


Hypersensitivity pneumonitis (HP) is an immune-mediated syndrome triggered by inhalation of a wide variety of allergens, to which an individual has previously been sensitized. More than 200 agents responsible for the disease have already been identified; however, HP occurs only in a small number of individuals exposed to causal antigens. The present report provides an overview of the role of antigen role in HP, highlighting its diversity, research methods, and prevention strategies, as well as the impact on disease prognosis following elimination of antigen. HP is an underdiagnosed disease and, therefore, it is difficult to accurately estimate its incidence. Triggering antigens can be divided into six broad categories: bacteria, fungi, mycobacteria, animal and plant proteins, chemicals, and metals, represented by disease prototypes. The identification of causal antigen is a major challenge; it is impossible to obtain in about 30–60% of cases. The acute form of HP, with early detection and immediate eviction of causal antigen, tends to have an excellent prognosis. In the chronic form, partial recovery of disease is still possible; however, some cases tend to progress to fibrosis, even after removal from exposure. In conclusion, HP diagnosis should be based on a proactive search for potential antigen sources, although their identification is hampered by the lack of standardized methods of demonstrating the specific antigen sensitization. Antigen avoidance is a critical determinant in disease prognosis.
Hypersensitivity pneumonitis (HP), also known as extrinsic allergic alveolitis, is an immune-mediated syndrome that results from lung parenchyma and small-caliber respiratory tract inflammation. This reaction is secondary to repeated and prolonged specific antigens inhalation to which an individual is sensitized.1 More than 200 antigens have already been identified as causal agents of HP and these can be found in the workplace, at home, and in recreational activities. The huge majority are derived from fungi, bacteria, protozoa, and animal proteins, or even low-molecular-weight chemical compounds.2 Clinical presentation and disease progression can be extremely variable, depending on the nature of causal agent, exposure duration, and intensity, as well as individual host factors.1,3,4
The incidence and prevalence of HP are difficult to estimate accurately, mostly because of underdiagnosis, which may be partly explained by the absence of widely accepted diagnostic criteria.3,4 Additionally, HP prevalence varies from country to country (and even within the same country), according to geographical conditions, local practices (agricultural and industrial), and host risk factors.3,5 For example, epidemiologic data show an incidence of HP in Europe ranging from 0.3 up to 0.9 per 100000 inhabitants.6–8 In fact, the annual incidence in Denmark is less than 1 per 100000 inhabitants,7 whereas in New Mexico, it is about 30 per 100000 inhabitants,9 and a prospective study carried out in India revealed that HP is the most common interstitial lung disease (47.3% of cases).10
Several HP diagnostic criteria have been proposed, but none of them so far has been validated. However, a recent study, using the modified Delphi method, identified some criteria for chronic HP that achieved consensus among international experts.11 Diagnosis is based on integration of clinical, radiological, and pathological data.12 Identification of causal antigen is crucial, not only for diagnosis, but also for prevention and even prognosis of disease. However, this issue represents a major challenge, mostly because of the lack of standardized techniques.5
In this sense, this report aims to provide an overview of the antigen's role in HP, highlighting its diversity, research methods, and prevention strategies, as well as the impact on disease prognosis due to elimination of the antigen.
From antigen to diseaseThe first descriptions of a pulmonary disease similar to HP, as it is known today, appeared in 1713, associated with people who worked with cereals.13 However, it was only in 1932 that Campbell first described Farmer's lung (FL), a disease that became the classic example of HP.14 In 1959, the respiratory disease was described in mushroom workers caused by the inhalation of compounds contaminated by thermophilic actinomycetes.15 In 1960, the disease was described in workers who come in contact with birds, initially associated with ducks and turkeys, and later also with parakeets and pigeons (Bird-breeder's lungs).16 From this date onward, other agents were progressively reported as having a direct contribution to the onset of this disease, having currently identified more than 200 causal antigens.2,3 HP only develops in a small proportion of individuals exposed to causal antigens; in fact, when exposed to the same causal agent, most individuals are only sensitized, leading to a small increase in lymphocytes locally, but without clinical relevance, which suggests the existence of the host's intrinsic factors in its pathogenesis4,5,17,18 (Fig. 1).
 Classical immunopathological mechanisms proposed for HP (adapted from Delgado et al.96). The coexistence of genetic or environmental promoting factors leads to the development of an exaggerated immune reaction that results in marked lung inflammation. The generation of the granulomatous inflammation requires, among others, the expression of Th1 cytokines, including TNF-α, IL-12, and IFN-γ.18 (B) Persistent antigen exposure and sensitization associates with local antigen–antibody complex deposition, macrophage activation, mononuclear cell recruitment, and predominant Th1 cell-mediated response; continuous exposure leads to critical changes in the lung, ending in fibrosis.4,18.")
Pathogenesis of HP. (A) Classical immunopathological mechanisms proposed for HP (adapted from Delgado et al.96). The coexistence of genetic or environmental promoting factors leads to the development of an exaggerated immune reaction that results in marked lung inflammation. The generation of the granulomatous inflammation requires, among others, the expression of Th1 cytokines, including TNF-α, IL-12, and IFN-γ.18 (B) Persistent antigen exposure and sensitization associates with local antigen–antibody complex deposition, macrophage activation, mononuclear cell recruitment, and predominant Th1 cell-mediated response; continuous exposure leads to critical changes in the lung, ending in fibrosis.4,18.
