

As the Coronavirus disease 2019 (COVID-19) is spreading worldwide, countries are dealing with different phases of the pandemic. Lately, scientific evidence has been growing about the measures for reopening respiratory outpatient services during the COVID-19 pandemic. We aim to summarize the key differences and similarities among recommendations by different national and international organizations.
MethodsWe searched on Google and Pubmed for recently published National and International Recommendations/Guidelines/Position Papers from professional organizations and societies, offering a guidance to physicians on how to safely perform pulmonary function testing during COVID-19 pandemic. We also searched for spirometry manufacturers' operational indications.
ResultsIndications on spirometry were released by the Chinese Task force, the American Thoracic Society, the European Respiratory Society, the Thoracic Society of Australia and New Zealand, the Société de Pneumologie de Langue Française, the Spanish Societies (Sociedad Espanola de Neumologia y Cirugia Toracica, Sociedad Espanola de Alergologia e Inmunologia Clinica, Asociacion de Especialistas en Enfermeria del trabajo, Asociacion de Enfermeria Comunitaria), the Sociedade Portuguesa de Pneumologia, the British Thoracic Society/Association for Respiratory Technology & Physiology, the Irish Thoracic Society, the Sociedad Uruguaya de Neumologia, the Italian Thoracic Society and the Italian Respiratory Society, Cleveland Clinic and Nebraska Medical Center. Detailed technical recommendations were found on manufacturers’ websites. We found several similarities across available guidelines for safely resuming pulmonary function services, as well as differences in criteria for selecting eligible patients for which spirometry is deemed essential and advice which was not homogenous on room ventilation precautions.
ConclusionsThis study shows a synthesis of national/international guidelines allowing practicing physicians to adapt and shape the way to organize their outpatient services locally. There is generally good agreement on the importance of limiting pulmonary function testing to selected cases only. However, significant differences concerning the subsets of candidate patients, as well as on the management of adequate room ventilation, were observed.
Coronavirus disease 2019 (COVID-19) has spread worldwide, becoming a public health emergency of international concern,1 officially designated as a pandemic by World Health Organization (WHO) on March 11.2 COVID-19 has had a high impact on the health care system, necessitating unprecedented measures for containing the infection, shutting down all the outpatient activities and providing treatment only for emergency cases.3
The infection is mainly transmitted by respiratory droplets4 and close contacts, so both pulmonologists and their patients are at high risk of COVID-19 transmission during the outpatient visit and the pulmonary function testing procedures. Therefore, in the early phases of the pandemic some International Societies such as the Chinese expert consensus,5 the American Thoracic Society (ATS),6 the Thoracic Society of Australia and New Zealand (TSANZ/ANZSRS),7 the Sociedade Portuguesa de Pneumologia (SPP),8 the Société de Pneumologie de Langue Française (SPLF),9 the Spanish Societies [Sociedad Espanola de Neumologia y Cirugia Toracica (SEPAR), Asociacion de Enfermeria Comunitaria (AEC), Asociacion de Especialistas en Enfermeria del trabajo (AET), Sociedad Espanola de Alergologia e Inmunologia Clinica (SEAIC)]10 and the Irish Thoracic Society (ITS),11 recommended stopping or postponing pulmonary visits and pulmonary function tests (PFTs) during the pandemic surge unless deemed clinically essential.5–8,11,12
Nevertheless, PFTs cannot be delayed for a long time in some patients’ groups. Moreover, a respiratory follow-up of patients who recovered from COVID-19 pneumonia is crucial in the monitoring of a possible fibrotic complication of the disease which could lead to a reduction of the pulmonary function.1,5 Entering the second phase of the COVID-19 pandemic, we need to consider that the infection will remain endemic and we have to coexist with the disease, which will become a part of the routine practice. Therefore, hospitals have to be prepared to safely bring back regular ambulatory services and PFT labs, especially to assess patients suffering from pre-existing chronic respiratory diseases, to prevent their risk of mortality and disability.
To date, several official Recommendations/Guidelines from National and International Societies, hospitals or professional organizations have been released on this topic with operational indications during the COVID-19 surge.5–11,13 Some Organizations updated their own documents,14–16 and other Societies, such as the European Respiratory Society (ERS),17 the British Thoracic Society/Association for Respiratory Technology & Physiology (BTS/ARTP),12 the Sociedad Uruguaya de Neumologia (SUNEUMO),18 the Italian Thoracic Society (ITS/AIPO),19 and the Italian Respiratory Society (IRS/SIP),20 as well as renowned medical centers such as Cleveland Clinic,21 recently published statements.
We aim to summarize the available official recommendations on the use of spirometry in the context of COVID-19 infection and to compare them, reviewing in detail the most important aspects, such as eligible patients, health-care workers’ and patients’ protection, equipment, and environmental management to prevent COVID-19 transmission. These results will help practicing physicians make decisions on how to safely reshape and reopen ambulatory services, tailoring measures to the specific context of their needs, and organizational issues.22
MethodsWe searched and reviewed all recent Guidelines, Consensus documents, Statements, and Position Papers from National and International Societies or local policies of medical centers on how to perform spirometry during COVID-19, published on official websites in four languages: English, Italian, French and Spanish.
To increase the search strategy’s sensitivity, we also searched on Google the websites of the spirometer manufacturers using the following terms: COVID-19, Sar-Cov-2, spirometry, pulmonary function test.
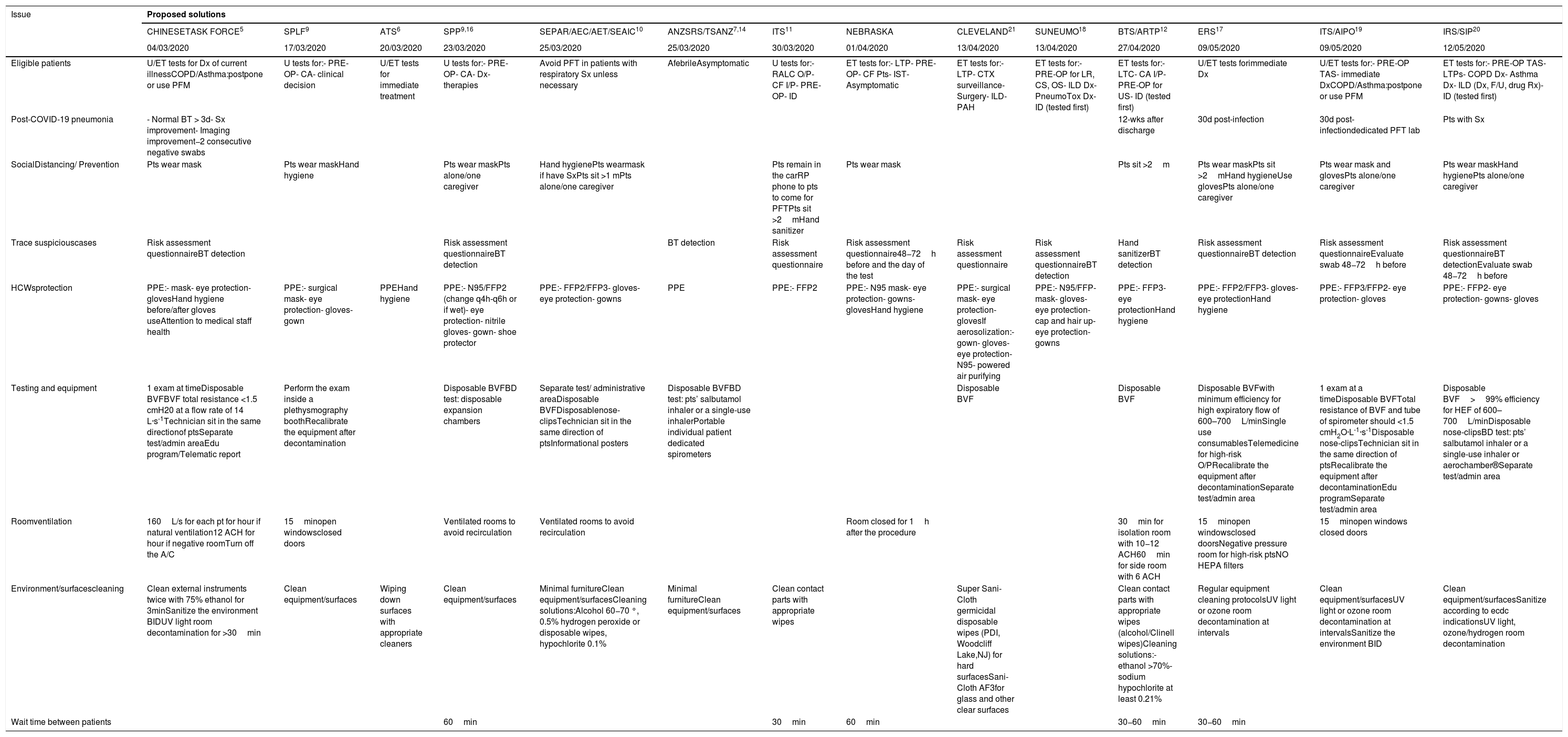
ResultsWe considered the challenging issues related to performing spirometry and the solutions that may be adopted, as suggested by official Recommendations. Table 1 summarizes Societies’ Recommendations on performing PFTs.
Issues related to safely performing pulmonary function test and proposed solutions by National/International Organizations.
| Issue | Proposed solutions | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CHINESETASK FORCE5 | SPLF9 | ATS6 | SPP9,16 | SEPAR/AEC/AET/SEAIC10 | ANZSRS/TSANZ7,14 | ITS11 | NEBRASKA | CLEVELAND21 | SUNEUMO18 | BTS/ARTP12 | ERS17 | ITS/AIPO19 | IRS/SIP20 | |
| 04/03/2020 | 17/03/2020 | 20/03/2020 | 23/03/2020 | 25/03/2020 | 25/03/2020 | 30/03/2020 | 01/04/2020 | 13/04/2020 | 13/04/2020 | 27/04/2020 | 09/05/2020 | 09/05/2020 | 12/05/2020 | |
| Eligible patients | U/ET tests for Dx of current illnessCOPD/Asthma:postpone or use PFM | U tests for:- PRE-OP- CA- clinical decision | U/ET tests for immediate treatment | U tests for:- PRE-OP- CA- Dx- therapies | Avoid PFT in patients with respiratory Sx unless necessary | AfebrileAsymptomatic | U tests for:- RALC O/P- CF I/P- PRE-OP- ID | ET tests for:- LTP- PRE-OP- CF Pts- IST- Asymptomatic | ET tests for:- LTP- CTX surveillance- Surgery- ILD- PAH | ET tests for:- PRE-OP for LR, CS, OS- ILD Dx- PneumoTox Dx- ID (tested first) | ET tests for:- LTC- CA I/P- PRE-OP for US- ID (tested first) | U/ET tests forimmediate Dx | U/ET tests for:- PRE-OP TAS- immediate DxCOPD/Asthma:postpone or use PFM | ET tests for:- PRE-OP TAS- LTPs- COPD Dx- Asthma Dx- ILD (Dx, F/U, drug Rx)- ID (tested first) |
| Post-COVID-19 pneumonia | - Normal BT > 3d- Sx improvement- Imaging improvement−2 consecutive negative swabs | 12-wks after discharge | 30d post-infection | 30d post-infectiondedicated PFT lab | Pts with Sx | |||||||||
| SocialDistancing/ Prevention | Pts wear mask | Pts wear maskHand hygiene | Pts wear maskPts alone/one caregiver | Hand hygienePts wearmask if have SxPts sit >1 mPts alone/one caregiver | Pts remain in the carRP phone to pts to come for PFTPts sit >2mHand sanitizer | Pts wear mask | Pts sit >2m | Pts wear maskPts sit >2mHand hygieneUse glovesPts alone/one caregiver | Pts wear mask and glovesPts alone/one caregiver | Pts wear maskHand hygienePts alone/one caregiver | ||||
| Trace suspiciouscases | Risk assessment questionnaireBT detection | Risk assessment questionnaireBT detection | BT detection | Risk assessment questionnaire | Risk assessment questionnaire48−72h before and the day of the test | Risk assessment questionnaire | Risk assessment questionnaireBT detection | Hand sanitizerBT detection | Risk assessment questionnaireBT detection | Risk assessment questionnaireEvaluate swab 48−72h before | Risk assessment questionnaireBT detectionEvaluate swab 48−72h before | |||
| HCWsprotection | PPE:- mask- eye protection- glovesHand hygiene before/after gloves useAttention to medical staff health | PPE:- surgical mask- eye protection- gloves- gown | PPEHand hygiene | PPE:- N95/FFP2 (change q4h-q6h or if wet)- eye protection- nitrile gloves- gown- shoe protector | PPE:- FFP2/FFP3- gloves- eye protection- gowns | PPE | PPE:- FFP2 | PPE:- N95 mask- eye protection- gowns- glovesHand hygiene | PPE:- surgical mask- eye protection- glovesIf aerosolization:- gown- gloves- eye protection- N95- powered air purifying | PPE:- N95/FFP-mask- gloves- eye protection- cap and hair up- eye protection- gowns | PPE:- FFP3- eye protectionHand hygiene | PPE:- FFP2/FFP3- gloves- eye protectionHand hygiene | PPE:- FFP3/FFP2- eye protection- gloves | PPE:- FFP2- eye protection- gowns- gloves |
| Testing and equipment | 1 exam at timeDisposable BVFBVF total resistance <1.5 cmH20 at a flow rate of 14 L·s-1Technician sit in the same directionof ptsSeparate test/admin areaEdu program/Telematic report | Perform the exam inside a plethysmography boothRecalibrate the equipment after decontamination | Disposable BVFBD test: disposable expansion chambers | Separate test/ administrative areaDisposable BVFDisposablenose-clipsTechnician sit in the same direction of ptsInformational posters | Disposable BVFBD test: pts’ salbutamol inhaler or a single-use inhalerPortable individual patient dedicated spirometers | Disposable BVF | Disposable BVF | Disposable BVFwith minimum efficiency for high expiratory flow of 600–700L/minSingle use consumablesTelemedicine for high-risk O/PRecalibrate the equipment after decontaminationSeparate test/admin area | 1 exam at a timeDisposable BVFTotal resistance of BVF and tube of spirometer should <1.5 cmH2O·L-1·s-1Disposable nose-clipsTechnician sit in the same direction of ptsRecalibrate the equipment after decontaminationEdu programSeparate test/admin area | Disposable BVF>99% efficiency for HEF of 600–700L/minDisposable nose-clipsBD test: pts’ salbutamol inhaler or a single-use inhaler or aerochamber®Separate test/admin area | ||||
| Roomventilation | 160L/s for each pt for hour if natural ventilation12 ACH for hour if negative roomTurn off the A/C | 15minopen windowsclosed doors | Ventilated rooms to avoid recirculation | Ventilated rooms to avoid recirculation | Room closed for 1h after the procedure | 30min for isolation room with 10−12 ACH60min for side room with 6 ACH | 15minopen windowsclosed doorsNegative pressure room for high-risk ptsNO HEPA filters | 15minopen windows closed doors | ||||||
| Environment/surfacescleaning | Clean external instruments twice with 75% ethanol for 3minSanitize the environment BIDUV light room decontamination for >30min | Clean equipment/surfaces | Wiping down surfaces with appropriate cleaners | Clean equipment/surfaces | Minimal furnitureClean equipment/surfacesCleaning solutions:Alcohol 60−70 °, 0.5% hydrogen peroxide or disposable wipes, hypochlorite 0.1% | Minimal furnitureClean equipment/surfaces | Clean contact parts with appropriate wipes | Super Sani-Cloth germicidal disposable wipes (PDI, Woodcliff Lake,NJ) for hard surfacesSani-Cloth AF3for glass and other clear surfaces | Clean contact parts with appropriate wipes (alcohol/Clinell wipes)Cleaning solutions:- ethanol >70%- sodium hypochlorite at least 0.21% | Regular equipment cleaning protocolsUV light or ozone room decontamination at intervals | Clean equipment/surfacesUV light or ozone room decontamination at intervalsSanitize the environment BID | Clean equipment/surfacesSanitize according to ecdc indicationsUV light, ozone/hydrogen room decontamination | ||
| Wait time between patients | 60min | 30min | 60min | 30−60min | 30−60min | |||||||||
List of Abbreviations: 30d: 30 days; A/C: air conditioning; ACH: air changes per hour; Admin: administrative; AET: Asociacion de Especialistas en Enfermeria del trabajo; AEC: Asociacion de Enfermeria Comunitaria; AS: Asymptomatic; ARTP: Association for Respiratory Technology and Physiology; ATS: American Thoracic Society; ANZSRS: Australian and New Zealand Society of Respiratory Science Ltd; ANZSRS: Australian and New Zealand Society of Respiratory Science Ltd; BD-Test: Post Bronchodilator test; BID: twice a day; BT: Body Temperature; BTS: British Thoracic Society; BVF: Bacterial/viral filter; CA: Cancer Patients; CF: Cystic fibrosis; CLEVELAND: Respiratory Institute Cleveland Clinic; COPD: Chronic Obstructive Pulmonary Disease; CS: Cardiac Surgery; CTX: chemotherapy; Dx: diagnosis; ecdc: European Centre for Disease Prevention and Control; Edu program: Educational program; ERS: European Respiratory Society; ET: essential; FFP: filtering face piece; F/U: follow up; HCWs: Health Care Workers; HEF: High Expiratory Flow; HEPA: High Efficiency Particulate Air filter; I/P: inpatients; ID: Immunocompromised patients; ILD: Interstitial Lung Diseases; IRS/SIP: Italian Respiratory Society/Società Italiana di Pneumologia; IST: Immunosuppressive Therapies; ITS: Irish Thoracic Society; ITS/AIPO: Italian Thoracic Society/Associazione Italiana Pneumologi Ospedalieri; LR: Lung Resection; LTC: long-term conditions; LTP: Lung Transplant Patients; Min: minutes; O/P: outpatients; OS: Oncological Surgery; PAH: Pulmonary Arterial Hypertension; PFM: Peak Flow Meter; PFTs: Pulmonary Function Tests; PneumoTox: Pneumotoxicity; PPE: personal protective equipment; PRE-OP: Preoperative patients; Pt/Pts: patient/patients; q4h: every 4h; q6h: every 6h; RALC: Rapid Access Lung Cancer Patients; RP: Respiratory Physiologist; SEIAC: Spanish Society of Allergy and Clinical Immunology; SEPAR: Spanish Society of Pneumology and Thoracic Surgery; Sx: symptoms; SPLF: Société de Pneumologie de Langue Française; SPP: Sociedade Portuguesa de Pneumologia; SUNEUMO: Sociedad Uruguaya de Neumologia; TAS: Thoraco-Abdominal Surgery; TR: Telematic Reports; TSANZ: Thoracic Society of Australia and New Zealand; U: urgent; US: Urgent Surgery; UV: ultraviolet; Wks: weeks.
There was an overall good agreement among Guidelines on limiting PFTs to patients really needed them, weighing the benefits of ongoing care and clinical evaluation with “exposure risk” to COVID-19 for individuals coming to the hospital. Nevertheless, we found heterogeneous indications on the subgroup of patients considered a priority.
The ATS6 and ERS17 Recommendations generically advise performance of PFTs when they are essential for immediate treatment decisions of the current illness. At the same time, SPP,16 SPLF9 and BTS/ARTP guidelines12 strongly encourage performing essential procedures only in cancer patients or in cases of pre-operative assessments for urgent surgery. In contrast, the recent update of the Australian Guidelines14 suggests that asymptomatic patients might undergo PFTs, especially in cases of a pre-operative evaluation for elective surgery. The ITS11 Guidelines recommend performing PFTs in patients with cystic fibrosis and rapid access lung cancer and in those needing a pre-operative assessment for emergency surgery. Furthermore, they recommend spirometry in immunocompromised patients for urgent treatment (e.g. bone marrow transplant, lung transplants, pre-chemotherapy treatments), suggesting testing them first on the day. Conversely, the Chinese expert Recommendations5 limit PFTs only to patients needing them; moreover, they specify that in patients with asthma and chronic obstructive pulmonary disease (COPD), the test might be suspended unless urgently needed for diagnosis and treatment, suggesting the use of a peak flow meter for self-monitoring the lung function. Similar indications come from the Position Paper of the ITS/AIPO Italian Society,19 which also prioritizes patients needing thoraco-abdominal surgery. The latest released IRS/SIP Recommendations,20 provide more broad indications, including the diagnosis of COPD and asthma and interstitial lung diseases, the follow-up and the antifibrotic drugs prescription. Cleveland21 is the only Organization that also mentions patients with pulmonary hypertension, while SUNEUMO18 also takes into account patients with pneumoconiosis and respiratory drug toxicity. Finally, the SEPAR/AEC/AET/SEAIC10 Recommendations suggest performing PFTs in negative rooms and postponing them unless urgently needed.
As regards patients recovered from COVID-19 experiencing persistent or evolving respiratory complications, BTS/ARTP12 Guidelines propose a detailed follow-up: all patients recovered from a severe (hospitalized in Intensive Care Unit/High Dependency Unit, or necessitating protracted dependency on a high fraction of inspired oxygen or noninvasive ventilation during the hospital stay, or discharged with oxygen or with significant ongoing respiratory symptoms) or a mild to moderate pneumonia, or clinically improved patients with persistent changes in the chest X-ray 12 weeks post-discharge, should undergo PFTs. Patients with a previous COVID-19 pneumonia are also mentioned by the ERS17 Guidelines that only specify that these patients must not be tested for a minimum of 30 days post-infection. The ITS/AIPO19 Position Paper recommends a documented negative swab test 48−72h before PFTs or arranging dedicated post-COVID PFTs lab facilities, while IRS/SIP20 Guidelines state that these patients need to be tested without specifying any strategy. No specific indications for PFTs in COVID-19 recovered patients are mentioned by the other Guidelines.
Patient management: measures to ensure social distancingTo safely restart PFTs services, it is mandatory to appropriately assess each outpatient, considering everyone as a potential symptomatic or asymptomatic COVID-19, avoiding at the same time denying access to many patients. All Guidelines are generally encouraging similar strategies to guarantee health safety, are implementing measures to warrant social distancing and to identify suspected patients for limiting the transmission of the infection, are ensuring the safety of health-care workers (HCWs) with adequate personal protective equipment (PPE), because subclinical patients may still transmit the virus.
Patient visitChinese,5 ITS/AIPO,19 IRS/SIP,20 and Irish Recommendations particularly emphasize that patients should be scheduled for a visit at a specific date and time, in order to avoid early arrival of the patient and crowded waiting rooms. The Irish Thoracic Society specifies that patients booked for a visit should wait in their own car, entering the department for testing only after a phone call by the administrative team.11 No mention of scheduled visits was formulated by ATS,6 BTS/ARTP,12 TSANZ/ANZSRS,14 SSP,8 SUNEUMO,18 SPLF,9 SEPAR/AEC/AET/SEAIC10 Societies.
Waiting roomsThe Recommendations generally encourage patients to come to the visit alone, without accompanying persons, when possible, or limited to one caregiver if they need support. Maintaining a minimum of 2m distance between sitting patients is recommended by Irish,11 Chinese,5 ITS/AIPO,19 ERS,17 and BTS/ARTP12 Societies, while SEPAR/AEC/AET/SEAIC limit the distance to at least 1m.
Furthermore, the Chinese task force,5 and ITS/AIPO19 Position Paper suggest making a demonstration video focused on the maneuvers for correctly performing spirometry and to project it in the waiting area, enabling patients to be prepared before the visit, while SEPAR/AEC/AET/SEAIC10 Societies recommend to use educational posters.
Patient entranceERS17 and ITS/AIPO,19 IRS/SIP,20 Portuguese,16 SPLF9 and Nebraska medical center15 Guidelines specify that patients coming to their visit should wear a mask, stressing that patients without a mask will not be allowed to enter the outpatient facility. SEPAR/AEC/AET/SEAIC10 Societies suggest wearing a mask only if patients have respiratory symptoms.
ScreeningAll the Guidelines besides ATS,6 TSANZ/ANZSRS14 and BTS/ARTP12 recommend administering a symptoms screening questionnaire to patient on arrival and checking body temperature, in order to verify if they are likely to have a COVID-19 infection. A sample screening questionnaire is provide by ERS,17 ITS/AIPO19 and IRS/SIP20 documents. ITS/AIPO,19 IRS/SIP,20 Irish11 and Chinese task force5 specify that the questionnaire, when possible, might also be administered by telephone (tele-screening) 48−72hours before the visit. Body temperature detection alone is recommended only by TSANZ/ANZSRS14 Guidelines: if the temperature is greater than 37.3°C, the visit will be suspended. No information on PPE to be used by the personnel during the triage is provided by any Guidelines. ITS/AIPO19 and IRS/SIP20 Guidelines strongly recommend a documented negative swab test 48−72h before PFTs for suspected cases, while ITS/AIPO19 Guidelines encourage physicians to arrange dedicated post-COVID-19 PFTs lab facilities.
Patient preparationAfter this screening phase, the patient will perform careful hand hygiene and enter the PFTs operative room; ITS/AIPO19 Guidelines specify that patients need to wear gloves too.
HCWs protectionThere is a lack of evidence about whether the PFTs should be considered aerosol-generating procedures. Nevertheless, HCWs assigned to PFTs lab should adopt all the precautionary measures suggested by WHO, since the procedure needs close contact with the patient and can induce coughing, similar to that induced by collecting diagnostic respiratory samples (e.g. nasopharyngeal swab). All Societies cautiously recommend PPE use for HCWs performing PFTs, specifying that HCWs should wear filtering facepiece respirators FFP3 or, when not available, FFP2 and eye protection. Only SPLF9 Guidelines state that HCWs can use a simple surgical mask. Changing disposable gloves between patients is highly recommended and rigorous hand hygiene is essential. BTS/ARTP12 Guidelines further specify that HCWs also need to wear a fluid-resistant gown and a disposable plastic apron, while IRS/SIP,20 SPLF9 and SEPAR/AEC/AET/SEAIC10 Guidelines mention only the gown. However, the Chinese task force5 and Portuguese8 Guidelines recommend the use of overshoes and surgical hats and replacing masks, gloves, and protective glasses if contaminated with saliva, sputum, and other secretions. Furthermore, Chinese task force,5 SEPAR/AEC/AET/SEAIC10 and ITS/AIPO Position Paper19 for an additional level of safety consider it appropriate that the chair direction of the PFTs operator should sit beside the patient, facing the same way, and recommend avoiding sitting face to face.
Equipment managementSpirometry systems are not designed to be sterile. There are three main potential sources of cross-contamination when performing the test: skin contact, aerosolized particles and saliva/body fluids; therefore, hygiene measures to protect users are crucial.
FilterThe ERS,17 BTS/ARTP,12 SEPAR/AEC/AET/SEAIC10 and ITS/AIPO19 Guidelines specify that in-line bacterial/viral filters should be used to protect the whole circuit from contamination with exhaled microorganisms, and the patient from inhaling particles from the circuit, while ATS,6 ITS11 and TSANZ/ANZSRS14 Guidelines do not specify any precaution in this regard.
To ensure the protective effect, BTS/ARTP 12 Guidelines recommend using in-line filters with a high-quality filtration performance against viruses but with proven evidence of not altering function measurements. Similarly, ITS/AIPO 19 and the Chinese Task force 5 state that verification of the total resistance of the filter and lung respiratory tube function instrument should be < 1.5 cmH2O at a flow rate of 14L·s−1, in order to not affect the results of the lung function test. At the same time, ERS 17 Guidelines suggest selecting a filter with a minimum proven efficiency for a high expiratory flow of 600–700L/min.
Interestingly, only the SPLF9 Guidelines recommend performing PFTs in a plethysmography boot with a shut door.
BronchodilatorAs far as bronchodilator challenge is concerned, TSANZ/ANZSRS14 Societies suggest using the patient’s own salbutamol inhaler or a single-use inhaler, while ITS11 Guidelines recommend considering the use of Turbohaler® or an aerosol holding chamber (spacer) device (i.e. aerochamber®), the latter also endorsed by the Portuguese Society.16
Equipment cleaningThe use of in-line filters does not preclude the necessity for thorough cleaning of the equipment. After each use, equipment cleaning with 75 % ethanol for 3min twice is recommended by the Chinese task force.17 SEPAR/AEC/AET/SEAIC10 and BTS/ARTP Guidelines12 also describe in detail the type of disinfectant solution, as shown in Table 1. A general statement regarding regular equipment cleaning protocol following local policies is advised by IRS/SIP.20
Nose-clipThe use of disposable nose clips is strongly recommended by ERS,17 BTS/ARTP,12 ITS/AIPO,19 IRS/SIP20 and SEPAR/AEC/AET/SEAIC10 Guidelines.
Environment managementVentilationAirborne transmission occurs through the dissemination of droplets from infectious patients; the motion of droplets significantly depends on gravity, direction and strength of local airflow, temperature, and relative humidity. It is crucial, therefore, to perform the spirometry in a properly ventilated room, in order to control any possible cross-infection. Ventilation is defined as the supply/distribution or removal of air from a space by mechanical or natural procedures. The clearance rate of aerosols in a closed space is dependent on the extent of any mechanical or natural ventilation; therefore, the greater the ventilation rate, expressed as the number of air changes per hour (ACH), the sooner any aerosol will be cleared.23 A single air change is estimated to remove 63% of airborne contaminants: after 5 air changes, less than 1% of airborne contamination is thought to remain.24 A minimum of 20min, that is 2 air changes, in hospital settings, where most of these procedures occurs, is considered pragmatic.25Nevertheless, the issue of adequate ventilation was considered only by ERS,17 ITS/AIPO,19 BTS/ARTP,12 Chinese task force,5 SUNEUMO18 and Nebraska Medical Center15 Recommendations. SEPAR/AEC/AET/SEAIC10 and Portuguese8 Guidelines generally suggest avoidance of air recycling.
In particular, adequate room ventilation, i.e. at least 15min to ventilate the room (open windows, closed doors), is recommended by SPLF,9 ERS17 and ITS/AIPO19 Guidelines. Negative isolation rooms with 6–12 ACH or side rooms with 6 ACH are encouraged by BTS/ARTP12 Guidelines.
The Nebraska Medical Center15 states that the procedure room should remain closed for an hour after the PFTs. The Chinese task force5 recommend maintaining the ventilation of the lung function examination room, ensuring 12 ACH if operating in a negative isolation room or an air flow of at least 160L / s per patient or hourly in a naturally ventilated room, as well as opening windows as much as possible for natural ventilation.
Chinese,5 SEPAR/AEC/AET/SEAIC10 and ITS/AIPO Guidelines19 proposed separating the test area from the administrative area of the room.
Room and surfaces cleaning and infection controlAll the reviewed Guidelines agreed on the importance of cleaning equipment and surfaces; SEPAR/AEC/AET/SEAIC,10 BTS/ARTP12 and Chinese5 Guidelines also recommend the type of cleaning solution to be used, Table 1.
Disposable cleaning wipes were strongly recommended by SEPAR/AEC/AET/SEAIC10 BTS/ARTP,12 ITS,11 and Cleveland Clinic21 Guidelines, but only TSANZ/ANZSRS14 and SEPAR/AEC/AET/SEAIC10 Guidelines expressly recommend the presence of minimal furnishings that can be easily cleaned and disinfected.14
As regards PFTs operating room cleaning, ERS17 ITS/AIPO19 and IRS/SIP20 Guidelines suggest the use of UV light or ozone room decontamination at intervals, compliant with local infection policies, while more detailed precautions are provided by the Chinese task force.5
The Chinese task force also recommend switching off the central air conditioner, sanitizing the room at least twice a day, using UV light for at least 30min a day to clean the air and medical air purification devices for air disinfection during lung function tests.
Waiting time between patientsThe suggested time required between visits by ERS,17 BTS/ARTP12 Guidelines is 30min for a regular side room and 60min for a negative isolation room. The Portuguese Society16 recommends a period time of 60min between visits and the Nebraska medical center15 specifies that the operating room must be closed for 1h after the visit.
Interesting suggestions come from ITS/AIPO19 and SPLF9 Guidelines that recommend a new calibration of the spirometer after the cleaning procedures, and from ERS,17 the only Society that takes into account high-risk patients, that suggest performing a remote test with live video instructions in these subgroups of patients.
A plan to manage the respiratory issues of people with acute respiratory symptoms, pre-existing chronic lung diseases or conditions that need adequate pulmonary function assessment to be appropriately diagnosed and treated, is essential to prevent an inevitably indirect effect of COVID-19 on frail patients that could be devastating, increasing death and disability.
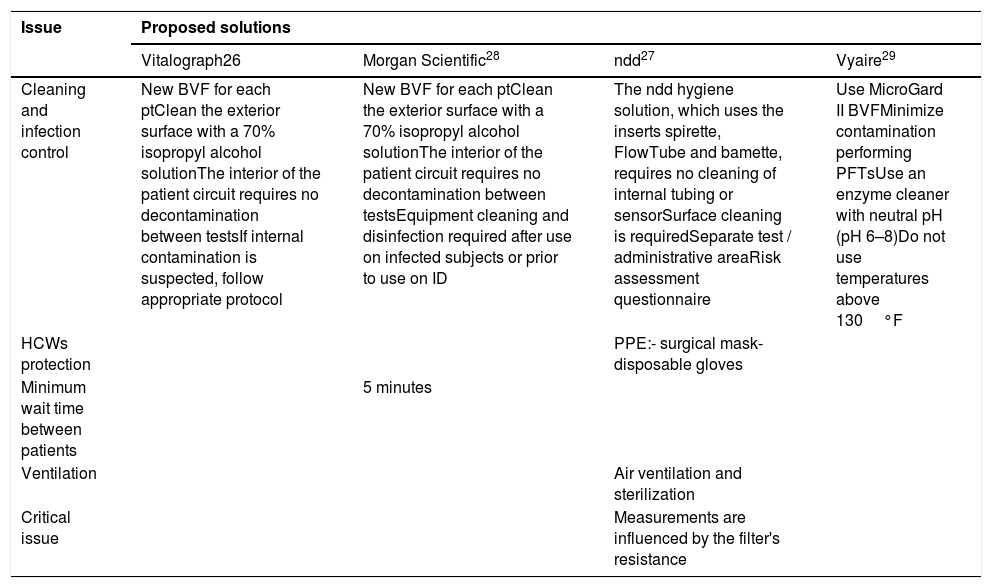
Manufacturers’ policiesManufacturers’ policies26–29 are summarized in Table 2.
Issues related to safely performing pulmonary function test: spirometry manufacturers’ proposed solutions.
| Issue | Proposed solutions | |||
|---|---|---|---|---|
| Vitalograph26 | Morgan Scientific28 | ndd27 | Vyaire29 | |
| Cleaning and infection control | New BVF for each ptClean the exterior surface with a 70% isopropyl alcohol solutionThe interior of the patient circuit requires no decontamination between testsIf internal contamination is suspected, follow appropriate protocol | New BVF for each ptClean the exterior surface with a 70% isopropyl alcohol solutionThe interior of the patient circuit requires no decontamination between testsEquipment cleaning and disinfection required after use on infected subjects or prior to use on ID | The ndd hygiene solution, which uses the inserts spirette, FlowTube and bamette, requires no cleaning of internal tubing or sensorSurface cleaning is requiredSeparate test / administrative areaRisk assessment questionnaire | Use MicroGard II BVFMinimize contamination performing PFTsUse an enzyme cleaner with neutral pH (pH 6–8)Do not use temperatures above 130°F |
| HCWs protection | PPE:- surgical mask- disposable gloves | |||
| Minimum wait time between patients | 5 minutes | |||
| Ventilation | Air ventilation and sterilization | |||
| Critical issue | Measurements are influenced by the filter's resistance | |||
List of Abbreviations: BVF: Bacterial Viral Filter; HCWs: health-care workers; ID: Immunocompromised patients; PFTs: Pulmonary Function Tests; PPE: personal protective equipment; Pt: patient.
The COVID-19 pandemic completely changed the routine of providing health-care services, shifting from elective to essential/acute management and limiting several diagnostic resources for chronic respiratory patients such as pulmonary function labs and sleep labs.30 We analyzed Society-specific clinical practice Guidelines on how to safely perform PFTs and the recommendation level of consensus for each clinically relevant problem; we found similarities but also several differences. In particular, the Societies’ Guidelines on spirometry during the COVID-19 outbreak differ greatly in relation to the subgroup of patients that need to be prioritized for testing.
The Guidelines agreed about prioritizing patients with urgent need to initiate treatment and pre-operative assessment, except Cleveland,21 which takes into account also pulmonary hypertension patients, IRS/SIP,20 which also considered patients with a diagnosis of pulmonary fibrosis and follow-up and for therapy prescription, as well as patients with a diagnosis of asthma and COPD, and Uruguayans18 Guidelines, providing indications also for pneumoconiosis and drug toxicity.
We identified a recommendation level of consensus on patient screening, on HCWs protection, and on the use of in-line filters for spirometry, but a little reference to adequate ventilation policies. No details on PPE that should be worn by the triage personnel were found, as well as no indications on how to safely perform spirometry using point of care portable spirometers with turbines in any National and International Guideline. ERS17 and BTS/ARTP12 Guidelines provided detailed information on when to perform PFTs in patients with a previous COVID-19 pneumonia, while IRS/SIP20 and ITS/AIPO19 Guidelines strongly recommend nasopharyngeal swab testing before the visit, probably taking into account only in-patients. The Chinese task force5 and ITS/AIPO19 Guidelines, interestingly, recommend providing an educational video on how to perform PFTs in the waiting rooms. ERS17 is the only Society that suggests the possibility of remote testing in very severely ill patients, “untethering” them from physical sites, promoting decentralized medical services. Manufacturers concentrate on in-detail technical issues, such as the type of in-line filters to be used or the cleaning procedures for the equipment of each product.
This review provides a summary of clinical practice Guidelines/Recommendations/Position Papers on practical problems that might arise worldwide during the safe reopening of respiratory outpatient services during COVID-19 pandemic, with a special focus on spirometry, but does not represent a Guideline itself. The main strength of this research is that all the reviewed Guidelines were published in the restricted time period of the COVID-19 outbreak, with publication dates ranging from 4, March 2020 to 12, May 2020. Therefore, the scientific evidence available when they were developed was almost the same for them all.
Differences in national healthcare systems, resource availability and different times of epidemic evolution might explain any dissimilarity in terms of consensus. However, the lack of specific COVID-19-related evidence could be another reason for heterogeneity of the Guidelines, mainly based on experts’ opinions rather than evidence-based recommendations. Furthermore, national and international recommendations may overlap due to the contribution of national representatives who possibly served also as the international experts in the Societies’ statement. Finally, although we have searched for national guidelines on spirometry resumption in four common languages (English, Spanish, French and Italian) we might have failed to detect recommendations of some Societies due to language restrictions.
ConclusionThe review of Guidelines/Recommendations/Position Papers indicate a good agreement in the need to prioritize patients for PFTs, patients screening, HCWs protection, and in the use of in-line filters for spirometry but poor consensus on the subgroup of patients considered a priority, and few indications on the measures to implement for adequate ventilation. We believe that this summary of the available literature may be a useful guide helping HCWs to select appropriate measures, tailored to the highly specific context in which they will be used, to meet the needs of intended users.
Authors’ contributionCC conceived the content, drafted the manuscript and approved the final version to be submitted. PI drafted the manuscript, approved the final version to be submitted. RC, SN, helped in writing the manuscript and approved the final version to be submitted. AS helped in writing the manuscript, revised it critically for important intellectual content and approved the final version to be submitted. NC conceived the content, revised it critically for important intellectual content and approved the final version to be submitted.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interestsAll authors declare no competing interests.
The authors thank Dr. Pietro Zucchi, medical writer, for improving the use of English in the manuscript.


