidência com «idade superior a 60 anos» 1,61 (1,32-1,97), o índice de qualidade de vida mais baixo 0,65 (0,47-0,83).
ConclusõesOs doentes com altos fatores de risco de tuberculose em regiões de elevada incidência precisam de ser monitorizados de forma mais assídua. Os doentes que vivam em regiões de classificação inferior têm maior probabilidade de ter «maus resultados do tratamento».
Even though affordable and effective treatment is available, tuberculosis is still the cause of millions of cases of active disease and deaths worldwide. In 2011, 8.7 million new cases of active tuberculosis (13% of which involved co-infection with the human immunodeficiency virus [HIV]) and 1.4 million deaths, including 430,000 deaths among HIV-infected patients were recorded.1 In the 1900s, the epidemic of TB that affected Northern industrialized countries was mainly related to social, economic, and environmental factors, chiefly increasing population density and urbanization. The current epidemic, however, which mainly affects developing countries, appears to result from the combination of pre-existing socio-economic determinants with new factors such as HIV, the rise of antimicrobial drug resistance and possibly more infectious strains.2–4
The quality of life index is determined by the relationship between objective and subjective factors of environmental and biological states, levels of education and health care facilities.5 Istanbul is a cosmopolitan city and has the highest tuberculosis incidence rate in Turkey (44.1 per 100,000 population). There is a distinct difference in the quality of life index across different regions of the city. There are many factors associated with ‘adverse treatment outcomes’ such as ‘male sex’, low socio-economic status, limited access to transportation, distance from home to treatment facilities, poor treatment compliance, limited interest in information about the disease and its treatment, presence of co-morbidity, no follow-up of treatment by medical staff, low income, alcohol abuse, previous default, and HIV co-infection.6–12
The aim of this study is to investigate the relationship between the diverse quality of life across specific urban regions, TB incidence rates, inclusive of demographic and clinical characteristics of TB patients, and adverse TB treatment outcomes in Istanbul.
MethodsThis retrospective cohort study included 23,845 new TB patients, recorded in the National TB Registry between 2006 and 2010. Patients were excluded from the study if they were currently under treatment (multidrug-resistant TB treated with second-line, non-tuberculosis mycobacteria (n=747)); had a ‘previous treatment history’ (n=2397); were ‘transfer in’ patients (n=592) or ‘transfer out’ patients (n=1694). All remaining TB patients (23,845) were included in this study.
New patients were defined as those who had ‘no previous treatment’ for TB, or who had taken anti-TB drugs for less than 1 month. New patients with pulmonary TB received a standardized short-course chemotherapy, consisting of two months of isoniazid (H), rifampicin (R), pyrazinamide (Z), and ethambutol (E), followed by four months of just HR. Patients were followed up monthly at TB dispensaries, and received TB drugs under DOTS (Directly Observed Treatment, Short-course) every day at the nearest DOTS facility.13,14
TB treatment in Turkey involves no direct cost to patients and is provided by dedicated TB dispensaries where treatment outcomes are monitored through case registries, facilitating comprehensive assessment of TB epidemiology and treatment results.
Clinical treatment outcomes are defined as: ‘treatment failure’ – a patient whose sputum smear or culture is positive at 5 months or later during treatment; patients found to harbour a multidrug-resistant strain at any point of time during treatment (smear positive or negative); ‘death’ – a patient who dies for any reason during the course of treatment; and ‘default’ – a patient whose treatment was interrupted for two consecutive months or more. In this study, clinical outcome was evaluated 12 months after commencement of treatment. Default, death, and treatment failure outcomes were grouped together as ‘adverse outcomes’.13
Research carried out by the Istanbul Chamber of Commerce in 2009, determined a ‘Quality of Life Index’, which derived from the calculation of the arithmetical mean of 7 indices, for each of the 39 regions in the study. The 7 indices were obtained from statistical data encompassing: Demographic structure (Turkish Statistics Institute); Education (The local educational authority); Health (The Public Health authority); Economy (The Chamber of Commerce Tax Office HQ, Central Bank, property market); Transportation and Accessibility (Public Transport offices); Environment (electric/gas/water boards); and Social life (The ministry of Culture and Tourism). The 39 regions were further categorized into five groups according to these indices (the 1st category having the highest quality of life5) which forms the basis of our study. Our patients were treated in their regional dispensary and coded according to the five groupings of the quality of life index.
TB incidence rates for specific regions in Istanbul between 2006 and 2010 were obtained from the public health directorate of Istanbul. TB regional incidence rate was grouped into three (100,000 per 20–40, 40–60, 60>). Demographic and clinical characteristics of TB patients were categorized into age groups (0–18, 18–35, 36–50, 51–65, >65); gender; country of birth (Turkey or other country); and antibiotics resistance (any resistance, HR resistance).