The coexistence of triggering (e.g., antigen exposure) and promoting factors, such as major histocompatibility complex (MHC II) gene polymorphisms, low-molecular-weight proteasomes, transporters associated with antigen processing-1 (TAP1), or other exposures, such as viruses, may lead to the development of an exacerbated immune reaction resulting in persistent lung inflammation.3,18 In fact, the inhalation of causal antigen leads to an inflammatory reaction, with the release of cytokines and proinflammatory mediators, among others, type 1 T helper (Th1), tumor necrosis factor-α (TNF-α), interleukin-12 (IL-12), and interferon gamma (INF-γ).19 Thereafter, the continued exposure, local antibody production, and/or the presence of genetic susceptibility lead to critical changes in the lung, namely, fibroblast expansion and activation, and extracellular matrix deposition18 (Fig. 1).
An interesting aspect to highlight is that HP is less frequent in cigarette smokers. In fact, nicotine is thought to inhibit macrophage activation, and lymphocyte proliferation and function, but this does not apply to ex-smokers.20 On the other hand, in smokers who develop HP, fibrosing disease with a worse prognosis is more common.21
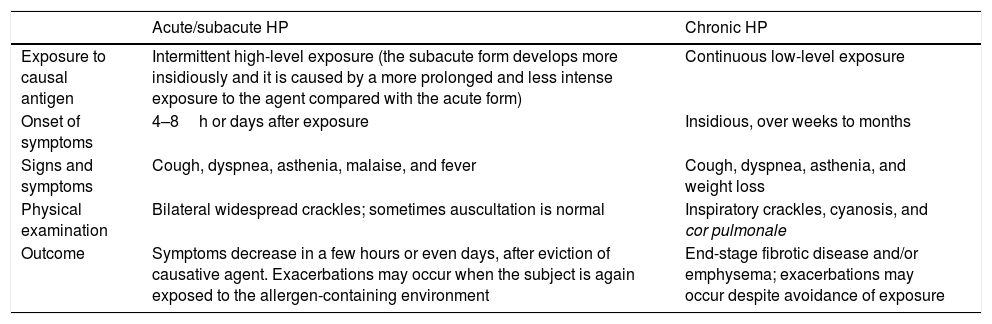
The clinical behavior of HP can be traditionally divided into three distinct phenotypes: acute, subacute, and chronic (Table 1). There is a considerable controversy surrounding this classification, because no widely accepted criteria exist to distinguish the various stages. In fact, the subacute form is considered by some authors as a variant of acute HP.1,4 Lacasse et al.22 performed a cluster analysis, suggesting that HP patients should be classified into only one of the two categories, based on clinical evaluation, pulmonary function tests, and high-resolution computed tomography findings. Other authors have proposed an alternative classification that includes acute or episodic HP, chronic HP with acute episodes, and chronic HP without acute episodes.23 More recently, Vasakova et al.6 proposed a novel HP classification into two main categories: acute/inflammatory HP and chronic/fibrotic HP, based on clinical–radiologic–pathologic correlation, with a considerable prognostic value.
Clinical classification of HP.1,17
| Acute/subacute HP | Chronic HP | |
|---|---|---|
| Exposure to causal antigen | Intermittent high-level exposure (the subacute form develops more insidiously and it is caused by a more prolonged and less intense exposure to the agent compared with the acute form) | Continuous low-level exposure |
| Onset of symptoms | 4–8h or days after exposure | Insidious, over weeks to months |
| Signs and symptoms | Cough, dyspnea, asthenia, malaise, and fever | Cough, dyspnea, asthenia, and weight loss |
| Physical examination | Bilateral widespread crackles; sometimes auscultation is normal | Inspiratory crackles, cyanosis, and cor pulmonale |
| Outcome | Symptoms decrease in a few hours or even days, after eviction of causative agent. Exacerbations may occur when the subject is again exposed to the allergen-containing environment | End-stage fibrotic disease and/or emphysema; exacerbations may occur despite avoidance of exposure |
HP, hypersensitivity pneumonitis.
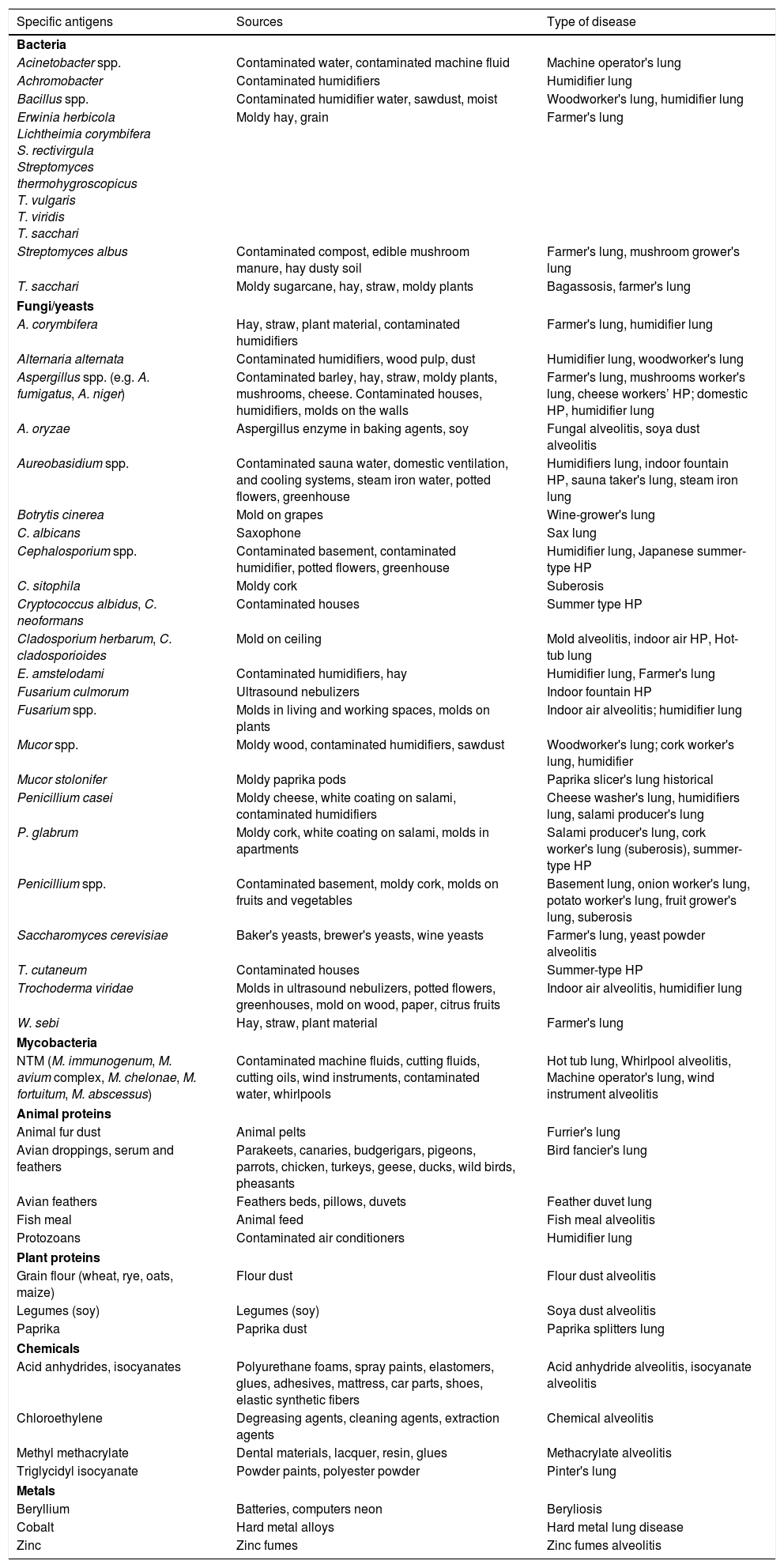
As already mentioned, HP may be induced by a wide and growing variety of antigens, which can be divided into six broad categories: bacteria, fungi, mycobacteria, animal and plant proteins, chemicals, and metals, represented by disease prototypes3 (Table 2).
Causal antigens of HP.4,6,35,56,57
| Specific antigens | Sources | Type of disease |
|---|---|---|
| Bacteria | ||
| Acinetobacter spp. | Contaminated water, contaminated machine fluid | Machine operator's lung |
| Achromobacter | Contaminated humidifiers | Humidifier lung |
| Bacillus spp. | Contaminated humidifier water, sawdust, moist | Woodworker's lung, humidifier lung |
| Erwinia herbicola Lichtheimia corymbifera S. rectivirgula Streptomyces thermohygroscopicus T. vulgaris T. viridis T. sacchari | Moldy hay, grain | Farmer's lung |
| Streptomyces albus | Contaminated compost, edible mushroom manure, hay dusty soil | Farmer's lung, mushroom grower's lung |
| T. sacchari | Moldy sugarcane, hay, straw, moldy plants | Bagassosis, farmer's lung |
| Fungi/yeasts | ||
| A. corymbifera | Hay, straw, plant material, contaminated humidifiers | Farmer's lung, humidifier lung |
| Alternaria alternata | Contaminated humidifiers, wood pulp, dust | Humidifier lung, woodworker's lung |
