

The modulation of adenosine receptors has been proposed as new therapeutic target for chronic obstructive pulmonary disease, but studies in humans were negative. Caffeine is widely consumed and acts by non-selective modulation of these receptors, allowing for a non-interventional evaluation of the purinergic effects on COPD. We evaluated the effects of chronic caffeine consumption on the risk for COPD exacerbations.
MethodsRetrospective study including patients with COPD. The total number of exacerbations during a three-year period and the mean daily caffeine consumption in the last twenty years were evaluated. A univariate and multiple regression analysis were performed for evaluation of the significant predictors of exacerbations.
ResultsA total of 90 patients were included. Most were males (82.2%) and had a mean forced expiratory volume in the first second (FEV1) of 57.0±17.1% predicted. The mean daily caffeine consumption was 149.7±140.9mg. There was no correlation between the mean caffeine consumption and exacerbations (p>0.05).
DiscussionOur results suggest that caffeine has no significant effect on the frequency of COPD exacerbations. These conclusions are limited by the sample size and the retrospective nature of the study.
Chronic obstructive pulmonary disease (COPD) is characterized by progressive, non-reversible airflow obstruction, leading to disability and premature death. Exacerbations are frequent episodes of increasing symptoms and inflammation, besides a major driver of morbidity and mortality from the disease. Most exacerbations are caused by bacterial/viral infection or exposure to pollutants. Importantly, some patients seem to be especially prone to exacerbations (frequent exacerbator phenotype), and each episode increases the risk for a new one. COPD usually develops as a late complication of cigarette smoking, with biomass and occupational exposure having smaller roles.1 The disease is highly prevalent, and the associated morbidity and mortality are growing. The World Health Organization estimates that COPD will be the third leading cause of worldwide death in 2030.2 Current treatments have no significant effects on its progression, and so new therapies are urgently needed.3
One potential new therapeutic target is the modulation of purinergic receptors, which have been shown to have potent anti-inflammatory and immunomodulatory effects.4 However, despite promising results in animal models, the clinical use of purinergic modulators in COPD has not shown efficacy, probably due to differences in receptor types and distribution among species.5
Caffeine, the most widely consumed psychoactive substance exerts its effects by non-selective antagonism of adenosine receptors.6 This allows for an estimation of the potential of adenosine receptor modulation on COPD patients, by studying the consequences of caffeine intake. Our objective was to evaluate the effects of chronic caffeine consumption on the risk of exacerbations of COPD patients.
Materials and methodsWe performed a retrospective study, including patients with COPD under follow-up at the outpatient consult of the Unit of Pneumology of an Academic Hospital in Portugal. The inclusion criteria were a diagnosis of COPD according to international guidelines1 and performance of at least one post-bronchodilator spirometry in the three previous years. The exclusion criteria were a diagnosis of another pulmonary or systemic inflammatory disease, asthma, pregnancy and non-consent. Patients were selected from the outpatient clinics database and contacted by telephone. After oral consent was given, a standardized questionnaire was applied. The purpose of the interview was the estimation of mean daily caffeine consumption in the last twenty years, and the number of exacerbation in the last three years. Patients were questioned about the mean daily consumption of the main dietary caffeine sources: espresso=100mg, instant coffee (cup)=60mg, decaffeinated coffee=3mg, tea (leaves, herbs or berries)=30mg, instant tea (cup)=20mg, cola-drinks (300ml can or bottle)=18mg.7 The average daily consumption of caffeine was calculated by multiplying the amount of caffeine content in each source by its mean daily consumption. An exacerbation was defined as a period of worsening symptoms leading to urgent medical evaluation. The subjects were also asked about their demography, habits and clinical history, including comorbidities. The questions about comorbidities focused on hypertension, stroke and peptic ulcer disease as the study investigators considered that these diseases could impact caffeine consumption. Patient's clinical files were reviewed for data on COPD diagnosis and lung function tests.
The statistical analysis was performed using the STATA software package version 13.1 (StataCorp, USA). The continuous variables were characterized using measures of central tendency (mean) and distribution (standard deviation), and the categorical variables were characterized using proportions. The group differences in quantitative variables were tested with Student's t test for independent variables or Wilcoxon rank-sum test, according to normality, as tested by Shapiro–Wilk. For more than two groups, ANOVA or Kruskal–Wallis was used. The correlations were tested using Pearson or Spearman coefficient, depending on normality. The relationships between categorical variables were tested using chi-square. For the analysis of the effect of caffeine consumption on the frequency of exacerbations, a multiple regression model was built using a step-down procedure. A p-value<0.05 was considered statistically significant. The sample size was also calculated using STATA. For a power of 0.8 and α-value of 0.05, a sample of 85 individuals was necessary to test for a correlation of 0.3 between caffeine consumption and exacerbation rate.