Statistical analysisCategorical variables were summarized using proportions. Logistic regression, clustered analyses yielding odds ratios, 95% CI and p values (STATA) were reported to describe the association between variables (specific regions and quality life index and its influence on TB incidence rate, inclusive of demographic and clinical characteristics of TB patients) and adverse treatment outcomes.
Data collectionThere are 32 TB dispensaries in Istanbul, and each collaborates with one of the two main diagnostic laboratories, subject to external quality control from the national TB reference laboratory in Ankara. The National Tuberculosis database follows the WHO country report (CISID) and case-based recording data standards (Euro TB data file). To reduce bias, 20 cases from the computerized database were randomly chosen to check against the original registry to evaluate quality of data.
Ethical approval for the study was obtained from the institutional review board of Istanbul University in accordance with the Helsinki recommendations (approval no. 2011/1543-718).
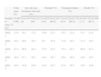
ResultsBaseline characteristics of the cases were summarized in Table 1. Of the total of 23,845 patients, 48.3% of cases were 18–35 year old, 60.4% of cases were male. 1.3% of cases were from another country of birth. 36.3% of cases were resistant to at least one drug. 38.4% of the cases occurred in areas which had over 60 incidences. The lowest rate (0.6%) of ‘other country of birth’ was found to be in the lowest quality of life group. ‘Resistance to at least one antibiotic’ varied from 42.8% to 30.5% in the QOL1 to QOL5 groupings. The lowest ‘resistance’ rate (30.5%) was found to be in the lowest quality of life group. QOL1 to QOL5 has 15.9–77% ‘over 60’ per 100,000 incidences. 77% of over those in the 60 per 100,000 incidences were in the lowest quality of life group.
Quality of life (QOL) groups, demographics and clinical characteristics of tuberculosis patients.
| Case characteristic | Total cases | QOL1 | QOL 2 | QOL 3 | QOL4 | QOL5 |
| (%) | (%) | (%) | (%) | (%) | (%) | |
| Number of cases | 23,845 | 2962 | 2461 | 10,085 | 3920 | 4417 |
| Age group | ||||||
| 0–18 | 10.0 | 11.0 | 10.4 | 12.6 | 15.8 | 19.8 |
| 18–35 | 48.3 | 46.2 | 44.8 | 48.5 | 50.5 | 49.4 |
| 36–50 | 19.6 | 21.3 | 21.1 | 20.4 | 18.1 | 17.3 |
| 51–65 | 12.0 | 13.2 | 15.5 | 12.2 | 11.1 | 9.8 |
| >65 | 6.0 | 8.2 | 8.1 | 6.4 | 4.5 | 3.6 |
| Gender | ||||||
| Male | 60.4 | 60.6 | 61.1 | 59.8 | 60.7 | 60.9 |
| Country of birth | ||||||
| Other country | 1.3 | 2.1 | 2.3 | 1.1 | 1.1 | 0.6 |
| Antibiotic resistance | ||||||
| Sensitive | 63.1 | 63.0 | 61.1 | 61.0 | 64.4 | 69.5 |
| Any resistance | 36.3 | 37.0 | 38.9 | 42.8 | 35.6 | 30.5 |
| TB incidence | ||||||
| 20–40 | 26.0 | 33.0 | 45.6 | 40.1 | 4.0 | 0 |
| 40–60 | 35.6 | 20.6 | 28.0 | 44.0 | 46.6 | 22.2 |
| 60> | 38.4 | 46.4 | 26.4 | 15.9 | 49.5 | 77.8 |
6% of total cases had ‘some adverse treatment outcome’ (default was 3.8%, failure was 0.5%, death was 1.7% in total cases). Most of the total cases (42.3%) were in QOL3. ‘Some adverse treatment outcome’ was 10.0–39.9% in the QOL1 to QOL5 groupings. The highest rate of adverse treatment was in QOL3 (Table 2).
Treatment outcomes according to quality of life indices (QOL).