| Aspergillus spp. (e.g. A. fumigatus, A. niger) | Contaminated barley, hay, straw, moldy plants, mushrooms, cheese. Contaminated houses, humidifiers, molds on the walls | Farmer's lung, mushrooms worker's lung, cheese workers’ HP; domestic HP, humidifier lung |
| A. oryzae | Aspergillus enzyme in baking agents, soy | Fungal alveolitis, soya dust alveolitis |
| Aureobasidium spp. | Contaminated sauna water, domestic ventilation, and cooling systems, steam iron water, potted flowers, greenhouse | Humidifiers lung, indoor fountain HP, sauna taker's lung, steam iron lung |
| Botrytis cinerea | Mold on grapes | Wine-grower's lung |
| C. albicans | Saxophone | Sax lung |
| Cephalosporium spp. | Contaminated basement, contaminated humidifier, potted flowers, greenhouse | Humidifier lung, Japanese summer-type HP |
| C. sitophila | Moldy cork | Suberosis |
| Cryptococcus albidus, C. neoformans | Contaminated houses | Summer type HP |
| Cladosporium herbarum, C. cladosporioides | Mold on ceiling | Mold alveolitis, indoor air HP, Hot-tub lung |
| E. amstelodami | Contaminated humidifiers, hay | Humidifier lung, Farmer's lung |
| Fusarium culmorum | Ultrasound nebulizers | Indoor fountain HP |
| Fusarium spp. | Molds in living and working spaces, molds on plants | Indoor air alveolitis; humidifier lung |
| Mucor spp. | Moldy wood, contaminated humidifiers, sawdust | Woodworker's lung; cork worker's lung, humidifier |
| Mucor stolonifer | Moldy paprika pods | Paprika slicer's lung historical |
| Penicillium casei | Moldy cheese, white coating on salami, contaminated humidifiers | Cheese washer's lung, humidifiers lung, salami producer's lung |
| P. glabrum | Moldy cork, white coating on salami, molds in apartments | Salami producer's lung, cork worker's lung (suberosis), summer-type HP |
| Penicillium spp. | Contaminated basement, moldy cork, molds on fruits and vegetables | Basement lung, onion worker's lung, potato worker's lung, fruit grower's lung, suberosis |
| Saccharomyces cerevisiae | Baker's yeasts, brewer's yeasts, wine yeasts | Farmer's lung, yeast powder alveolitis |
| T. cutaneum | Contaminated houses | Summer-type HP |
| Trochoderma viridae | Molds in ultrasound nebulizers, potted flowers, greenhouses, mold on wood, paper, citrus fruits | Indoor air alveolitis, humidifier lung |
| W. sebi | Hay, straw, plant material | Farmer's lung |
| Mycobacteria | ||
| NTM (M. immunogenum, M. avium complex, M. chelonae, M. fortuitum, M. abscessus) | Contaminated machine fluids, cutting fluids, cutting oils, wind instruments, contaminated water, whirlpools | Hot tub lung, Whirlpool alveolitis, Machine operator's lung, wind instrument alveolitis |
| Animal proteins | ||
| Animal fur dust | Animal pelts | Furrier's lung |
| Avian droppings, serum and feathers | Parakeets, canaries, budgerigars, pigeons, parrots, chicken, turkeys, geese, ducks, wild birds, pheasants | Bird fancier's lung |
| Avian feathers | Feathers beds, pillows, duvets | Feather duvet lung |
| Fish meal | Animal feed | Fish meal alveolitis |
| Protozoans | Contaminated air conditioners | Humidifier lung |
| Plant proteins | ||
| Grain flour (wheat, rye, oats, maize) | Flour dust | Flour dust alveolitis |
| Legumes (soy) | Legumes (soy) | Soya dust alveolitis |
| Paprika | Paprika dust | Paprika splitters lung |
| Chemicals | ||
| Acid anhydrides, isocyanates | Polyurethane foams, spray paints, elastomers, glues, adhesives, mattress, car parts, shoes, elastic synthetic fibers | Acid anhydride alveolitis, isocyanate alveolitis |
| Chloroethylene | Degreasing agents, cleaning agents, extraction agents | Chemical alveolitis |
| Methyl methacrylate | Dental materials, lacquer, resin, glues | Methacrylate alveolitis |
| Triglycidyl isocyanate | Powder paints, polyester powder | Pinter's lung |
| Metals | ||
| Beryllium | Batteries, computers neon | Beryliosis |
| Cobalt | Hard metal alloys | Hard metal lung disease |
| Zinc | Zinc fumes | Zinc fumes alveolitis |
HP, hypersensitivity pneumonitis; NTM, nontuberculous mycobacteria.
The list of HP-associated environments is increasing, but in most situations, the disease is caused by similar antigens in distinct environments.19 Recently, Millon et al.24 have shown the existence of common antigenic amino acid sequences in orthologous proteins from a fungus belonging to Mucorales order and a Mycobacterium species, each one acting as a main etiologic agent of a specific HP form. The existence of common epitopes in orthologous immunogenic proteins from microorganisms belonging to greatly different phylogenetic families explains how, in some cases of HP, a growing number of etiologic agents have been found in the same disease.24 HP can effectively arise in any environment, including