


Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is the standard approach for lung cancer staging. However, its diagnostic utility for other mediastinal diseases might be hampered by the limited tissue retrieved. Recent evidence suggests the novel sampling strategies of forceps biopsy and cryobiopsy as auxiliary techniques to EBUS-TBNA, considering their capacity for larger diagnostic samples.
MethodsThis study determined the added value of forceps biopsy and cryobiopsy for the diagnosis of mediastinal diseases. Consecutive patients with mediastinal lesions of 1 cm or more in the short axis were enrolled. Following completion of needle aspiration, three forceps biopsies and one cryobiopsy were performed in a randomised pattern. Primary endpoints included diagnostic yield defined as the percentage of patients for whom mediastinal biopsy led to a definite diagnosis, and procedure-related complications.
ResultsIn total, 155 patients were recruited and randomly assigned. Supplementing EBUS-TBNA with either forceps biopsy or cryobiopsy increased diagnostic yield, with no significant difference between EBUS-TBNA plus forceps biopsy and EBUS-TBNA plus cryobiopsy (85.7 % versus 91.6 %, P = 0.106). Yet, samples obtained by additional cryobiopsies were more qualified for lung cancer molecular testing than those from forceps biopsies (100.0 % versus 89.5 %, P = 0.036). When compared directly, the overall diagnostic yield of cryobiopsy was superior to forceps biopsy (85.7 % versus 70.8 %, P = 0.001). Cryobiopsies produced greater samples in shorter procedural time than forceps biopsies. Two (1.3 %) cases of postprocedural pneumothorax were detected.
ConclusionsTransbronchial mediastinal cryobiopsy might be a promising complementary tool to supplement traditional needle biopsy for increased diagnostic yield and tissue harvesting.
Trial registrationChiCTR2000030373
Key messages
What is already known on this topic
Forceps biopsy and cryobiopsy are recently recognised as innovative auxiliary techniques to EBUS-TBNA for mediastinal sampling. Nevertheless, it remains unclear which of the two techniques is the superior match for standard needle biopsy.
What this study adds
Despite the similar overall diagnostic yield and safety profile, additional cryobiopsy is capable of producing greater quantity of intact mediastinal tissues while shortening the procedural duration, giving rise to increased sample suitability for lung cancer molecular testings than forceps biopsy. Cryobiopsy had an enhanced diagnostic accuracy when compared directly with forceps biopsy.
How this study might affect research, practice, or policy
Our results suggest that mediastinal cryobiopsy might be a suitable complementary approach to traditional needle sampling. Larger studies are required to further validate and broaden the findings.
For mediastinal disorders, invasive biopsy is an important diagnostic step that provides tissues for pathological and molecular evaluations. Historically, mediastinoscopy or thoracoscopy used to be considered the reference standard technique for obtaining mediastinal materials, yet endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), with its super safety profile and promising diagnostic ability has recently revolutionized this field and has become the mainstream approach.1,2 Although serving as the preferred initial tool for mediastinal staging of patients with lung cancer, one of the innate limitations of EBUS-TBNA is the restricted availability of intact tissue obtained by needle puncture, which usually suits for a cytological but not histopathological diagnostic workup, and thus might give suboptimal yields specifically in lesions of non-lung cancer aetiologies that are often more challenging to diagnose.3-5 To circumvent these limitations, other mediastinal biopsy techniques based on minimally invasive procedures have been proposed for higher accuracy. Forceps biopsy performed under real-time EBUS guidance, a relatively new technique to extract more mediastinal tissue, shows augmented sample quality and consequently improved diagnostic yield, especially in sarcoidosis and lymphoma.6
Transbronchial biopsy with a cryoprobe has been introduced over the past decade and is typically used for pulmonary parenchyma sampling in interstitial lung disease.7 This approach has proven superior to forceps biopsy in overall diagnostic yield as it provides for additional relevant pathological information due to larger samples of lung tissue without crushing artifacts.8,9 Inspired by the successful implementation of cryoprobes in the collection of lung tissue, we were the first to show that transbronchial mediastinal cryobiopsy with EBUS guidance is an equally safe while more efficient approach for the acquisition of diagnostic tissues compared to needle sampling, particularly for uncommon tumours and benign disorders.10,11 Moreover, we and other groups have previously demonstrated that both forceps biopsy and cryobiopsy offer additional diagnostic benefits to EBUS-TBNA.12,13 However, it has yet to be determined which of these two emerging techniques is more compatible with conventional needle strategy in terms of added diagnostic gain relative to added risk. Hence, the present study prospectively evaluated the added value of transbronchial mediastinal cryobiopsy versus forceps biopsy as an adjunctive approach to standard EBUS-TBNA for the diagnosis of mediastinal diseases, with diagnostic yield and procedure-related adverse events as the primary outcomes.