| Total cases (%) | Any adverse treatment outcome (%) | Default (%) | Treatment failure (%) | Death (%) | |||||
| Number of cases, N (%) | 23,845 (100) | Yes1433 (6) | No22,412 (94) | Yes918 (3.8) | No22,927 (96.2) | Yes119 (0.5) | No23,726 (99.5) | Yes397 (1.7) | No23,448 (98.3) |
| QOL 1 | 12.4 | 14.2 | 12.3 | 14.6 | 12.3 | 15.1 | 12.4 | 13.1 | 12.4 |
| QOL 2 | 10.3 | 10.0 | 10.3 | 9.2 | 10.4 | 11.8 | 10.3 | 11.3 | 10.3 |
| QOL 3 | 42.3 | 39.9 | 42.4 | 37.5 | 42.5 | 35.3 | 42.3 | 46.9 | 42.2 |
| QOL 4 | 16.4 | 21.1 | 16.1 | 24.4 | 16.1 | 16.0 | 16.4 | 14.9 | 16.5 |
| QOL 5 | 18.5 | 14.8 | 18.8 | 14.4 | 18.7 | 21.8 | 18.5 | 13.9 | 18.6 |
‘Some form of adverse treatment outcome’ and ‘death’ were found to be significant with increasing age (1.02 (1.01–1.03), 1.07 (1.06–1.08)). Some kind of ‘adverse treatment outcome’ was found to be significant in males (1.65 (1.28–2.12)) and ‘default’ was found to be significant (2.08 (1.59–2.72)) in males. ‘Some kind of adverse treatment outcome’ was found to be significant (4.82 (3.05–7.62)) in ‘other country of birth’. Default was significant in ‘other country of birth’ 5.70 (3.76–8.62). ‘Some adverse treatment outcome’ was found to be significant (1.61 (1.32–1.97)) in ‘over 60’ for 100.000 groups and ‘default’ was found to be significant 2.66 (1.80–3.92) in ‘over 60’ for 100,000 groups. ‘Failure of treatment outcome’ was found to be significant (3.14 (1.93–5.09)) in drug resistance strains. ‘Some form of adverse treatment outcome’ and ‘default’ were found to be significantly lower in the lowest quality of life (0.65 (0.47–0.83), 0.38 (0.26–0.56)) (Table 3).
Multivariable logistic and cluster analysis for adverse treatment outcomes and effecting factors (OR (CI 95%)).a
| Any adverse treatment outcome | Default | Failure | Death | |
| Age, years | 1.02 (1.01–1.03) | 1.00 (0.99–1.01) | 0.99 (0.98–1.00) | 1.07 (1.06–1.08) |
| Female | – | – | – | – |
| Male | 1.65 (1.28–2.12) | 2.08 (1.59–2.72) | 1.57 (0.78–3.15) | 1.18 (0.78–1.78) |
| Birth in Turkey | – | – | – | – |
| Other country of birth | 4.82 (3.05–7.62) | 5.70 (3.76–8.62) | 2.83 (0.91–8.75) | 1.18 (0.27–5.05) |
| TB incidence (20–40) | – | – | – | – |
| TB incidence (40–60) | 1.29 (1.03–1.63) | 1.76 (1.20–2.58) | 0.68 (0.34–1.35) | 1.02 (0.40–1.61) |
| TB incidence (over 60) | 1.61 (1.32–1.97) | 2.66 (1.80–3.92) | 0.50 (0.25–1.02) | 0.78 (0.52–1.73) |
| Sensitive | – | – | – | – |
| Any resistance | 1.40 (1.15–1.71) | 1.20 (0.92–1.58) | 3.14 (1.93–5.09) | 1.12 (0.86–1.46) |
| QOL 1 | – | – | – | – |
| QOL 2 | 0.88 (0.68–1.14) | 0.79 (0.54–1.16) | 0.83 (0.42–1.61) | 1.39 (0.91–2.11) |
| QOL 3 | 0.82 (0.60–1.11) | 0.69 (0.41–1.17) | 0.82 (0.36–1.86) | 1.45 (0.96–2.02) |
| QOL 4 | 0.95 (0.59–1.53) | 0.87 (0.50–1.52) | 1.24 (0.56–2.70) | 1.18 (0.69–2.02) |
| QOL 5 | 0.62 (0.47–0.83) | 0.38 (0.26–0.56) | 2.11 (0.96–4.65) | 1.36 (0.85–2.19) |
In this study, 6% of total new cases had ‘some kind of adverse treatment or outcome’ (default was 3.8%, failure was 0.5%, death was 1.7%). ‘Death’ was found to be significant with increasing age. ‘Default’ was approximately two-fold in males and was found to be six-fold in ‘other country of birth’ category. ‘Default’ was found to be approximately three-fold in ‘over 60’ incidence for 100,000 groups. ‘Failure of treatment outcome’ was found to be three-fold in drug resistant strains. ‘Default’ was found to be significantly lower in the lowest quality of life group. The lowest ‘other country of birth’ rate (0.6%) was found to be in the lowest quality of life group. The lowest ‘resistance’ rate (30.5%) was found to be in the lowest quality of life group.