workplace, home, and recreational activities, where bacteria and fungi grow or birds are kept.25 Further, drugs can also cause HP, constituting a noninhaling variant of the disease. Although it is a rare cause, and therefore it was not highlighted in this paper, the number of HP-associated drugs is increasing, with more than 380 drugs already reported26–29; therefore, it is extremely relevant to exclude this cause, frequently missed. The individuals with a higher risk of developing HP are those working in agriculture, poultry, and livestock industries; workers using fluid metals;30–32 cheese, sausages, or flour processing;33–35 and malt or soy sauce manufacturers.36 The risk also increases during wood processing (e.g., cork oak bark) and construction; textiles, clothing, or plastics manufacturing; and even in individuals who work with paints, paint hardeners, or other chemical products.37,38 However, in about 30–60% of cases, the antigen remains hidden or unrecognized, some authors have even suggested the use of “cryptogenic HP” for such patients.6,39
Types of disease according to antigen classBacterial exposureFarmer's lung (FL) is considered the HP prototype. Although it is still underdiagnosed, this is one of the most prevalent types of disease, and where bacteria are most commonly the responsible antigens. This form of the disease is triggered by inhalation of antigens from housed microorganisms, in high humidity conditions, in hay, straw, and grain dust stored in agricultural yards.30 FL responsible antigens vary from country to country and depend on climate, farming, and production conditions.40 Thermophilic actinomycetes, such as Saccharopolyspora rectivirgula, Thermoactinomyces vulgaris, Thermoactinomyces viridis, and Thermoactinomyces sacchari, are the most frequently described agents.30,41 However, in some cases, FL disease results from fungal exposure, such as Alternaria, Aspergillus fumigatus, and Botrytis species.42 Further, Reboux et al. (2006) identified Absidia corymbifera, Eurotium amstelodami, and Wallemia sebi as the main causal agents of FL in France.43 In fact, all these organisms typically reproduce at high humidity zones and temperatures of 40–60°C; therefore, this form of HP is most frequent in regions where agriculture predominates, especially during rainy and hot seasons.43 Although the disease prevalence in exposed farmers is not well known, several studies have reported similar findings, placing the prevalence in 0.5–4.4%.44,45
Fungal exposureMolds have been described for years as a common cause of occupational HP.46 In fact, a mold is a type of fungus that grows in damp areas; it releases tiny particles, commonly called as spores, which can be harmful when breathed in.47 Mold-induced HP has been increasingly reported as being caused by humidifiers, heating, and ventilation systems contaminated by Aspergillus, Cladosporium, Penicillium, Aureobasidium pullulans, Cephalosporium, or Mucor species46 (Table 2). However, molds can be found in other unexpected home reservoirs, such as fruits and vegetables, leading to various forms of HP, such as onion worker's lung, potato worker's lung, or fruit grower's lung6; moldy tapestry with Penicillium, Cladosporium, or Botrytis species;47 and even flower pots, whose inhalation of mold spores containing Pullularia pullulans, Trichoderma viride, Cephalosporium acremonium, or A. fumigatus may lead to HP.48 All these exposure sources can go completely unnoticed in a domestic environment and are possibly more frequent than widely recognized. So, a thorough inspection of the whole house is advisable in search of mold stains, even of unnoticed size, humidity, condensation, or a musty odor.46,49
Summer-type HP (SHP) is the most common form of domestic HP in Japan, especially in the western and southern parts of the country; some cases have also been reported in other Asian countries.50 SHP is caused by repeated inhalation of fungi Trichosporon species, namely, Trichosporon cutaneum, which contaminates domestic environments, usually wooden houses, during hot and humid summers, and after a rainy season.50,51T. cutaneum develops at temperatures between 25 and 28°C and a relative humidity above 80%, especially in the presence of wet wood or vegetation.51 An epidemiological study on HP performed in Japan in the 1980s showed that the proportion of SHP cases in patients with HP was 74.4%.52 However, more recently, Iijima et al.53 verified that the incidence seems to be decreasing, mainly due to changes in residential environments, although climatic conditions in any year may cause a temporary increase in the incidence rate.
