





To examine any correlations between tumor maximum standard uptake values (SUVmax) in positron emission tomography-computed tomography (PET-CT) and homogeneous/heterogeneous tumor FDG uptake in PET-CT, and the diagnostic success of the procedure in thoracic ultrasonography (US)-guided transthoracic fine needle aspiration biopsy (TFNAB).
MethodsThe files of patients who underwent thoracic US-guided TFNAB between 2013 and 2018 were examined. Patients who underwent thoracic US-guided TFNAB and were diagnosed as having primary lung cancer were considered as the US-TFNAB diagnostic group. Patients whose disease was diagnosed as primary lung cancer using a different diagnostic method (e.g. CT-guided biopsies, fiberoptic bronchoscopy) due to a lack of diagnosis despite undergoing thoracic US-guided TFNAB were allocated to the US-TFNAB non-diagnostic group. The clinical and radiologic characteristics and PET-CT parameters of the two groups were compared.
ResultsA total of 104 patients were included in the study; 79 (76%) patients whose disease was diagnosed using US-guided TFNAB, and 25 (24%) patients whose primary lung cancer could not be diagnosed with US-guided TFNAB. The mean SUVmax value of the US-TFNAB diagnostic group was 19.5 ± 10.1, whereas it was 15.1 ± 8.9 in the US-TFNAB non-diagnostic group (p = 0.016). Whether a lesion showed homogeneous or heterogeneous FDG uptake did not effect diagnostic success (p = 0.289). SUVmax value was the only effective independent factor in the diagnostic success of the procedure (p = 0.035).
ConclusionsHigh SUVmax values in PET-CT in lung cancers may increase the diagnostic success of US guided-TFNAB procedures.
Thoracic ultrasonography (US)-guided transthoracic fine needle aspiration biopsy (TFNAB) performed on peripheral lung tumors is a diagnostic method with proven reliability and effectiveness, and has been used for a long time. Much work has been done on factors affecting the diagnostic success of US-guided TFNAB. These studies investigated the effects of factors on diagnostic success, including the size of the lesion, its internal structure, its location in thorax, the selected biopsy method such as FNAB or Tru-cut, the type of needle used, the use of color Doppler during the procedure, the type of US probe preferred for the procedure, and rapid on-site evaluation (ROSE).1–6
Studies have shown that US-guided TFNAB and computed tomography (CT)-guided TFNAB have similar diagnostic success in peripheral tumors of the lung. However, US-guided TFNAB has advantages over CT-guided procedures because it can be performed at the patient’s bedside, it is a real-time procedure, and it does not require exposure to radiation.7
Positron emission tomography (PET) is a metabolic imaging technique in which isotopes emitting positrons are used. Metabolism is rapid due to the rapid cell proliferation and increased protein synthesis in malignant tumor cells. Therefore, glucose metabolism is also increased. The uptake of 18-fluoro-labeled FDG (18F-FDG), a glucose analogue, is proportional to glucose use in malignant tissues, and FDG is taken up into the cell like glucose, but not metabolized. In these tumor cells, metabolic imaging can be performed using FDG, which is held in the cell without being metabolized.8,9 FDG uptake intensity is positively correlated with proliferative activity, cell differentiation, and the aggressiveness of tumor, and negatively correlated with prognosis.10 It is also known that necrotic areas in tumor exhibit less FDG uptake, and are regarded as false-negative areas in PET-CT images.11,12
Studies have demonstrated that in biopsies of mediastinal lymph nodes in lung cancers, high standard uptake values (SUVmax) correlated with diagnostic success of biopsy procedures, and that in the case of high SUVmax values, diagnostic success increased.13,14 When the literature was examined, no study investigating the relationship between PET-CT parameters and thoracic US-guided TFNABs performed in peripheral tumors of the lung was found. In the current study, correlations between tumor SUVmax values in PET-CT and homogeneous/heterogeneous tumor (presence of necrotic component) FDG uptake in PET-CT were investigated, and the diagnostic success of the procedure was assessed in peripheral lung tumors on which we performed thoracic US guided-TFNAB.
Material and methodPatient population and demographic findingsWe used a retrospective and cross-sectional study design. We retrospectively reviewed hospital records of patients who had peripheral lesion localization in the lung parenchyma as detected using thoracic US due to its contact with visceral pleura, and had undergone thoracic US-guided TFNAB in the US unit of our Chest Diseases Clinic between January 2013 and May 2018.
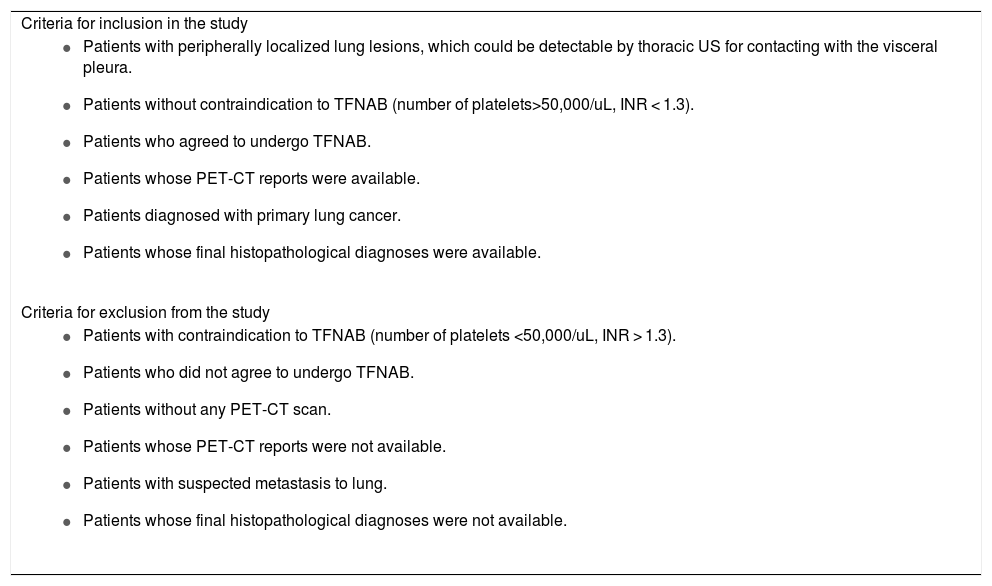
Patients who underwent thoracic US-guided TFNAB and were diagnosed as having primary lung cancer were considered as the US-TFNAB diagnostic group. Patients whose disease was diagnosed as primary lung cancer using a different diagnostic method (e.g. CT-guided biopsies, fiberoptic bronchoscopy) due to a lack of diagnosis despite undergoing thoracic US-guided TFNAB were allocated to the US-TFNAB non-diagnostic group (Table 1). The demographic findings of the patients such as age, sex, and smoking history were recorded (Table 2).
Inclusion/exclusion criteria.
| Criteria for inclusion in the study |
|
| Criteria for exclusion from the study |
|
CT: Computed tomography; PET-CT: Positron emission tomography-computed tomography; TFNAB: Transthoracic fine needle aspiration biopsy; US: Ultrasonography.
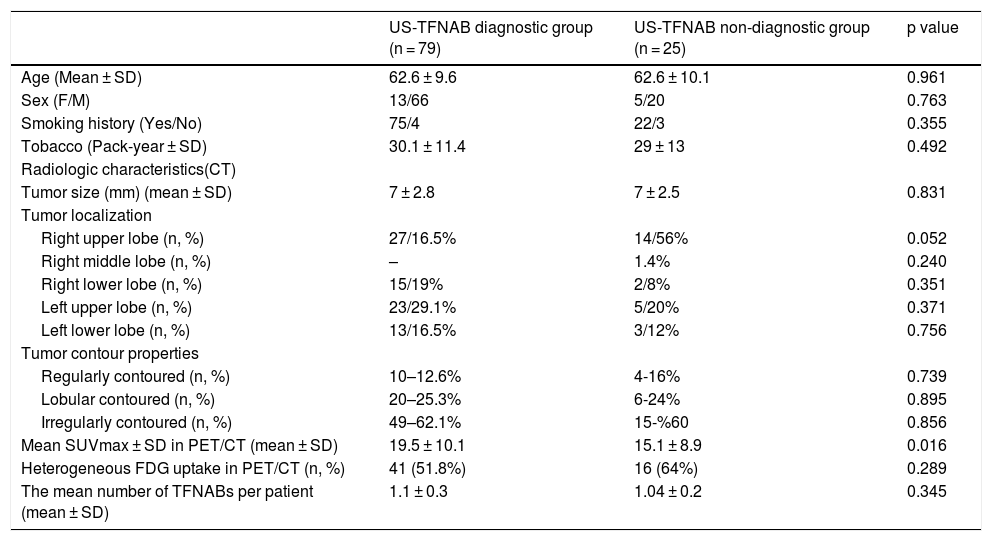
Clinical, radiologic, radiometabolic (PET/CT) features of the patients.
| US-TFNAB diagnostic group (n = 79) | US-TFNAB non-diagnostic group (n = 25) | p value | |
|---|---|---|---|
| Age (Mean ± SD) | 62.6 ± 9.6 | 62.6 ± 10.1 | 0.961 |
| Sex (F/M) | 13/66 | 5/20 | 0.763 |
| Smoking history (Yes/No) | 75/4 | 22/3 | 0.355 |
| Tobacco (Pack-year ± SD) | 30.1 ± 11.4 | 29 ± 13 | 0.492 |
| Radiologic characteristics(CT) | |||
| Tumor size (mm) (mean ± SD) | 7 ± 2.8 | 7 ± 2.5 | 0.831 |
| Tumor localization | |||
| Right upper lobe (n, %) | 27/16.5% | 14/56% | 0.052 |
| Right middle lobe (n, %) | – | 1.4% | 0.240 |
| Right lower lobe (n, %) | 15/19% | 2/8% | 0.351 |
| Left upper lobe (n, %) | 23/29.1% | 5/20% | 0.371 |
| Left lower lobe (n, %) | 13/16.5% | 3/12% | 0.756 |
| Tumor contour properties | |||
| Regularly contoured (n, %) | 10–12.6% | 4-16% | 0.739 |
| Lobular contoured (n, %) | 20–25.3% | 6-24% | 0.895 |
| Irregularly contoured (n, %) | 49–62.1% | 15-%60 | 0.856 |
| Mean SUVmax ± SD in PET/CT (mean ± SD) | 19.5 ± 10.1 | 15.1 ± 8.9 | 0.016 |
| Heterogeneous FDG uptake in PET/CT (n, %) | 41 (51.8%) | 16 (64%) | 0.289 |
| The mean number of TFNABs per patient (mean ± SD) | 1.1 ± 0.3 | 1.04 ± 0.2 | 0.345 |
CT: computed tomography; F: Female; FDG; fluorodeoxyglucose; M: Male; SD: standard deviation; SUVmax: maximum standard uptake; PET-CT: positron emission tomography-computed tomography; TFNAB: transthoracic fine needle aspiration biopsy; US:ultrasonography.
A Hitachi Pratico (Pratico, Hitachi, Japan) device was used for thoracic CT scans. The CT examinations were performed in a caudal-cranial direction with a 1-mm slice thickness and full inspiration in the supine position. The window width was 1500 Hounsfield Units (HU) for the lung window and 400 HU for the mediastinal window. The window level was −700 HU for the lung window and 10 HU for the mediastinal window. The measurements were made in the axial plane; however, coronal and sagittal images were used if necessary. Intravenous contrast agents were used for all scans except for patients with acute or chronic renal insufficiency. The radiologic findings of the patients such as tumor size, localization, and tumor contour characteristics were recorded.
Thoracic ultrasonography in peripheral lung massesIn the US unit of our clinic, thoracic US is conducted by an experienced pulmonologist using a General Electric (GE) Logic 7 device (Healthcare, Waukesha, WI, USA)and a 3.5-MHz convex probe in the abdominal mode. With the patient in a sitting position (in the supine, oblique, lateral decubitus position if needed), the entire thorax is scanned, starting from the region where the lesion has been previously observed radiologically, by moving the probe across the intercostal spaces transversely and longitudinally, along the parasternal line, the medial and lateral clavicular line, the anterior — medial and posterior axillary line, lateral and medial scapular line, and the paravertebral line.15
Thoracic ultrasound-guided transthoracic fine needle aspiration biopsy procedureIn the USG unit of our clinic, prior to biopsy procedures, a complete blood count and biochemical tests and a coagulometric test results are examined. Informed consent forms of all patients are obtained before the procedure. Patients with a platelet count of <50,000/uL and INR > 1.3, and those who do not agree to US guided-TFNAB do not undergo the procedure. Prior to thoracic US guided-TFNAB procedures, no premedication or sedation is administered. Iodine-alcohol is used to sterilize the region where the procedure will be performed and the USG probe to guide the procedure. The biopsy procedure is performed in real time using a 22-G spinal needle attached to a 20-mL injector from the pre-determined spot in which necessary measurements have been made and scanned using a power Doppler.
In all US-guided TFNAB procedures, after the hypoechoic mass lesion is detected using US, anechoic, irregular hypoechogenicities or areas observed as mixed echo-patterns in the lesion, if any, are assessed as necrotic foci. A biopsy procedure is performed by avoiding these areas.16
Integrated positron emission tomography/computed tomography findingsPatients with a fasting time of at least 8 h and a normal blood glucose level were included in the procedure. The PET-CT scans were as performed on a Philips Gemini TF ultra-speed integrated PET-CT imaging system (Philips Healthcare, Best, The Netherlands). SUV was calculated based on the ratio of the tissue radioactivity concentration and all administered doses at the time of injection divided by body weight. Patients whose PET-CT revealed different levels of FDG uptake in different areas of the tumor due necrotic areas mainly constituted by tumor cells that had lost their vitality were recorded as patients with heterogeneous FDG uptake (presence of necrotic component), and patients whose PET-CT revealed similar levels of FDG uptake across the entire tumor were recorded as patients with homogenous FDG uptake (absence of necrotic component).8,17,18 The PET-CT findings of the patients were examined. From the PET-CT reports, the SUVmax value of the main mass lesion biopsied and homogeneous or heterogeneous FDG uptake features of that lesion were recorded. Patients were excluded from the study if a PET-CT report was not available or a PET-CT scan had not been performed.
Pathologic examination histopathologic resultsWe did not have an on-site pathologist at the time of the procedures. After the cytologic specimens were prepared using both alcohol fixation and air-drying techniques, the remaining material was separated and sent in an appropriate manner to the pathology laboratory for the preparation of a cell block. In the pathology laboratory, slides fixed in 95% alcohol are stained with the Papanicolaou stain, and air-dried slides are stained with the May-Grunwald-Giemsa stain. Three-micron-thick paraffin sections obtained from the cell blocks are stained with hematoxylin andeosin. Immunohistochemical examination is applied to cell block sections in the required specimens. Patients with a definitive diagnosis of extra pulmonary cancer metastases or benign lesions and patients without a definite histopathologic diagnosis were excluded from the study.
The size of lesions detected using CT, number of TFNABs per lesion, diagnoses of patients identified using US-guided TFNAB, final diagnoses of patients whose disease could not be diagnosed using US-guided TFNAB, and final diagnosis methods were recorded. We compared the clinical, radiologic and radiometabolic (SUVmax values and homogeneous FDG uptake of the main lesion by PET-CT/heterogeneous FDG uptake) characteristics of patients between the US-TFNAB-diagnostic and US-TFNAB non-diagnostic groups.
Statistical analysisStatistical analysis was performed using the SPSS 17.0 (IBM Inc.,Relased 2008. SPSS Statistics for Windows Chicago, USA) and Med-Calc version 8.1.1.0, (Med-Calc Software, Ostend, Belgium) programs. In descriptive statistics, continuous variables are expressed as mean ± standard deviation, and categorical variables as percentage. The data of the groups were evaluated using the Chi-square and Mann-Whitney U test, and receiver operating characteristic (ROC) curve analysis.
Multivariate logistic regression analysis was conducted with variables likely to affect diagnosis in order to find independent variables that influenced the diagnostic success of thoracic US guided-TFNAB procedures. Logistic regression analysis was performed using the forward likelihood ratio method, and p < 0.05 was considered as significant.
FindingsUS guided-TFNAB procedures were conducted in a total of 167 patients in our US unit during the study period. A total of 104 patients, including 86 (82.7%) males and 18 (17.3%) females who met our inclusion criteria, were included in the study (Fig. 1). The mean age of the patients was 62.6 ± 9.6 (range, 42–84) years. Ninety-seven (93.3%) patients had a smoking history, and the average smoking story was 29.8 ± 11.8 pack-years. The most common thoracic CT finding was mass in 104 (100%) cases. The mean long axis diameter of masses and nodules detected in our patients was 7 ± 2.7(min 2, max 17) cm. An analysis of anatomic localization of masses and nodules showed that the tumor was most frequently localized in the right upper lobe in 41 (39.4%) patients (Table 2).

There were 79 (76%) patients in the US-TFNAB diagnostic group and 25 (24%) in the US-TFNAB non-diagnostic group. When the final diagnostic methods of these 25 patients (US-TFNAB non-diagnostic group) were examined, it was observed that 13 (52%) patients’ final diagnosis was achieved using CT-guided Tru-cut biopsies, 9 (36%) with fiberoptic bronchoscopy (FOB), and 3 (12%) with thoracic US-guided Tru-cut biopsies. The distribution of the final histopathologic diagnoses of the patients is given in Table 3. The mean number of TFNABs per patient was 1.09 ± 0.28.When the PET-CT reports of the patients were examined, the mean SUVmax in PET-CT scans was 19.5 ± 10.1 in the US-TFNAB diagnostic group, whereas it was 15.1 ± 8.9 in the US-TFNAB non-diagnostic group (p = 0.016) (Fig. 2). When heterogeneous FDG uptake and homogeneous FDG uptake characteristics in PET-CT of biopsied mass lesions of the patients were examined, heterogeneous FDG uptake was reported in 41 (5) patients in the US-TFNAB diagnostic group and in 16 (64%) patients in the US-TFNAB non-diagnostic group (Figs. 2a–d) (Figs. 3a–d). There was no statistically significant relationship between lesions showing homogeneous or heterogeneous FDG uptake and the diagnostic success of the US guided-TFNAB procedure (p = 0.289) (Table 2).
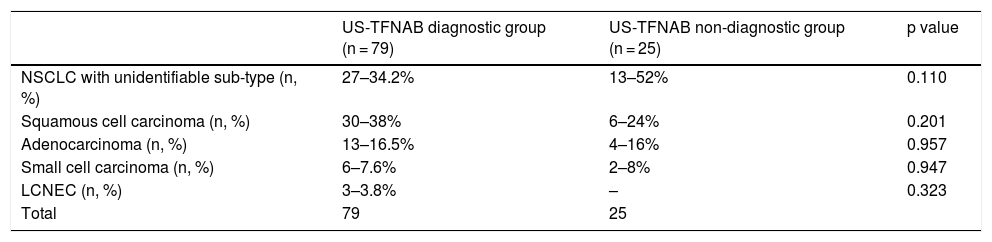
Distribution of final histopathological diagnoses.
| US-TFNAB diagnostic group (n = 79) | US-TFNAB non-diagnostic group (n = 25) | p value | |
|---|---|---|---|
| NSCLC with unidentifiable sub-type (n, %) | 27–34.2% | 13–52% | 0.110 |
| Squamous cell carcinoma (n, %) | 30–38% | 6–24% | 0.201 |
| Adenocarcinoma (n, %) | 13–16.5% | 4–16% | 0.957 |
| Small cell carcinoma (n, %) | 6–7.6% | 2–8% | 0.947 |
| LCNEC (n, %) | 3–3.8% | – | 0.323 |
| Total | 79 | 25 |
LCNEC: large cell neuroendocrine carcinoma; NSCLC: non-small cell lung cancer; TFNAB: transthoracic fine needle aspiration biopsy; US: ultrasonography.
 An approximately 5 × 5-cm mass in the left lung in thoracic CT. b) Homogeneous FDG uptake of the mass in PET-CT. c) Ultrasonographic image of the mass. d) Malignant tissue fragment (HEx400) whose structural and cellular details can be evaluated in the histopathologic preparation.")
 An approximately 15 × 10-cm mass in the right lung in thoracic CT. b) Heterogeneous FDG uptake with observed necrotic areas inside the mass in PET-CT. c) Anechoic necrotic foci in the ultrasonographic image of the same mass. d) Necrotic tissue specimen (HEx200) whose structural and cellular details cannot be evaluated in the histopathologic preparation.")
a) An approximately 15 × 10-cm mass in the right lung in thoracic CT. b) Heterogeneous FDG uptake with observed necrotic areas inside the mass in PET-CT. c) Anechoic necrotic foci in the ultrasonographic image of the same mass. d) Necrotic tissue specimen (HEx200) whose structural and cellular details cannot be evaluated in the histopathologic preparation.
The cut-off value obtained by ROC analysis made in order to determine the optimal SUVmax cut-off value in PET-CT was 10.7 (AUC: 0.661). Where SUVmax was above 10.7 in PET-CT, the sensitivity and specificity of US guided-TFNAB were calculated as 81% and 40%, respectively (Fig. 4).

When a logistic regression model was established for the variables (number of TFNABs performed, size of tumor, location of tumor, SUVmax value, presence of homogeneous/heterogeneous FDG uptake) likely to influence the diagnostic success of thoracic US guided-TFNAB, the SUVmax value was found to be the only independent factor effective in the diagnostic success of the procedure (p = 0.035, OR: 1.08, 95% CI: 1.0–1.1). The diagnostic success was not influenced by the number of TFNABs (p = 347), tumor size (p = 0.359), anatomic location of tumor (p = 0.240), or homogeneous/heterogeneous character of FGD uptake (p = 0.095).
DiscussionIn the present study, which aimed to evaluate the impact of PET-CT findings in thoracic US-guided TFNAB on diagnostic success in primary lung cancers, US-guided TFNAB allowed us to make a diagnosis in 79 of 104 (76%) patients, whereas it failed in 25 (24%) patients. SUVmax was statistically significantly lower in patients whose disease could not be diagnosed using US-guided TFNAB. Although FDG involvement was mostly heterogeneous (64%) in mass lesions in those who could not be diagnosed, no statistically significant difference was found between the type of FDG involvement (homogeneous/heterogeneous) and diagnostic success. Furthermore, SUVmax value was the only independent factor which was effective in diagnostic success of the procedure.
Glucose affinity is increased in malignant tumor cells. The main reason for increased glucose affinity is carrier proteins such as the glucose transporter (GLUT1-GLUT3), which is increased in tumor cell membranes. Previous studies reported that tumors with extremely increased GLUT 1- GLUT 3 production, hence high FDG uptake, had poor prognosis.19 It is known that tumors with high FDG uptake are metabolically more active.20 The greater the glucose affinity of the tumor, the higher the FDG uptake. Aggressive tumors with high cell differentiation and proliferative activation have high FDG uptake.10 In a study investigating the diagnostic efficiency of conventional transbronchial needle aspiration biopsies, Öztürk et al.21 established a statistically significant correlation between SUVmax values of lymph nodes in PET-CT and diagnostic efficiency (p < 0.05), and concluded that the diagnostic success of the procedure increased with high SUVmax values in PET-CT. In that study, the authors performed transbronchial biopsy on 127 lymph nodes, and reported a cut-off SUVmax value of 4.8, a procedure sensitivity of 71.7%, and a specificity of 51.4%. That study is an important study because it associates high SUVmax values with the diagnostic properties of biopsies. Studies have shown a strong correlation between tumor growth and invasion and high FDG uptake.22–24 Umeda et al.25 published a paper on the hypothesis that there might be a relationship between SUVmax and the diagnostic efficiency of transbronchial biopsies performed with virtual bronchoscopic navigation in peripheral lung lesions.25 In that study, 201 peripheral lung lesions were evaluated and it was concluded through multivariate analysis that high FDG uptake and positive bronchial signs were the only statistically significant determinants of diagnostic efficiency (SUVmax ≥2.8 OR: 3.57). Based on their results, the authors concluded that different diagnostic methods such as CT-guided biopsy or surgical biopsy, which increase diagnostic efficiency, would be more useful in lesions with low SUVmax values. In their series consisting of 140 patients who underwent transbronchial biopsies on mediastinal lymph nodes by bronchoscopy, Seijo et al.26 investigated the effects of FDG uptake in biopsies and reported that a cut-off SUVmax value of 3 or more increased diagnostic efficiency. When a cut-off SUVmax value was 3, the sensitivity of the procedure was 98% and the specificity was 45%. In that study, of 27 patients with an SUVmax value less than 3, 26 could not be diagnosed despite a sample adequacy of 74%, adequate needle passage (3.7), and adequate lymph node size (14.4 mm). The authors concluded that FDG uptake was the only and most important variable in transbronchial biopsies of malignant mediastinal lymph nodes based on multivariate analysis.
The above-mentioned studies and many similar previous studies13,14 demonstrated that a high SUVmax value in PET-CT affected diagnostic procedures in malignant diseases and the diagnostic characteristics of the procedures correlated with SUVmax values. Our study is in good agreement with these results. In our study, the diagnosis rate of thoracic US-guided TFNAB in patients with high SUVmax values was higher than in patients with low SUVmax values (p = 0.016). In multivariate regression analysis, SUVmax values were found to be the only independent factor effective in the diagnostic success of the procedure (p = 0.035). We associate this relationship with the fact that tumors with high FDG uptake are metabolically more active, more proliferative, and have more cell differentiation.10,20
The presence of various ratios of FDG uptake in various areas in PET-CT (heterogeneous FDG uptake) allows differentiation of necrotic areas, granulation tissues, and viable tumor tissues inside tumoral tissue. Clinical trials have shown that PET-CT can better assess proliferative activity in tumoral tissue and is useful in distinguishing viable tumor tissue from fibrotic tissue.27–30 In a study by Cataluna31 that evaluated factors affecting the diagnostic accuracy of bronchial biopsies, the degree of cell differentiation and the absence of necrosis in pathologic specimens were shown to be the most influential factors on diagnostic accuracy. They demonstrated that in the absence of necrosis in a pathology specimen, diagnostic accuracy was 5.2 times higher. Further, Greses et al.32 found diagnostic sensitivity to be 69.6% in their series of 151 patients, and demonstrated that one of the variables that significantly affected diagnostic accuracy in biopsy procedures was the presence of necrosis in the biopsy material. They reported that the diagnostic success was 2.6-times higher when there was no necrosis in the biopsy material. In spite of a higher rate (64%) of patients whose PET-CT revealed heterogeneous uptake due to the presence of a necrotic component than in the US-TFNAB non-diagnostic group, no statistically significant difference was found between the two groups (p = 0.289). As is widely known, US is very sensitive in the differentiation of necrotic areas in tissues.16 Necrotic areas with thoracic US are seen as focal heterogeneous echo-densities within a hypoechoic mass lesion33 (Fig. 3c). We thought that mass lesions with a necrotic component in PET-CT might negatively affect diagnostic success; however, we found no statistically significant relationship. This may be associated with the low number of patients and real-time nature of US-guided TFNABs. In real-time procedures, needle movements can be tracked within the lesion. The direction of the needle can be determined by the operator. Therefore, during biopsy, necrotic regions may be identified and biopsy of those necrotic regions can be avoided.
A limitation of our study is that it was a retrospective study conducted with a limited number of patients. It reflects experiences related to this subject from a single center; therefore, the results cannot be generalized. Another limitation is that we did not evaluate the interrater differences for thoracic US procedures and SUVmax values. Furthermore, the number of patients in some sub-groups, particularly in cancers with a relatively low FDG involvement such as well differentiated adenocarcinomas, was small. It may be worth conducting controlled studies with adequate numbers of participants in cancers with a relatively lower FDG involvement such as well-differentiated adenocarcinomas and evaluating the diagnostic role of PET-CT and US-guided biopsy in cancers with a low FDG involvement.
ConclusionWith this study, we showed that high SUVmax values in PET-CT in lung cancers increased diagnostic success of US guided-TFNAB procedures, and that a lesion with a necrotic component in PET-CT was not a factor that affected the diagnostic success of TFNAB procedures. Based on the results of this study, we believe that, in patients with low SUVmax values in PET-CT — especially in cases of urgent need for diagnosis – alternative diagnostic methods for early diagnosis should be kept in mind instead of US-guided TFNAB.
Conflict of interestCoşkun Doğan, Ali Fidan, Sevda Şener Cömert, Nesrin Kıral, Banu Salepçi, Elif Torun Parmaksız, and Benan Çağlayan and declare that they have no conflict of interest.
There are no financial or other relations that could lead to a conflict of interest
The manuscript has not been submitted to more than one journal for simultaneous consideration.
The manuscript has not been published previously, unless the new work concerns an expansion of previous work.
Ethical statementsAll procedures were conducted in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the local ethics committee.