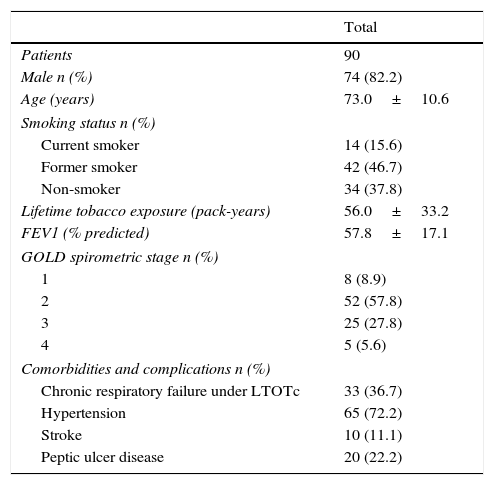
ResultsAn initial sample of 100 patients was contacted but 10 were excluded due to an alternative diagnosis (8) or concomitant systemic inflammatory disease (2). Our final sample included 90 patients. The demographical and clinical characteristics of the study population are described in Table 1. Patients were predominantly male, with a mean age of 73.0±10.6 years. The majority were smokers (15.6%) or former smokers (46.7%), with a mean of 56.0±33.2 pack years of tobacco lifetime exposure. Former smokers had quit 17.5±12.0 years before this study. Concerning COPD severity, most patients had GOLD spirometric stage 2 disease, with a mean forced expiratory volume in the first second (FEV1) of 57.8±17.1% predicted. A significant proportion (36.7%) were on long term oxygen therapy (LTOT). Comorbidities were common, including hypertension in 72.2% and stroke in 11.1% of patients. When comparing genders, we found differences in smoking history (31.3% of smokers or former smokers in females vs 68.9% in males, p<0.01, chi square), and oxygen therapy (68.8% in females vs 29.7% in males, p<0.01, chi-square). There were no other significant differences between genders in demographical or clinical features.
Demographical and clinical characteristics of the study population. Values are expressed as mean±standard deviation. FEV1: forced expiratory volume in the first second (% predicted); GOLD: global initiative for chronic obstructive lung disease (GOLD 1: FEV≥80%, GOLD 2: 50≤FEV1<80; GOLD 3: 30%≤FEV1<50%; GOLD 4: FEV1<30%).
| Total | |
|---|---|
| Patients | 90 |
| Male n (%) | 74 (82.2) |
| Age (years) | 73.0±10.6 |
| Smoking status n (%) | |
| Current smoker | 14 (15.6) |
| Former smoker | 42 (46.7) |
| Non-smoker | 34 (37.8) |
| Lifetime tobacco exposure (pack-years) | 56.0±33.2 |
| FEV1 (% predicted) | 57.8±17.1 |
| GOLD spirometric stage n (%) | |
| 1 | 8 (8.9) |
| 2 | 52 (57.8) |
| 3 | 25 (27.8) |
| 4 | 5 (5.6) |
| Comorbidities and complications n (%) | |
| Chronic respiratory failure under LTOTc | 33 (36.7) |
| Hypertension | 65 (72.2) |
| Stroke | 10 (11.1) |
| Peptic ulcer disease | 20 (22.2) |
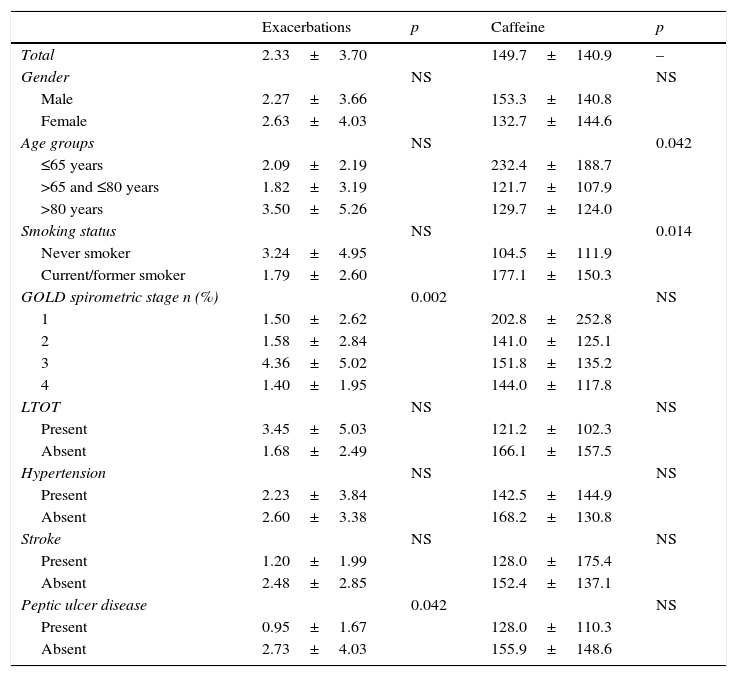
The patient's frequency of exacerbations can be seen in Table 2. Patients reported a mean of 2.33±3.70 exacerbations during the three years of the study, with 0.74±1.57 leading to admission. There was no significant correlation between age and the number of exacerbations (p=0.72, Spearman). There was also no difference regarding gender (p=0.90, Mann–Whitney), history of smoking (p=0.20, Mann–Whitney) hypertension (p=0.59, Mann–Whitney) and stroke (p=0.31, Mann–Whitney). There was a trend for higher number of exacerbations for patients under LTOT (p=0.077, Mann–Whitney), and an unexpected lower number of exacerbations in patients