Suberosis, also known as corkhandler's disease or corkworker's lung, is another form of HP caused by fungi existing in the working environment; it occurs in cork workers and has been mainly reported in Portugal.54–58 Cork oak is the second most dominant forest species in Portugal, making this country the world's leading exporter of cork, followed by Spain.59,60 The processes used in cork manufacture depend on the end product to be obtained; however, during this process, workers are exposed to a heavily contaminated environment with moldy cork dust.56 The most frequent cork colonizing fungi during its industrial processing are Penicillium glabrum (formerly known as Penicillium frequentans) and Chrysonilia sitophila. P. glabrum is the main causative agent of suberosis, but during the storage period, cork can also be colonized by other fungi, such as A. fumigatus or Mucor species.56,57 In Portugal, it has been estimated that 9–19% of cork workers may develop suberosis.54,55
In recent decades, several other different forms of disease caused by fungi have been described in the literature. HP can also be observed in individuals working with woods colonized by fungi, namely, Aspergillus and Penicillium species, Cryptostroma corticale, Alternaria species, among others. The first cases were reported when conventional outdoor drying of wood was replaced by indoor drying in special ovens, as well as in the indoors wood sorting and cutting, to improve working conditions in sawmills.37
Some cases have been reported in food industry workers, such as bakers who are exposed to flour on a daily basis, which can be contaminated with the fungi A. fumigatus;34 cheese producers can also develop cheese workers’ HP caused by Penicillium notatum, Penicillium viridicutum, A. fumigatus, Aspergillus niger, or A. pullulans35; in soy sauce brewer, where precipitin against Aspergillus oryzae was found (soya dust alveolitis);6,36 and even in salami factory workers due to inhalation of dried sausage dust. Morell et al.,33 for example, described five Spanish patients working in dry sausage production with Salami Brusher's disease, caused by P. glabrum and A. fumigatus.
In conclusion, fungal exposure can have various sources, variable in frequency but highly troublesome; so, there should be increasing awareness of the importance of detecting them in any patient's daily activities, such as for instance, musicians, mainly saxophonists who may inhale fungi, Candida albicans, Phoma species, or Ulocladium botrytis, present in the instrument mouthpiece (Sax Lung disease).61
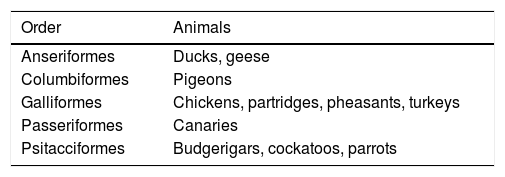
Animal proteins exposureBird fancier's lung (BFL), or bird breeder's disease, is a complex syndrome caused by the repeated inhalation of avian proteins through the form of bird droppings, feathers, or secretions, triggering an exaggerated immune response to the antigen and consequent HP in sensitized individuals.62 Less often, the inhalation may occur from feathers of duvets or pillows.63 BFL is most frequently reported after exposure to pigeons and birds belonging to the Psittaciformes order, including cockatoos, parakeets, and parrots. Elsewhere, some cases of BFL resulting from poultry exposure, including chickens, turkeys, geese, and ducks, have also been reported31,64 (Table 3).
Birds associated with bird fancier's lung.31
| Order | Animals |
|---|---|
| Anseriformes | Ducks, geese |
| Columbiformes | Pigeons |
| Galliformes | Chickens, partridges, pheasants, turkeys |
| Passeriformes | Canaries |
| Psitacciformes | Budgerigars, cockatoos, parrots |
The prevalence of this form of disease varies geographically, which might be partially explained by the local climate, availability of medical resources, local cultural habits, racial factors, smoking habits, and even exposure duration and intensity. However, it is known that BFL is the most common form of HP worldwide, corresponding to 66–68% of all HP forms,31 with a prevalence ranging from 6 to 20% in exposed pigeon breeders.62 In Portugal, some studies have reported a prevalence of BFL ranging from 2 to 5%.65,66 On the other hand, the acute, subacute, and chronic presentations of BFL have also been recognized, but often overlap clinically to each other. In any case, a continuous antigen exposure in chronic phase presents worse prognosis.31
Mycobacterial exposureHot tub baths have become increasingly common in homes, as well as in hotels and spas. Recently, these baths have been associated with an emerging disorder, known as Hot Tub Lung (HTL).67
HTL is a lung disease which can be caused by the inhalation of hot water aerosols from hydromassage baths (the most common cause found in literature) and can also occur in public recreational water facilities, such as swimming pools, saunas, and spas, because these waters are contaminated by nontuberculous mycobacteria (NTM), in most cases belonging to the Mycobacterium avium complex (MAC).67,68
MAC mainly consists of two mycobacteria species, namely, Mycobacterium avium and Mycobacterium intracellulare.69 It is the hydrophobic nature of M. avium and M. intracellulare and the high content of mycolic acid present in their cell walls that makes MAC highly resistant to disinfectants commonly used in swimming pools and spas. They withstand temperatures up to 42°C, exceeding the higher limit of temperature established in spas.68 Glazer et al.70 reported that M. avium and other NTMs were found in 72% of the air and water samples randomly collected from 18 swimming pools; concentrations were significantly lower in chlorine and bromide disinfected pools than in those disinfected with hydrogen peroxide and ultraviolet light.
A relatively recent example of HP induced by mycobacteria is that of metal workers exposed to aerosolized metalworking fluids (MWF) contaminated with NTM, namely, Mycobacterium chelonae and Mycobacterium immunogenum. MWF are complex mixtures of oil and water commonly used as refrigerants and lubricants in various industries.32
Chemical exposureChemically induced HP is an uncommon entity; however, several substances capable of causing the disease have already been described6 (Table 2). Acrylate compounds, such as methyl methacrylate, are associated with an increased incidence of HP in dentists. This increase seems to be associated with the substitution of amalgam fillers by acrylate fillers in dental care.71 On the other hand, isocyanates are highly reactive reagents, widely used in polyurethane polymers production for flexible and rigid foams, such as elastomers, adhesives, surface coatings, and paints.72 Several cases of HP caused by these reagents have already been reported, mainly related to spray painting or plastics manufacturing.38
Other compounds, such as anhydrides used in plastics, paints, resins, and glues, and also triglycidyl isocyanurate, often used in paints, are also recognized as causing HP.31,73 The prevalence of isocyanate-induced HP, related to the plastic manufacturing process, is 1.3% of all chronic HPs in Japan, only three cases having been reported over a 10-year period.72,74
Methods for antigen determinationThe identification of the causal antigen is crucial not only for the diagnosis, but also for establishing preventive measures and of disease prognosis. All available tools for detecting the source of exposure should be used.5
Clinical historyThe first step is to collect a highly detailed clinical history so that it is possible to uncover or to assume the exposure source, either in domestic, recreational, or work setting.5 The use of a standardized questionnaire can be very useful in identifying exposures, otherwise undetected in a more informal discussion with the patient; however, these questionnaires need validation before being used in clinical practice.6
Specific antibodiesThe second step requires the use of laboratory tests to confirm the presence of immunologic sensitization to a suspected antigen, classically using a precipitation reaction between patient's sera and causal antigen extracts for detection of specific antibodies, mainly of the immunoglobulin G (IgG) class.5 The presence of specific IgG antibodies reflects an immune response to a specific exposure, indicating that the individual had a sufficient level of exposure to the antigen to develop sensitization. However, in itself, this aspect is not sufficient to establish the diagnosis, because many asymptomatic individuals show a similar level of humoral responses.17 In fact, precipitins are only an exposure marker. Antibodies precipitating against potential antigens may be present not only in serum and bronchoalveolar lavage (BAL) samples from individuals with HP, but also in some who are asymptomatic although exposed to the same antigens. Up to 40% of the farmers exhibit positive serum precipitins in the absence of clinically significant manifestation of the disease, with no long-term sequelae,3 as shown by one study evaluating 43 asymptomatic milk producers who had serum antibodies specific for FL antigens and did not develop abnormal lung function tests during a 20-year follow-up period.75 Nonetheless, a positive serum antibody testing is a significant predictor of HP (odds ratio, 5.3; 95% confidence interval, 2.7–10.4)76 although the absence of serum precipitin does not exclude an HP diagnosis.2 Fenoglio et al.77 found that serum precipitins were useful for diagnosing acute HP induced by fungi (predictive negative value, 81–88%; predictive positive value, 71–75%). There are several laboratory methods for qualitative determination of specific antibodies, such as the precipitation reaction of the double immunodiffusion of Ouchterlony or combinations with immunoelectrophoresis, as well as those for quantitative determination, such as, enzyme-linked immunosorbent assay (ELISA), ImmunoCAP® or Immulite®. In general, the results obtained using these methods differ considerably78; ELISA is, at present, the most frequently used.79–82 Sandoval et al. (1990), carrying out a comparative study for detection of specific antibodies in BAL of patients with HP, using immunoelectrophoresis and ELISA, found positivity in 12 and 100% of the cases, respectively, showing its usefulness for antibody detection against pigeon antigens in fluids with a low protein content.81 In another study, Simpson et al. (1992) revealed that the ELISA method showed greater sensitivity (nearly to 103 times higher) than the double-immunodiffusion method, in patients with BFL.82 Suhara et al.80 also reported high sensitivity and specificity of the antibodies, 80–100 and 92–100%, respectively, in acute bird-related HP, claiming that antibody titers may be lower in chronic bird-related HP, because cellular immunity is more closely associated with chronic bird-related HP pathology than the humoral immunity.
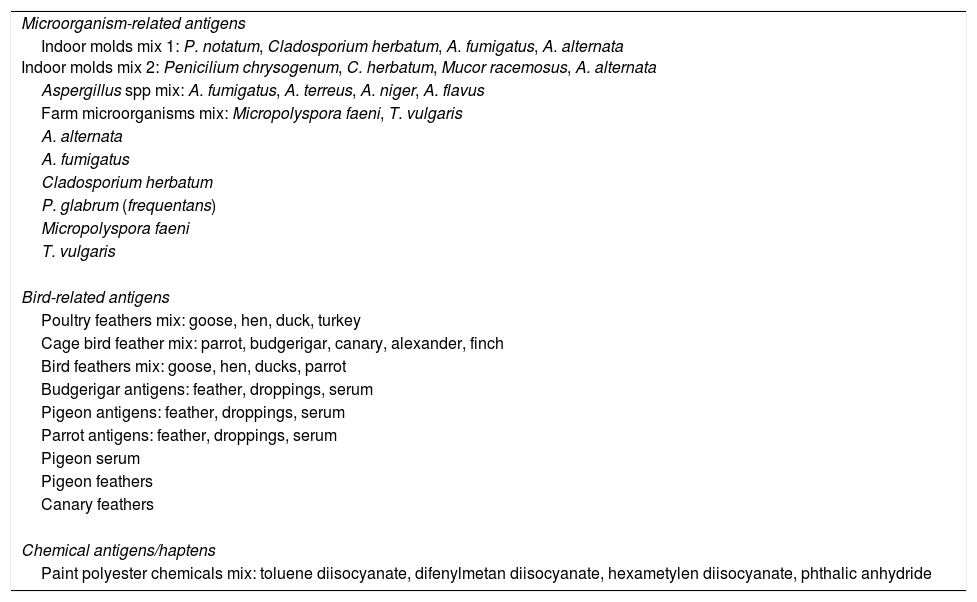
There is a long list of potential antigens in HP, although there is only a limited number of available antigen preparations proposed for detection (Table 4). The selection of antigens to be tested should be based on the individual exposure history and in the most prevalent type in each region.6,78 In fact, the serum-specific IgG (sIgGs) panels used in different centers is determined by practice location. An example of a sIgGs panel includes molds, bacteria, animal proteins, and chemical substances, as illustrated in Table 4.
Some common antigen panels and mixtures available for specific IgG quantification to evaluate exposure/sensitization in suspected HP (adapted from Vasakova et al.6).
| Microorganism-related antigens |
| Indoor molds mix 1: P. notatum, Cladosporium herbatum, A. fumigatus, A. alternata Indoor molds mix 2: Penicilium chrysogenum, C. herbatum, Mucor racemosus, A. alternata |
| Aspergillus spp mix: A. fumigatus, A. terreus, A. niger, A. flavus |
| Farm microorganisms mix: Micropolyspora faeni, T. vulgaris |
| A. alternata |
| A. fumigatus |
| Cladosporium herbatum |
| P. glabrum (frequentans) |
| Micropolyspora faeni |
| T. vulgaris |
| Bird-related antigens |
| Poultry feathers mix: goose, hen, duck, turkey |
| Cage bird feather mix: parrot, budgerigar, canary, alexander, finch |
| Bird feathers mix: goose, hen, ducks, parrot |
| Budgerigar antigens: feather, droppings, serum |
| Pigeon antigens: feather, droppings, serum |
| Parrot antigens: feather, droppings, serum |
| Pigeon serum |
| Pigeon feathers |
| Canary feathers |
| Chemical antigens/haptens |
| Paint polyester chemicals mix: toluene diisocyanate, difenylmetan diisocyanate, hexametylen diisocyanate, phthalic anhydride |
Currently, clinicians do not have access to tests that allow them to individualize the panel for actual exposure on their patients. In addition, the specific antibodies are not always identified in patients with HP, probably because some of the antigens that cause this condition still remain unknown.83 The finding that common peptide epitopes may induce cross-reactivity in HP serodiagnosis can affect test performance when searching for epitopes that are common to different microorganisms and capable of inducing the same antibody response in patients with HP; this is a current challenge.24
The lack of reliable standardized techniques and of established physiological intervals for sIgGs levels against possible causal antigens raise concerns about the diagnostic use of this technique.5 It would, therefore, be advantageous to involve auxiliary specialists, occupational physicians, and industrial or environmental hygienists to obtain more reliable samples for microscopic, microbiological, and immunological analysis.6 However, despite all these limitations, this technique is essential to support the HP diagnosis, sometimes determinant in discovering new etiologies of the disease, as well as providing differential diagnosis between HP and other diseases, such as idiopathic pulmonary fibrosis (IPF).75,84
Specific inhalation challengeA third method of confirming causality between a suspected antigen and the disease is the specific inhalation challenge (SIC), which presupposes patient exposure to the potentially contaminated environment either through direct inhalation of the antigens or through commercially available extracts.5 This technique has also been used to confirm a suspected etiologic agent and when there are doubts about the differential diagnosis of chronic HP and IPF.85 The focus of SIC is to demonstrate that exposure to a particular agent produces a fall in forced expiratory volume in one second (FEV1) while ensuring that fall remains within safety limits and does not cause serious adverse reactions. Indeed, most authors recommend that, during SIC, exposure should be increased very gradually; in fact, the exposure intensity is of particular relevance to enhance SIC safety, especially with previously unknown sensitizing agents. In this context, it would be very useful to identify patient characteristics that predict a specific response during SIC.86 Morell et al.64 proposed that SIC should be considered the “gold standard” among noninvasive BFL diagnostic examinations, focusing on decreased forced vital capacity (FVC) and/or lung diffusing capacity for carbon monoxide (DLCO). In fact, this test reveals very satisfactory sensitivities and specificities in experienced centers.6 In a study carried out by Muñoz et al.,87 SIC evidenced a good diagnostic yield in 113 patients with suspected HP. The overall sensitivity and specificity were, respectively, 73 and 84%, when tests against all causative agents were analyzed together; and 85 and 86%, respectively, when evaluating results in patients only exposed to avian or fungal antigens. In the same way, Ishizuka et al.88 demonstrated that the sensitivity and specificity for diagnosing chronic BFL were as high as 92.9 and 94.7%, respectively.