TB is almost always curable if patients are treated with effective, uninterrupted anti-tuberculosis treatment, which is crucial in controlling the spread of infection and minimizing the development of drug resistance. The rate of ‘treatment success’ for smear-positive cases treated, exceeded the WHA global target for the first time in 2007 (86% globally).15 Since 2006 (after the expansion of DOT in Turkey), ‘treatment success’ rate is continuing to improve.16 In 2008, ‘treatment success’ was achieved in 92% of smear positive new cases.16 Statistics in Turkey (2005–2008) displayed consistent reduction in ‘treatment default’ of 5.7–3.2% and reduction in ‘adverse treatment outcome’ of 19.2% between 1998 and 2000 in Istanbul.17–20 In our study, new TB cases were evaluated and the default rate (3.8%) was found to be higher than the other ‘any adverse treatment outcomes’.
Upon evaluation by systematic review,21 it was found that four major factors interact which affect adherence to TB treatment including: structural factors; poverty and gender discrimination; social context; health service factors; and personal factors. Gender differences in tuberculosis epidemiology may arise either as a consequence of differences in biological functioning or differences in the societal roles of men and women.22 In our study, ‘adverse treatment outcome’ and ‘default’ were found to be approximately two-fold in males. The increased risk of ‘adverse treatment outcome’ and ‘default’ among immigrants is recorded in ‘other country’.23,24 In our national study, ‘birth outside Turkey’ was associated with a more than five-fold increase in the odds of ‘adverse treatment outcome’.25,26 In this study, ‘birth outside of Turkey’ was associated with an approximately six-fold increase and ‘male gender’ was associated with a two-fold increase in the odds for ‘default treatment outcome’.
‘Over 60’ was strongly associated with death in an analysis of TB treatment outcomes involving 15 European Union (EU) countries.27 In our study, ‘some adverse treatment outcome’ and ‘death’ were found to be significant. International studies highlight the importance of antibiotic resistance in treatment outcomes. Espinal et al. reported increased risks of ‘treatment failure’ and ‘mortality’ among new TB cases with MDR in 6 countries in the Caribbean region, Asia, Europe, and South America.28 In recent studies carried out in Istanbul, ‘antibiotic resistance’ had the strongest impact on outcome. Patients with MDR strains had over 90-fold increased odds of ‘treatment failure’ and nearly 6-fold increased odds of ‘death’.25 ‘Any kind of resistance’ had three-fold increased odds of ‘some adverse treatment outcome’.26 ‘Failure of treatment outcome’ was found to be three-fold in drug resistance strains.
WHO has recently highlighted the importance of biological and socio-economic factors in driving the epidemic of the ‘new TB’, and studies challenge the impact of the current global strategy for the control of TB, based on case findings and treatment.29–31 Many components, such as health, adequate nutrition and protection, access to education, sexual equality and lack of negative impact, contribute to the quality of an individual's life. In this study, seven indices were utilized for determining quality of life (demographical structure, education, health, economy, transportation and accessibility, environment and social life)5 and it was found that ‘some form of adverse treatment outcome’ and ‘default’ were lower in the lowest quality of life region. Patient treatment compliance was seen to be high in the lower quality of life regions. The study also revealed that in the lowest quality of life regions, ‘resistance to at least one antibiotic’, and ‘other country of birth’ rates were lower than in the higher quality of life regions.
The strength of this study is that it was carried out in Istanbul, Turkey's largest city, with the country's highest incidence of TB. The study included all eligible patients within the city catchment area, minimizing the effect of selection bias.
The limitations of this study included: firstly, TB patients who were not detected by the national health system could not be included and although this group is small it is also likely to include marginalized groups such as the homeless. Secondly, patients were transferred out, and follow-up information was unavailable. Finally, the living conditions and socio-economic factors vary considerably according to district within the regions of Istanbul, which could not be evaluated in this study.
Significant findings in this study include a ‘treatment success’ rate of 92.8% and identification of patient characteristics associated with ‘adverse outcomes’. These findings suggest several recommendations for improving care among TB patients. Patients with characteristics of ‘advanced age’, ‘male sex’, ‘birth outside of Turkey’, prevalence of ‘antibiotic resistance’ should be considered a high risk for ‘adverse outcomes’, justifying more increased awareness and care.
Patients living in high TB incidence regions need to be monitored more closely. This study also showed that region in relation to the quality of life index could affect the TB treatment outcomes; however, for a more accurate evaluation details of the TB patient's specific district of abode and living conditions, within the regional category, need to be taken into account.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThis work was conducted without funding support.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank the American Thoracic Society and the Turkish Thoracic Society for their sponsorship of the Methods in Epidemiology, Clinical, and Outcomes Research (MECOR) course, as well as Mary Ann, Diana Buist, MD MPH, a member of the MECOR faculty, from which this study was conceived and developed. We also thank the patients and staff involved in the Istanbul TB programme.