reporting a diagnosis of peptic ulcer disease (PUD) (mean of 0.95±1.67 vs 2.73±4.03, p<0.05, Mann–Whitney). A negative correlation was found between lung function and number of exacerbations, (rS −0.37, p<0.001, Spearman for % predicted FEV1). The analysis for exacerbations requiring admission led to similar results, except for a trend for less incidents in patients reporting history of peptic ulcer disease (p=0.054, Mann–Whitney).
Mean number of exacerbations in the last three years and mean daily caffeine consumption in the last 20 years according patient's epidemiological and clinical characteristics. LTOT: long term oxygen therapy; GOLD: global initiative for chronic obstructive lung disease (GOLD 1: FEV≥80%, GOLD 2: 50≤FEV1<80; GOLD 3: 30%≤FEV1<50%; GOLD 4: FEV1<30%).
| Exacerbations | p | Caffeine | p | |
|---|---|---|---|---|
| Total | 2.33±3.70 | 149.7±140.9 | – | |
| Gender | NS | NS | ||
| Male | 2.27±3.66 | 153.3±140.8 | ||
| Female | 2.63±4.03 | 132.7±144.6 | ||
| Age groups | NS | 0.042 | ||
| ≤65 years | 2.09±2.19 | 232.4±188.7 | ||
| >65 and ≤80 years | 1.82±3.19 | 121.7±107.9 | ||
| >80 years | 3.50±5.26 | 129.7±124.0 | ||
| Smoking status | NS | 0.014 | ||
| Never smoker | 3.24±4.95 | 104.5±111.9 | ||
| Current/former smoker | 1.79±2.60 | 177.1±150.3 | ||
| GOLD spirometric stage n (%) | 0.002 | NS | ||
| 1 | 1.50±2.62 | 202.8±252.8 | ||
| 2 | 1.58±2.84 | 141.0±125.1 | ||
| 3 | 4.36±5.02 | 151.8±135.2 | ||
| 4 | 1.40±1.95 | 144.0±117.8 | ||
| LTOT | NS | NS | ||
| Present | 3.45±5.03 | 121.2±102.3 | ||
| Absent | 1.68±2.49 | 166.1±157.5 | ||
| Hypertension | NS | NS | ||
| Present | 2.23±3.84 | 142.5±144.9 | ||
| Absent | 2.60±3.38 | 168.2±130.8 | ||
| Stroke | NS | NS | ||
| Present | 1.20±1.99 | 128.0±175.4 | ||
| Absent | 2.48±2.85 | 152.4±137.1 | ||
| Peptic ulcer disease | 0.042 | NS | ||
| Present | 0.95±1.67 | 128.0±110.3 | ||
| Absent | 2.73±4.03 | 155.9±148.6 |
We then analyzed the consumption of caffeine in our population. The detailed data on caffeine consumption from our sample can be seen in Table 2. Patients reported a mean daily consumption of 149.7±140.9mg. There was no difference between genders (p=0.644, Mann–Whitney). Subjects with a history of smoking reported higher caffeine consumption (177.1±150.3 vs 104.5±150.3mg, p=0.014, Mann–Whitney). There was no correlation between the number of pack-years smoked and caffeine consumption (p=0.35, Spearman). Younger patients reported higher consumption (232.4±188.7 for those younger than 65 years, 121.7±107.9 for those between 65 and 80 years, and 129.7±124.0 for those over 80 years, p=0.042, Kruskal–Wallis). There were no differences in consumption between those under LTOT (p=0.345, Mann–Whitney), with a history of stroke (p=0.292, Mann–Whitney), hypertension (p=0.149, Mann–Whitney) or PUD (p=0.525 Mann–Whitney).