Despite its “gold standard” status, SIC is rarely performed because it is neither standardized nor validated, because specialized centers are required which have experience in the procedure and proper equipment for treatment of uncommon, but potential complications.78
PreventionAvoiding exposure to causal agent is the cornerstone of HP management and an important and determinant factor for prognosis, because progression is largely avoidable with appropriate antigen eviction.3 Patients should be advised about the relevance of a clean domestic air environment and the absolute necessity of avoiding further exposures to known HP causative agents. However, eviction is difficult for most patients because of professional or personal issues (e.g., affective links to a pet or fear of abandoning a hobby).6 In this sense, an occupational and environmental health professional should carefully recognize individuals at risk, identified through a detailed history and exposure evaluation in the workplace, and also collaborate with partners in the local community and employers to raise awareness about the risks of antigen exposure, and even inform them about preventive measures. Providing simple and accessible educational material can also help to reduce exposure and to facilitate more accurate diagnosis, as well as to incite the use of personal protective equipment, including masks and respirators.89
In the specific case of FL exposure, there are three possibilities for reducing repeated inhalation of organic particles and, thus preventing progression to a fibrosing process: (1) definitive withdrawal of patients from workplace, which in most situations is not a feasible solution for economic reasons; (2) improve the storage methods for hay or straw; it has been shown that storing in low-density bundles hinders the growth of microorganisms, rather than round bales with a high concentration of moisture due to the increased hay compaction; (3) use of really efficient respiratory protection devices capable of preventing the entry of antigens into the bronchial tree.30 In the case of pigeon breeders, they might be encouraged to spend less time in the loft and to wear a hat and coat which can be removed when exiting the loft, so as to avoid continuous contact with the antigen that can be carried on clothing or hair. Increasing the level of ventilation in the loft can also be useful in reducing antigen exposure.17 In respect to HTL, the World Health Organization recommends that treatment and prevention methods of HP caused by M. avium should include protection, coagulation, flocculation, sedimentation, filtration, disinfection, and protection of water distribution system.68
PrognosisHP evolution is highly variable and depends essentially on the time and concentration of antigen exposure. Individuals with acute form of the disease, but who were detected early and the causal antigen was immediately evicted, tend to have an excellent prognosis. In chronic forms, a partial recovery may also occur; however, in some cases, the disease tends to progress, leading to a permanent loss of lung function, irreversible pulmonary fibrosis and death, even after antigen eviction and appropriate treatment.6,91 For example, about 20% of the acute forms of FL evolve into chronic forms and are irreversible30 and fatal HP cases have been reported to be related to acute exacerbations after chronic exposure to some antigens, namely, avian protein antigens, thermophilic actinomycetes, molds, heated plastics, among others.72,91,92
Mortality data are scarce in the literature; however, in England and Wales, from 1968 to 2008, 878 HP deaths were reported,93 whereas in a study performed in Denmark, 5-year survival rate was 93%.7 In chronic HP, the average survival rate is 7 years.1
Factors associated with a poor prognosis include longer exposure period, high-intensity antigen exposure, advanced age, smoking, and a radiological and/or histological pattern with fibrosis.1,6,21,90,94 The antigen type may also influence the prognosis, because there are some data suggesting that BFL may have a worse prognosis than FL.5 However, Braun et al.95 suggest that exacerbations/relapses are the factors that most influence a detrimental evolution long term. Further, Fernandez-Pérez et al.39 following up 142 HP cases reported that the nonidentification of antigen was associated with a decrease in survival from 18.2 to 9.3 years.
ConclusionHP occurs only in a small number of individuals exposed to causal antigens. Most individuals are only sensitized, because the development of the disease is based on the interaction between inducing factors (causal antigen) and promoters, itself related to the host (genetic background and additional environmental factors), leading to dysregulation of the immune system and consequent persistent inflammation.
Several forms of the disease have been described, the most common being caused by the inhalation of bacteria, proteins, fungi, or mycobacteria present in the host environment, such as workplace, home environment, or recreational activities. Other substances, such as chemicals (namely, isocyanates, or acrylates) may also act as triggering agents, despite being less commonly associated with the disease.
The diagnosis of HP should be based on a proactive search for potential antigen sources, whose identification is often hampered by the lack of recognition of some sources and/or by the absence of standardized detection methods of sensitization. In this context, it would be legitimate to create multidisciplinary public health teams to collect and to evaluate in locus potentially suspicious material.
Eviction of the causal agent exposure is the cornerstone of HP management, because antigen inhalation maintenance has prognostic implications, with the consequent progression and reduction in survival rate. In this way, protection measures should be implemented, in particular, at the level of the individual or at the source of exposure itself. A longer exposure period, high antigenic intensity, the type of antigen, and the unidentified exposure source are associated with a reserved prognosis.
Conflicts of interestThe authors declare no conflicts of interest.