MethodsFor the details of the study protocol please see Supplement.
Study designWe designed a randomised trial assessing the clinical value of complementary forceps biopsy and cryobiopsy in patients with mediastinal lesions. Eligible participants were randomly assigned to receive EBUS-TBNA followed by either forceps biopsy first or cryobiopsy first and subsequently the respective complementary technique with a distribution of 1:1. The study protocol was approved by the research ethics committees of the participating centres, and had been registered at the Chinese Clinical Trial Registry (ChiCTR2000030373). All participants provided written informed consent before bronchoscopy.
ParticipantsPatients over 15 years of age with at least one mediastinal lesion (1 cm or more in the short axis) referred for diagnostic bronchoscopy to the Thoraxklinik Heidelberg or Xinqiao Hospital, respectively, were eligible to enter the trial. The sample size was estimated based on the results of our prior trial and the largest prospective study of EBUS-forceps biopsy, which indicates a 17.4 % increase in the diagnostic yield of cryobiopsy over forceps biopsy for the major mediastinal diseases.12,14 Accordingly, to achieve 90 % power at a type I error rate of 0.05, a sample size of at least 76 patients per study group was needed.
ProceduresIn all participants, mediastinal endosonographies were performed by a skilled bronchoscopist using a dedicated bronchoscope (BF-UC260F-OL8 or BF-UC260F, Olympus, Tokyo, Japan). In brief, patient airways were first endoscopically and ultrasonographically examined. Once identified by EBUS, the location, size, and blood supply of the suspected nodes were recorded. Next, needle aspiration (four passes) was performed as specified below, follow by three forceps biopsies and one cryobiopsy in random order. Bronchoscopic procedures were performed as previously described.11,15 The pathologic specimens were obtained and further evaluated by pathologists that were unaware of the patient enrollment for a clinical trial.
OutcomesThe primary end-points of this trial were first, the diagnostic yields of mediastinal cryobiopsy and forceps biopsy as either a supplementary approach to standard needle aspiration or as an individual biopsy technique, which was defined as the percentage of patients for whom mediastinal biopsy provided a definite diagnosis, and second, EBUS procedure-related adverse events such as airway bleeding, pneumothorax, pneumomediastinum, or mediastinitis.
Statistical analysisCategorical variables were presented as counts and percentages, and continuous variables were presented as mean and standard deviation (SD). Statistical analyses were performed using PASW Statistic 21 (IBM Corp., Armonk, NY). Pearson's chi-square or Fisher exact test was used to compare proportions, as appropriate. For continuous data, differences between groups were determined using Student´s t-test or Mann-Whitney U test for parametric or non-parametric data, respectively. P<0.05 was considered statistically significant. All reported P values were two-sided.
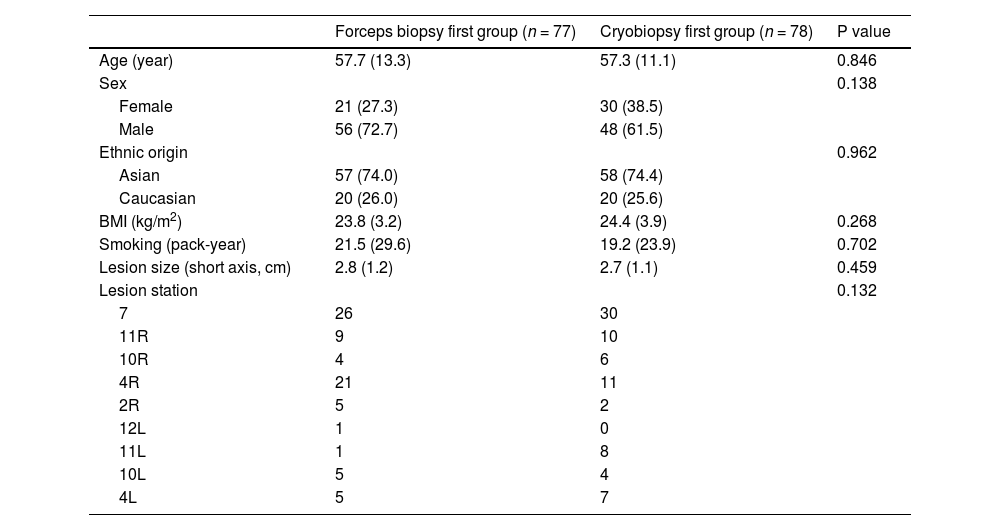
ResultsPatient characterizationBetween October 2021 and April 2022, 155 consecutive patients [40 (25.8 %) at Thoraxklinik Heidelberg, 115 (74.2 %) at Chongqing Xinqiao Hospital] with mediastinal lesions requiring diagnostic bronchoscopy were enrolled and randomised (Fig. 1). EBUS procedures under moderate sedation were well-tolerated by all patients, and each biopsy was technically successful. One (0.6 %) participant from the cryobiopsy first group declined all further investigations post-discharge, and was hence excluded from the diagnostic yield analyses. Baseline characteristics of patients in each trial group are shown in Table 1.

Baseline characteristics.
Data are mean (SD) or n (%). BMI, body mass index.
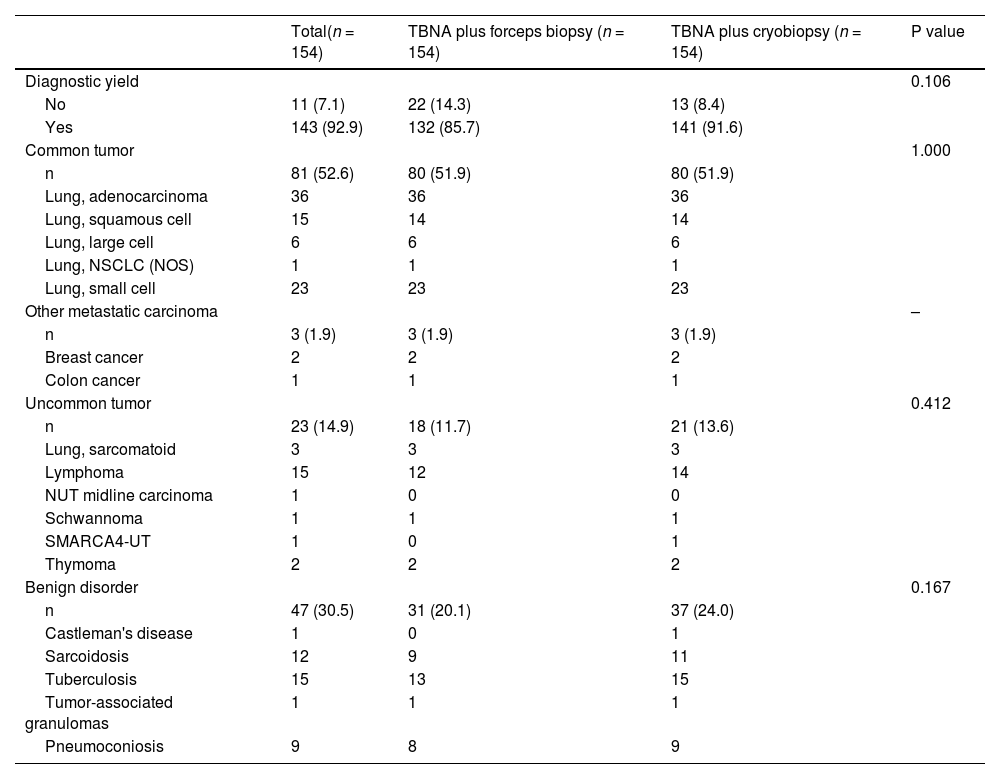
The results of the biopsies are presented in Table 2. Overall, mediastinal specimens arrived at a definite diagnosis in 143 (92.9 %) patients. Consistent with earlier reports, needle aspiration followed by either transbronchial forceps biopsy or mediastinal cryobiopsy resulted in a considerable enhancement of the overall diagnostic yield compared to EBUS-TBNA alone (Supplemental Table 1 and 2). Of note, an extra benefit in the diagnostic yield for benign diseases was only obtained by additional mediastinal cryobiopsy (78.7 % versus 59.6 %, P = 0.044), but not forceps biopsy (66.0 % versus 59.6 %, P = 0.522).
Diagnostic yield analyses (EBUS-TBNA plus forceps biopsy versus EBUS-TBNA plus cryobiopsy).
Data are n (%). TBNA, transbronchial needle aspiration; NSCLC, non-small cell lung cancer; NOS, not otherwise specified; SMARCA4-UT, SMARCA4-deficient undifferentiated tumor.
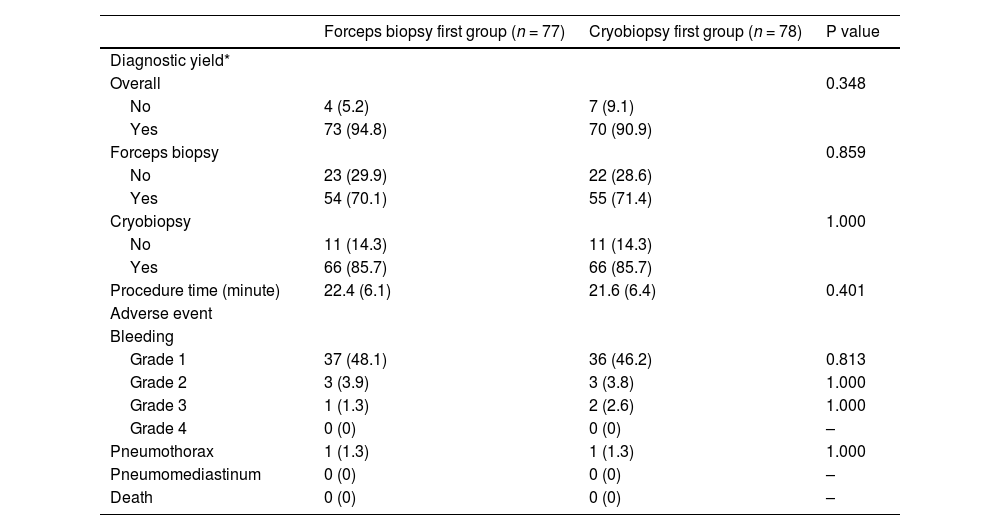
The combination of EBUS-TBNA with either forceps biopsy or cryobiopsy did not differ in overall diagnostic yield (P = 0.106) or for the different subgroup populations. In non-small cell lung cancer (NSCLC), all samples collected by TBNA plus cryobiopsy were suitable for lung cancer genomic and PD-L1 immunohistochemical testings, while this fraction was lower at 89.5 % for TBNA plus forceps biopsy (P = 0.036) (Supplemental Table 3). Diagnostic yields were unaffected by the sequence of biopsies (Table 3).
Diagnostic yield analyses, procedural duration, and complications (forceps biopsy first versus cryobiopsy first).
| Forceps biopsy first group (n = 77) | Cryobiopsy first group (n = 78) | P value | |
|---|---|---|---|
| Diagnostic yield* | |||
| Overall | 0.348 | ||
| No | 4 (5.2) | 7 (9.1) | |
| Yes | 73 (94.8) | 70 (90.9) | |
| Forceps biopsy | 0.859 | ||
| No | 23 (29.9) | 22 (28.6) | |
| Yes | 54 (70.1) | 55 (71.4) | |
| Cryobiopsy | 1.000 | ||
| No | 11 (14.3) | 11 (14.3) | |
| Yes | 66 (85.7) | 66 (85.7) | |
| Procedure time (minute) | 22.4 (6.1) | 21.6 (6.4) | 0.401 |
| Adverse event | |||
| Bleeding | |||
| Grade 1 | 37 (48.1) | 36 (46.2) | 0.813 |
| Grade 2 | 3 (3.9) | 3 (3.8) | 1.000 |
| Grade 3 | 1 (1.3) | 2 (2.6) | 1.000 |
| Grade 4 | 0 (0) | 0 (0) | – |
| Pneumothorax | 1 (1.3) | 1 (1.3) | 1.000 |
| Pneumomediastinum | 0 (0) | 0 (0) | – |
| Death | 0 (0) | 0 (0) | – |
Data are n (%) or mean (SD).
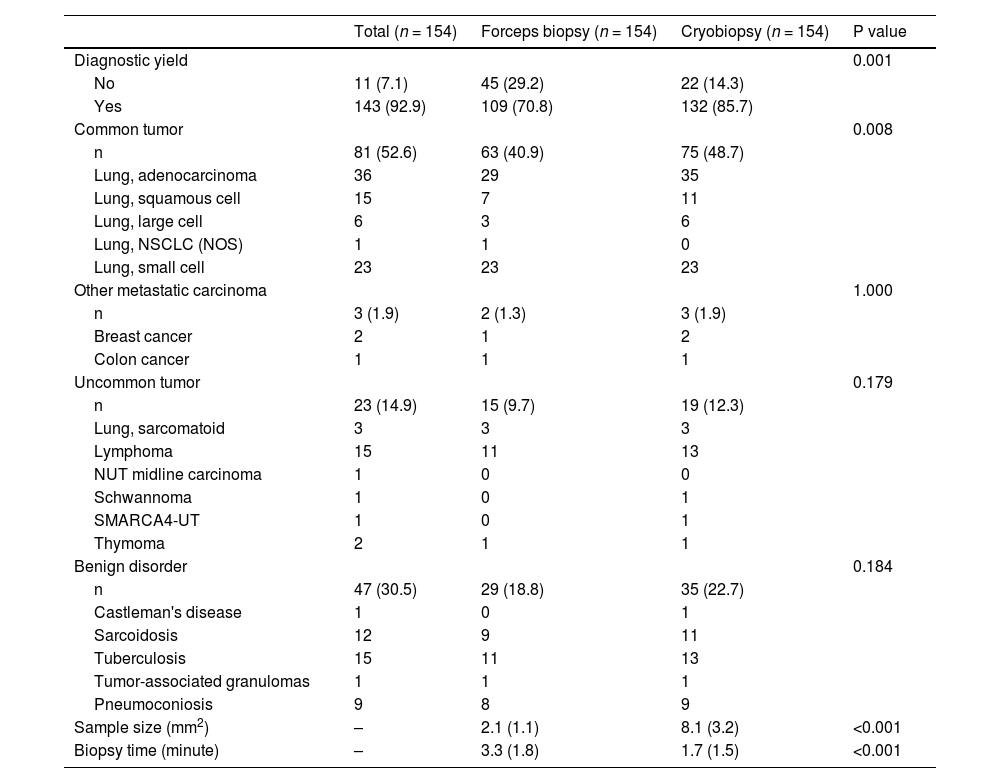
We next compared forceps biopsy alone versus cryobiopsy alone for diagnosis of mediastinal diseases, which revealed an overall diagnostic yield of 70.8 % for forceps biopsy and 85.7 % for cryobiopsy, respectively (P = 0.001) (Table 4). Subgroup analyses demonstrated a substantial advantage in diagnostic accuracy of cryobiopsy for patients with common lung cancer, as compared to forceps biopsy (92.6 % versus 77.8 %, P = 0.008). Cryobiopsy also tended to provide a higher diagnostic yield in rare tumors and benign disorders than forceps biopsy, although these trends did not achieve statistical significance (82.6 % versus 65.2 %, P = 0.179 for rare tumors; 74.5 % versus 61.7 %, P = 0.184 for benign disorders; respectively). Notably, the superiority of cryoprobe over forceps was not affected by biopsy sequence, patient and lesion characteristics, or participating centre (data not shown).
Diagnostic yield analyses, sample size, and procedural duration (forceps biopsy versus cryobiopsy).
Data are n (%) or mean (SD). NSCLC, non-small cell lung cancer; NOS, not otherwise specified; SMARCA4-UT, SMARCA4-deficient undifferentiated tumor.
In 11 (7.1 %) cases, the acquired materials were not diagnostic yet qualified for histological examination, in spite of all accessible EBUS-guided approaches. One of them was subsequently diagnosed as nuclear protein in testis (NUT) midline carcinoma after surgical resection of the lesions, and one was diagnosed as NSCLC by a CT-guided percutaneous needle aspiration biopsy. The remaining 9 patients declined further invasive testing. However, their initially presumed benign diagnosis was verified by regression or stabilization of lesion size in radiologic images over a follow-up period of at least 6 months; therefore, no further workup was pursued.
Adverse eventThere were no severe complications observed at the time of procedure, or at the 4-week follow-up (Table 3). Minor bleeding that did not necessitate haemostatic control was the most frequently encountered adverse event. Two (1.3 %) cases of pneumothorax were detected by chest radiography, yet none required drainage or other interventions.
Sample size and adequacySamples harvested by one cryobiopsy were larger in size even when compared to the combined tissue from three biopsies using a 1.9 mm standard-sized forceps (8.1 ± 3.2 mm2 versus 2.1 ± 1.1 mm2, P<0.001) (Supplemental Figure 1). Each biopsy specimen was deemed sufficient (Supplemental Figure 2).
Operation timeThe overall duration of each EBUS examination was 22.0 ± 6.3 min (range 12.3 - 42.3 min). The procedural time for one cryobiopsy was significantly shorter as compared to the time required for the three forceps biopsies (1.7 ± 1.5 versus 3.3 ± 1.8 min; P<0.001).
DiscussionIn this prospective, dual-centre, randomised clinical trial, we determined the clinical value of transbronchial forceps biopsy and mediastinal cryobiopsy in addition to standard needle biopsy for the diagnosis of mediastinal lesions and perihilar lymphadenopathy. Our data show a significant increase in diagnostic yield by the combination of EBUS-TBNA with either forceps biopsy or cryobiopsy. No significant difference in diagnostic yield was detected between the two combinations. Yet, additional cryobiopsy is less time-consuming, and provides for larger specimens that are better suited for lung cancer molecular genetic analysis and immunological profiling. Direct comparison of the two adjunct approaches yielded a higher overall sensitivity of cryobiopsy alone for mediastinal diseases.
Guidelines recommend EBUS-TBNA as the method of choice for accessing the mediastinum, and especially for the detection of lung cancer metastases.3,16 Yet, endoscopy-guided needle aspiration is limited by the small amount of retrieved material that in many cases can only be used for cytologic evaluation, making the diagnosis of mediastinal lesions from non-lung cancer causes challenging.17,18 Given the revolution of lung cancer management that has shifted from empirical chemotherapy to a personalized approach, alternative ways capable of harvesting sufficient high-quality materials enabling molecular and immunological information have attracted evolving interests. In an attempt to improve the acquisition of histological tissue from mediastinal lymphadenopathies, EBUS-guided forceps biopsy has recently been developed. Several studies have demonstrated its improved diagnostic yields for sarcoidosis and lymphoma.6,13,19 Yet, the largest prospective study of mediastinal forceps biopsy so far suggested in fact a lower sensitivity for the detection of malignancies as compared to standard EBUS-TBNA.14 Motivated by the potential of cryobiopsy to produce sizeable and well-preserved lung specimens, we recently used the cryoprobe as a novel sampling technique for the diagnosis of mediastinal disease.10,11,20,21 In our prior clinical studies, cryoprobe proved superior to standard needle aspiration, in part due to its capacity to obtain sufficient tissue samples for detailed histopathological assessment.11
Of late, there is a rising interest in combined application of needle aspiration and either forceps biopsy or cryobiopsy, aiming at synergistic accuracy.12,22 However, despite a substantial and rapidly expanding body of literature, two critical questions have so far remained unanswered: a) which of these two techniques, forceps or cryobiopsy, may yield the higher diagnostic accuracy either alone or in combination with EBUS-TBNA, and b) which technique is better suited for needle biopsy?