Finally, we examined the effects of caffeine consumption on the number of reported exacerbations in the last three years. On the univariate analysis, there was no correlation between caffeine consumption and either the total number of exacerbations (p=0.678, Spearman) or the exacerbations requiring admission (p=0.822, Spearman). On the multiple linear regression analysis, ulcer (β=−1.53, p<0.01) and FEV1 (β=0.058, p<0.05) were found to explain 11% of the variability on exacerbations (R2=0.13, F(2,87)=5.75, p<0.01). Caffeine consumption was not a significant predictor (p>0.05).
DiscussionWe report the first study evaluating the effects of caffeine consumption on the frequency of exacerbations in COPD patients. Our main finding was the lack of a significant effect of caffeine on this frequency, both before and after adjusting for major confounders. This is surprising, given that caffeine has been associated with an improved lung function in previous studies,8 and lung function is a major predictor for the risk of COPD exacerbations.9 Caffeine exerts its effects by the antagonism of adenosine receptors, potent modulators of inflammation in the lung and other organs.4,6 There is evidence that the levels of adenosine are increased in patients with COPD,10 and a number of preclinical studies suggest that adenosine receptor modulation may be an effective treatment for COPD.5
One possible explanation for these negative results is that caffeine consumption is only beneficial in non-smokers and long term former smokers. In fact, caffeine was only associated with better lung function in non-current smokers, and even former smokers who quit in the last 15 years seem to gain less from caffeine consumption than those who abandoned smoking earlier.8 Some of the suggested mechanisms for this interaction include changes in caffeine metabolism that are induced by smoking, and an enhanced inflammation in smokers overwhelming the effects of caffeine. Another explanation for our results is confounding by smoking, a common problem in health studies of caffeine and disease.11 The authors tried to overcome this with a multivariate regression analysis. COPD exacerbations may be characterized by a heightened or different form of inflammation that is resistant to the anti-inflammatory effects of caffeine, unlike stable disease. The found association between reported peptic ulcer disease and lower exacerbation rate was unexpected. In fact, previous studies have shown a positive association between PUD, worsening COPD12 and mortality.13 The 2015 edition of GOLD report recognizes that reflux is associated with an increased risk or exacerbations and poorer health status.14,15 The mechanism for this association is not fully known. Our results may be caused by the self-report nature of these data and the use of anti-reflux therapies in patients who reported PUD, whereas other subjects may have non-identified, non-treated PUD or reflux.
This study has some limitations. The retrospective nature of the study and the self-reported nature of the clinical data may have induced bias. We evaluated caffeine consumption over a period of 20 years. Although some recall bias is to be expected from this questionnaire, subjects tend to maintain stable caffeine consumption throughout the years. Other studies have successfully used a similar approach to estimate caffeine consumption in patients with Alzheimer's disease, as well as matched controls. 16 This was also a single-center study. The sample size was powered to test for a 0.3 correlation, and weaker associations may have been missed. Finally, we did not collect data on other variables that may have an influence on the risk for exacerbations, including patient's current treatment for COPD and coexistence of bronchiectasis. Some of the strengths of the study include a comprehensive assessment of the dietary sources of caffeine and a multivariate analysis for exacerbations, controlling for smoking and comorbidities.
In conclusion these results suggest that caffeine has no significant effects on the risk for exacerbations in COPD patients. These conclusions are limited by the sample size and the retrospective nature of the study. We propose that further studies of the use caffeine for COPD should focus on different clinical endpoints such as loss of lung function or quality of life.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
This study was supported by FCT, grants PIC/IC/83226/2007 and SFRH/BD/69640/2010. The authors would also like to acknowledge Sara Freitas, MD and Maria João Matos, MD for assistance in patient identification and Alexandre Mendonça, MD, PhD, for kindly providing us with the caffeine consumption questionnaire.
The following are the supplementary data to this article:


