







The objective of this study was to review chest radiographs (CXR) and chest computer tomography (CT) findings in patients with influenza A H1N1 virus pneumonia.
Materials and methodsOf ninety-eight patients with influenza A H1N1 infections seen in the General Hospitals of Villa Scassi, Genoa, and Sestri Levante from September 2009 to December 2009, twenty-eight developed pneumonia. The initial CXR were evaluated for radiological patterns: (ground-glass, consolidation, nodules, reticulation), distribution, and extent of the disease. Chest CT scans were reviewed for the same findings. A new radiographic score (CXR score) was used to evaluate the severity of the illness.
ResultsThe predominant radiological findings on chest CT in the patients at presentation were unilateral or bilateral multifocal ground glass opacities (84.5% of the patients).
Consolidation areas had a peribronchovascular and subpleural predominance and were found mainly in the middle and upper zones of the lung. Reticular opacities were found in about 20% of the cases. The most outstanding CXR and chest CT features of the disease were basal and axial alveolar consolidation and ground-glass opacities. The severity of disease as determinate by need for mechanical ventilation was greater in patients with a greater number of lobes involved and a higher CXR score.
ConclusionBilateral ground-glass opacities and areas of consolidation were the predominant radiological findings of influenza A (H1N1) virus pneumonia. Multifocal bilateral opacities and CXR score are strictly correlated with the severity of the illness.
O objetivo deste estudo foi rever radiografias ao tórax (RXT) e tomografia computadorizada do tórax (TC) em pacientes com pneumonia pelo vírus gripe A H1N1.
Materiais e métodosDos noventa e oito pacientes com infecção pelo vírus gripe A H1N1 vistos nos Hospitais Gerais de Villa Scassi, Génova e em Sestri Levante, de setembro de 2009 a dezembro de 2009, vinte e oito desenvolveram pneumonia. Os RXT iniciais foram avaliados através de padrões radiológicos: (consolidação em vidro despolido, nódulos, reticulação), distribuição e extensão da doença. As TC do tórax foram revistas para os mesmos achados. Uma nova escala radiográfica (escala RXT) foi utilizada para avaliar a gravidade da doença.
ResultadosOs achados radiológicos predominantes na TC do tórax em pacientes na apresentação foram opacidades multifocais em vidro despolido (84% dos pacientes).
As áreas de consolidação tinham uma predominância peribroncovascular e subpleural e foram encontradas principalmente nas áreas médias e superiores do pulmão. Foram encontradas opacidades reticulares em cerca de 20% dos casos. As características mais notórias da doença na TC e RXT do tórax foram a consolidação basal e alveolar axial e as opacidades em vidro despolido. A gravidade da doença determinada pela necessidade de ventilação mecânica foi maior nos pacientes com um maior número de lóbulos envolvidos e com uma pontuação na escala RXT mais elevada.
ConclusãoAs opacidades bilaterais em vidro despolido e as áreas de consolidação foram os achados radiológicos predominantes da pneumonia do vírus da gripe A (H1N1). As opacidades multifocais bilaterais e a pontuação da escala RXT estão estritamente correlacionados com a gravidade da doença.
Influenza A viruses belong to the family Orthomyxovirus, with 16 varieties of hemagglutinin and 9 varieties of neuraminidase proteins used for subtyping. Influenza1 A pandemics occurred three times in the 20th Century: H1N1 in 1918, H2N2 in 1957, and H3N2 in 1968. H1N1 re-emerged in 1977 to periodically circulate with A (H3N2) subtypes as “seasonal flu”. A new influenza pandemic arrived in April 2009. This novel H1N1 virus was initially termed “swine origin influenza virus” but further studies revealed that it represents a quadruple reassortment of one human, one avian and two swine strains. Retrospective studies showed a virus similar to swine origin influenza virus that appeared in Thailand in 2000.2
Children and young adults are the most susceptible to this infection and high risk groups for complications are pregnant women, adults older than 65 years, children younger than 5 years, patients with underlying conditions such as chronic obstructive pulmonary disease (COPD), cardiovascular or neurological diseases, immunosuppression, hematological disorders, chronic liver diseases, chronic renal failure, metabolic diseases (especially diabetes mellitus and obesity).2,3 Although patients with conditions that confer some degree of immunosuppression, such as asplenia, should not have increased risk of influenza-associated complications, they can be at high risk of secondary invasive infections such as pneumococcal or methycillin-resistant Staphylococcus aureus pneumonia.2,3 The signs and symptoms are similar to those of “seasonal flu”, except for the fact that a greater number of subjects develop gastrointestinal symptoms.2,3 The most important complications are lower respiratory tract involvement, acute respiratory failure and acute lung injury or respiratory distress syndrome (ALI/ARDS) with refractory hypoxemia. Other severe complications include secondary invasive bacterial infections, septic shock, acute renal failure, reversible cardiac dysfunction, and the multiple organ failure syndrome. Moreover, worsening of underlying chronic diseases such as asthma, COPD or congestive heart failure may occur.2–4 Non-specific laboratory features include: elevated lactate dehydrogenase levels, lymphopenia or leucopenia or leucocytosis, thrombocytopenia and increased creatinine-phosphokinase and transaminases levels. The diagnostic test of choice is RT-PCR; samples must be collected through nasopharyngeal aspirate, or nasopharyngeal or pharyngeal swab, or, in the case of pneumonia, through the lower respiratory tract.3,5
The radiological appearance has been described in previous studies and presents similar findings, but there is a quantitative difference between cases of mild or severe illness. The predominant findings consist of ground-glass opacities or areas of consolidation, or a mixed pattern of ground glass and areas of consolidation.6 Bilateral opacities are common, with involvement of multiple lung zones. Findings in four or more zones and bilateral peripheral distribution occurred with significantly higher frequency in patients with poorer outcomes.7 The aim of this study was to review radiological findings on chest X-ray (CXR) and on chest computed tomography (CT) of influenza A (H1N1) virus-correlated pneumonia, and to evaluate whether radiological findings may be linked to clinical outcome.
Materials and methodsThe study was carried out in the Hospital of Sestri Levante and in Villa Scassi Hospital, Genoa, and was approved by the Institutional Review Board of each hospital. The subjects included 28 patients (15 males and 13 females, ranging in age from 26 to 78 years, average age 31.7±24.5) with RT-PCR confirmed influenza A H1N1 pneumonia in the period from September 2009 to December 2009.
The inclusion criteria were: patients aged 16 years or more, diagnosed of influenza A H1N1 infection and a CXR report compatible with pneumonia. The exclusion criteria were: admission to hospital in the preceding 10 days or coexistence of lung cancer or tuberculosis. The first aim of the study was to describe CXR and chest CT abnormalities of patients admitted to our hospitals with PCR-confirmed diagnosis of influenza A H1N1 virus pneumonia.
Most of our patients had a more favorable outcome (only one died), compared to previously described cases.5,8,11 The second aim was to determinate whether there were differences in radiological findings between patients who underwent mechanical ventilation and those who received only medical therapies (including oxygen therapy).
We retrospectively reviewed CXRs and chest CTs of two community hospitals in Liguria, a region of Northern Italy where our study was done. Informed patient consent was waived due to the study's observational nature. Initial CXRs were obtained in all twenty-eight patients: twelve patients had posterior–anterior projections and sixteen had both posterior–anterior and lateral projections. All radiographs were obtained using a Proteus unit (General Electrics). Chest CT scan was performed in eighteen of the twenty-eight patients within 24h of admission and in the other ten within 72h of admission.
Unenhanced HRCTs were performed with a 64-detector-row CT scanner (Somaton Sensation, Siemens Forchheim, Germany) or with a single slice helical scanner (High Speed CTi, GE Medical System, Milwaukee, WI, USA). End-inspiratory images were acquired from pulmonary apex to the diaphragm with a spiral technique (120kV, 120mA, slice thickness 1mm, pitch 1.4, ultra sharp reconstruction algorithm) on the 64-detector CT scanner, and with high-resolution axial technique (140kV, 160mA, slice thickness 1mm, interval 10mm, 1.5s acquisition time, ‘bone’ reconstruction algorithm) on the single slice scanner. CT images were displayed with a lung window (width 1800 UH, level −500) and with a mediastinal window (width 400, level 50) for evaluation. The imagining data were displayed directly on monitors of a picture archiving and communication system. CXR and the chest CT images stored in the Picture Archiving and Communications System (PACS) were examined and interpreted by two trained radiologists (with more than 20 years in CXR and CT imaging) until both reached a consensus. Each radiologist knew the diagnosis, but was blinded to all other information concerning the subjects.
Their findings were described according to the pattern of opacity: ground-glass opacity is defined as an area of hazy increased lung opacity within which definition of lung structures is usually preserved; this pattern is less opaque than consolidation. Consolidation is defined as a homogeneous increase in pulmonary parenchymal attenuation which obscures the margins of vessel and airways.7,8 Nodular opacities were defined as focal round opacities and reticular opacities were defined as linear opacities forming a web pattern.9,10 The distribution of abnormalities is categorized as focal, multifocal or diffuse.
A focal distribution was defined as a single focus of abnormality. A multifocal distribution described more than one focus, further classified as unilateral or bilateral. A diffuse distribution was defined as an abnormality is bilateral and involved an equivalent volume of one or both lungs.6,7 The anatomical distribution of radiological findings is characterized as central (from 1 to 4cm from the hila) or peripheral.7 The location of each abnormality on the CXR is divided into upper, middle or lower (based on dividing the vertical distance between the apices and the hemidiaphragmatic domes into thirds).6,7
The presence and size of pleural effusion were recorded. We have adapted a scoring system described by Opravil to grade the severity of pulmonary infiltrates in CXR: each lung is divided into four equal quadrants and each quadrant is scored on a scale of 0–3 (0: normal, 1: subtle increase interstitial markings, 2: prominent interstitial opacities, 3: confluent interstitial and acinar opacities). This system allows a maximum score of 24 for both lungs.11,12
The twenty-eight patients were divided in two groups: Group 1 consisted of ten critically ill patients admitted to ICU or to the Intermediate Respiratory Care Unit, who required invasive or non-invasive mechanical ventilation. Group 2 consisted of eighteen patients who required brief hospitalization without mechanical ventilation or vasopressor medications. A retrospective review of clinical and laboratory data was also performed to evaluate correlations between clinical, laboratory and radiological features and the severity of illness.
Statistical analysisResults are expressed as average with standard deviation and medians with quartiles for continuous variables and as frequency of occurrence of the group from which they derive for categorical variables. Regression analysis has been used to evaluate the correlation between severity and continuous variables (Age, LDH, pO2, P/F, number of lobes involved, XRC score).
Logistic regression has been used for the categorical variables to evaluate the increase of risk in the severe group versus mild group.
In both analyses p values of ≤0.05 were considered statistically significant. Statistical analyses were performed with R-Project version 2.13.2.
ResultsThere was no statistical difference between the age range of the two groups (53.8±18.2 in mild disease group versus 40.78±10.4 in severe group, p>0.058), and the predominant radiological findings in the patients at presentation were unilateral or bilateral multifocal ground glass opacities (twenty-three patients) (84.5%) (Fig. 1).
 virus pneumonia and severe respiratory failure (paO2/FIO2 at admission 180) who underwent non-invasive mechanical ventilation: chest computed tomography demonstrates patchy bilateral interstitial infiltrates and peripheral focal ground-glass opacities in the middle and lower lung zones.")
A 40-year-old man with influenza A (H1N1) virus pneumonia and severe respiratory failure (paO2/FIO2 at admission 180) who underwent non-invasive mechanical ventilation: chest computed tomography demonstrates patchy bilateral interstitial infiltrates and peripheral focal ground-glass opacities in the middle and lower lung zones.
The consolidation areas had a peribronchovascular and subpleural predominance and were found mainly in the middle and upper zones of the lung (Fig. 2). Reticular opacities were found in six cases. The most outstanding CXR and chest CT features of the disease were basal and axial interstitial-alveolar consolidation and ground-glass opacities (Fig. 3): the extent of disease was greater in Group 1 (patients requiring mechanical ventilation) with a greater number of lobes involved and a greater CXR score (p<0.001). Airway thickening and dilatation, small airway involvement with centrilobular nodules and tree-in-bud opacities was not found.
 virus pneumonia and not severe respiratory failure (PaO2/FIO2 at admission 340): chest computed tomography exhibits bilateral, patchy, confluent areas of consolidation in all lung zones.")
 virus pneumonia and severe respiratory failure (PaO2/FIO2 at admission 170) respiratory underwent non-invasive mechanical ventilation: chest computed tomography shows alveolar consolidation, peripheral ground-glass opacities in both middle and lower lung zones and small bilateral pleural effusions.")
A 39-year-old man with Influenza A (H1N1) virus pneumonia and severe respiratory failure (PaO2/FIO2 at admission 170) respiratory underwent non-invasive mechanical ventilation: chest computed tomography shows alveolar consolidation, peripheral ground-glass opacities in both middle and lower lung zones and small bilateral pleural effusions.
Predominant distribution was bilateral with involvement of lower lung zone: 21 patients presented these findings and 8 of them underwent mechanical ventilation. Patients having multifocal and bilateral distribution of opacities had a more severe course of the disease and a significantly higher frequency of mechanical ventilation (p≤0.02). Crazy-paving pattern was found in only 7 patients. The chest CT findings of the patients of our study appear in Table 1. Pleural effusions (500ml or less) were found: two patients in Group 1 and four patients in Group 2; these decreased gradually on follow-up. No evidence of hilar or mediastinal lymphnode enlargement was seen.
Radiological findings of the patients with Influenza A H1N1 pneumonia.
| Characteristics | Mechanical ventilation (10 pts) | No. mechanical ventilation (18 pts) | p-Value |
| Opacity | |||
| Ground-glass | 7 | 11 | 0.821 |
| Reticular | 3 | 3 | 0.937 |
| Nodular | 1 | 2 | 0.492 |
| Consolidation | 3 | 5 | 0.422 |
| Pleural effusion | 2 | 4 | 0.677 |
| Distribution | |||
| Focal | 1 | 3 | 0.062 |
| Multifocal | 1 | 3 | 0.268 |
| Multifocal bilateral | 8 | 5 | 0.02 |
| Diffuse | 1 | 0 | 0.110 |
| Predominant distribution | |||
| Upper lung zone | 1 | 3 | 0.121 |
| Middle lung zone | 1 | 2 | 0.234 |
| Lower lung zone | 8 | 13 | 0.039 |
Opravil et al. (modified).11,12
Higher levels of LDH, lower pO2 and pO2/FIO2 ratio at admission as well as higher number of involved pulmonary lobes and a higher XRC score were the independent variables associated with severity of illness and use of mechanical ventilation (Table 2).
Discussions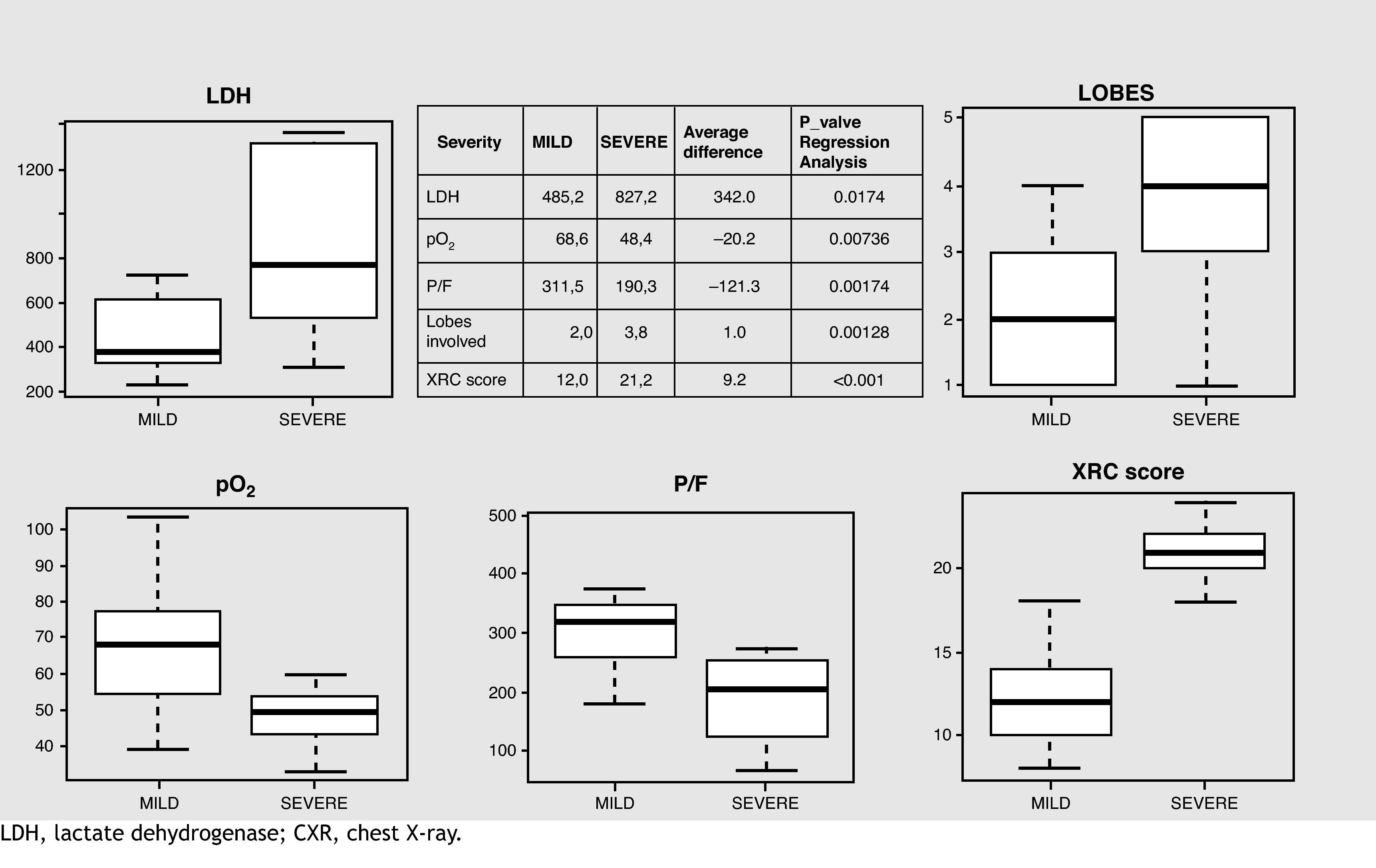
Influenza A H1N1 virus can cause either a mild influenza-type illness that is indistinguishable from seasonal influenza, or less often, a rapidly progressive, community-acquired pneumonic illness that can develop acute respiratory failure and can lead to death, most often in persons with underlying medical conditions.10 CXR is usually the first imaging test performed for the assessment of acute respiratory symptoms.
However, an increasing number of patients undergo chest CT when there is high clinical suspicion of pneumonia in the presence of normal or questionable radiological findings. Chest CT is also helpful in assessing complication or evidence of mixed infection.14 The predominant CT findings at presentation of illness were unilateral or more often bilateral multi-focal asymmetric ground-glass opacities, either alone or associated with areas of consolidation.7,13,14
The abnormalities have a predominantly peripheral and subpleural distribution: patients who exhibit consolidation on chest CT have a more severe clinical course, occasionally requiring mechanical ventilation, compared with those who present with ground-glass opacities.7,15 All the patients described originally by Perez-Padilla et al.5 had radiologically confirmed pneumonia with bilateral patchy alveolar consolidation. Subsequent studies have described ground-glass opacities, areas of consolidation and pleural effusions as the predominant computed tomography findings6,8.9 and bilateral crazy-paving.13,14
The crazy-paving pattern is a common finding on chest CT of the lungs: it consists of scattered or diffuse ground-glass attenuation with superimposed interlobular septal thickening and intralobular lines.13,14 Some authors presume that crazy-paving pattern is also closely related to an adverse course, requiring not only treatment with mechanical ventilation, but often ECMO therapy.14,16 Marchiori et al.15 have recently described high resolution computed tomography (HRCT)-pathological correlation: the predominant HRCT findings included areas of airspace consolidation and ground-glass opacities; the main pathological features consisted of diffuse alveolar damage with hyaline membrane formation, associated with various degrees of pulmonary congestion, edema, hemorrhage, inflammatory infiltration and bronchiolitis often evolving into organizing pneumonia.17
The most common chest CT abnormalities of pandemic H1N1 influenza virus infection were multifocal consolidation and ground-glass and more rarely poorly defined nodules with upper lobe predominance.18 The predominant findings in our study were bilateral consolidation and reticular opacities similar to those reported in previous literature and the predominant computed tomographic findings were ground-glass opacities and areas of consolidation.8,14,19 Multifocal bilateral distribution and Opravil CXR score were directly correlated with the severity of the illness: actually all the patients who underwent invasive or non-invasive mechanical ventilation had multifocal bilateral opacities and a higher CXR score. Secondary bacterial pneumonia usually presents a pattern consistent with bronchopneumonia, including lobular, subsegmental or segmental consolidation.20 In our case-series only one patient presented a bacterial co-infections (Staphylococcus aureus MRSA) with radiological findings of lobar pneumonia (Fig. 4).
 virus pneumonia and bacterial coinfection (Staphylococcus aureus) and severe respiratory failure (PaO2/FIO2 at admission 250). Chest computed tomography shows prominent interstitial opacity with ground-glass areas and air bronchogram.")
This study has several limitations: it is retrospective; there are a small number of patients (which results in low statistical power in our analyses). It does not present the follow-up of the patients, only their hospital courses (this may explain why organizing pneumonia was not found as a late complication of influenza A H1N1 virus pneumonia). Moreover, the study did not include children (who frequently present patchy consolidation with mediastinal lymph node, pleural effusion and pneumomediastinum) and pregnant women (who sometimes have a more severe course of illness).20,21
ConclusionsThe predominant findings in our study were bilateral consolidation and reticular opacities similar to those reported in previously and the predominant CT findings were ground-glass opacities and areas of consolidation.8,14,19,20 Multifocal bilateral distribution and Opravil XRC score were directly correlated with the severity of the illness. Furthermore, the results of the present study indicate that higher serum level of LDH or lower PaO2 and PaO2/FIO2 ratio correlated directly with lung involvement based on chest CT findings of bilateral or diffuse areas of ground-glass areas and consolidation.
These correlations were associated with severity of illness. A combination of clinical and chest CT indicators may aid in predicting the clinical course and outcome of influenza A H1N1 pneumonia.
Conflict of interestThe authors have no conflict of interest to declare.
The authors thank Giovanni Circella MD, Gabriella Bregante MD, Silvia Cantoni MD Radiological Department, Hospital of Sestri Levante, for the help in the study concept and design, and their assistance in the revision of chest X-rays and chest computed tomographies, Monica Bonfiglio MD Intensive Care Unit, Hospital of Lavagna, Alessandro Perazzo MD, Piergiorgio Gatto MD, Pulmonary Diseases Unit Hospital of Sestri Levante for the help in the data collection and Cornelius Barlascini for the help in reviewing the manuscript.