In the past, we have been among the pioneers in the use of forceps biopsy and cryobiopsy for endobronchial and peripheral pulmonary lesion sampling, indicating an overall superiority of cryobiopsy over forceps biopsy for establishing a diagnosis, in part due to higher sample volumes and better sample quality.23-25 To directly compare the usefulness of forceps versus cryobiopsy for the diagnosis of mediastinal lesions, we initiated this prospective study. The exceptional performance of cryosampling in view of its ability to provide the largest mediastinal tissue samples among the minimally invasive endoscopic techniques translated into a superior overall diagnostic yield. Particularly, cryobiopsy enhances accuracy in the detection of mediastinal metastases, and produces samples more conducive to lung cancer molecular testings, which is consistent with prior observations reported in the literature.14,26,27 Technical difficulties have previously been proposed as reasons for the relatively inferior performance of forceps biopsies, such as acute angles of forceps penetration or a fibrotic mediastinum.14 However, taking into account the adequate samples harvested by forceps in our study, we consider its inferiority in mediastinal metastases might primarily be the result of the small tissue size and crush artifacts, which subsequently narrows the scope of sampling and dampens specimen quality. Cryobiopsy, on the other hand, provides for a greater quantity of intact tissue without crush artifacts, and may thus overcome the problem of lesion heterogeneity within metastatic lymph nodes, consequently minimizing the likelihood of a false negative diagnosis. Likewise, a better diagnostic yield for rare tumors and benign disorders was shown for cryobiopsies, although this difference was not statistically significant.
Consistent with previous studies, both forceps biopsy and cryobiopsy increased the overall diagnostic yield of needle aspiration when used as complementary techniques in addition to EBUS-TBNA.12,13 In contrast to the superior efficacy of cryobiopsy in the head to head analyses, the added values of these two combined strategies did not differ significantly. Yet, the amount of material obtained from one cryobiopsy exceeded that from three biopsies with large forceps, while demanding less procedural time. In addition, lung cancer patients may benefit from combined needle aspiration and cryobiopsy due to the increased suitability of the obtained tissue for molecular testings. In line with our prior report, EBUS-guided biopsies were generally safe, with minor bleeding as the most frequently encountered complication.28 No cases of pneumomediastinum, serious bleeding, mediastinal infection, or perioperative death were observed. Post-procedural pneumothorax occurred in 1.5 % of participants with no clinical symptoms, and was self-resolving with no need for drainage. The study design precludes a definitive attribution of these adverse events solely to needle aspiration or its supplementation.
The present study has several limitations. First, because of initial safety concerns, we opted to biopsy only the most suspicious lesion, and it is therefore possible that the utility of these sampling methodologies could thus be impaired. Indeed, the overall diagnostic yields observed in this study are slightly lower than those reported in literature. Nevertheless, the discrepancy might be primarily ascribed to the large proportion of non-lung cancer cases in our cohort, and the strict criteria that the plausible benign diagnoses were judged as negative (nearly one tenth of the cohort). Second, a 1.5- rather than a 1.9 mm biopsy forceps was applied in this trial, due to the challenge of passing the latter through the bronchoscopy's working channel, which may limit the sample volume that can be retrieved by the forceps. Recent studies, however, indicate that the diagnostic accuracy of these two different forceps sizes is comparable.29,30 Finally, on-site cytology was not routinely performed in order to avoid bias in diagnostic analyses. Yet, EBUS procedures followed current guidelines, suggesting no significant influence of ROSE on diagnostic accuracy.31
ConclusionWe here report the first prospective trial to evaluate the use of forceps versus cryoprobe for the diagnosis of mediastinal lesions. In comparison with forceps biopsy, substantially larger tissue samples can be obtained by bronchoscopic cryosampling within shorter time, indicating enhanced effectiveness. In direct head-to-head comparison, cryobiopsy was superior to forceps biopsy in overall diagnostic yield, yet this difference was no longer significant when both techniques were used as add-on to needle aspiration. Needle aspiration supplemented by cryobiopsy remained, however, superior for lung cancer molecular testings compared to the combination of EBUS-TBNA and forceps biopsy. As such, transbronchial mediastinal cryobiopsy might be a valuable adjunct to conventional needle-based biopsy.
Felix JF Herth received honoraria for advisory board activities and lecture fees from Pulmonx, Erbe, Olympus, and Uptake. All other authors declare no competing interests.


