





To identify the prevalence of exposure to secondhand smoke (SHS) at home and in the car among children attending the 4th grade in Azores.
MethodsThis is a cross-sectional study that assessed children's exposure to SHS in a convenience sample of school children attending the 4th grade in all primary schools of Azores. The entire population of 4th graders from all elementary schools in Azores were asked to participate in the study (n=2463) in 2017. A validated self-reported questionnaire was administered to 2092 students who delivered the signed informed consent form. We analyzed frequencies, contingency tables, and performed Chi-square tests.
ResultsResults showed that 56.1% (95% CI 54.0–58.2) children reported having, at least, one smoking parent. Overall exposure to SHS at home was 38.4% (95% CI 36.3–40.6), and overall exposure to SHS in the car was 27.6% (95% CI 25.8–29.3). Children whose parents were smokers reported being more exposed to SHS at home (63.6%; 95% CI 58.6–68.3) than children whose parents were non-smokers (32.3%; 95% CI 30.2–34.6).
ConclusionThe results showed that the children's exposure to SHS in Azores is high and it tends to be higher than the prevalence found in mainland Portugal. Having parents who smoke is a major risk factor for children's exposure to SHS at home. These data justify a population-wide intervention plan for preventing tobacco consumption and children's exposure to SHS in Azores.
More than 600,000 non-smokers die each year worldwide due to secondhand smoke (SHS) and 28.0% of these deaths occur in children.1 Children and newborns are particularly vulnerable to the negative effects of SHS (such as pneumonia, ear infections and asthma), as their respiratory system and immune system are still developing.2,3
SHS exposure occurs, in most cases, when parents and/or other household member smoke at home and/or in the car. However, a study concluded that less than a fifth of parents implemented a total ban on smoking at home.4 A study conducted in nine Portuguese cities concluded that children's exposure to SHS at home was high, especially if their parents smoked.5 In addition to SHS exposure at home, children may also be exposed to SHS in the car.6 According to the European Commission, 13% of Portuguese smokers reported smoking inside the car, even with children on board.7
Portugal became a Party of the World Health Organization (WHO) Framework Convention on Tobacco Control in 2006. A new tobacco law was approved in 2007 that banned smoking in the workplaces and enclosed public spaces, although it allowed smoking in some restaurants or similar places. These exceptions are an obstacle to help the legislation achieve all the goals for which it was designed.5 This law also reinforced the creation of smoking cessation consultations in health centers and public hospitals. Still, Portugal has low tobacco control activity. Several authors report lack of public health campaigns, limited healthcare professionals’ leadership, and inconsistent smoke-free policy support.8 Thus, it is still necessary to devise a set of legislative, educational and therapeutic measures to protect children from the negative effects of SHS.9 In order to establish and implement effective interventions to prevent the exposure of children to SHS, it is important to estimate the prevalence of Portuguese children exposed to SHS at home and in the car. The exposure of children to SHS in mainland Portugal has been described through comprehensive studies, but there is no regional representative study on children's exposure to SHS in Azores (Portuguese island). This is particularly important, as the standardized mortality rate for trachea and lung tumors in Azores (51.2) is significantly higher than in mainland Portugal (23.2).10
Thus, this cross-sectional and regional study aimed to identify the prevalence of exposure to SHS at home and in the car among children attending the 4th grade in Azores.
MethodsParticipantsAll elementary schools in Azores (135 schools) were included in the study. In 2017, the total population of children attending the 4th grade at elementary schools in Azores was 2463 students. The 2463 students were approached to participate in the study, but the final sample included 2092 students, as 371 did not deliver the signed informed consent form. The collaboration rate was 84.9% (95% CI 83.5–86.3).
Thus, a total of 2092 students attending the 4th grade at elementary schools in Azores in 2017 participated in the study, of whom 1071 (51.3%; 95% CI 49.0–53.4) were male and 1018 (48.7%; 95% CI 46.6–51.0) were female (3 participants did not answer the question about gender). The mean age was 9.3 years (SD=0.7) and most of the participants lived in villages (41.1%; 95% CI 39.1–43.2). The majority of the sample (84.6%; 95% CI 83.1–86.2) lived in a nuclear family (with parents and siblings, or only with parents).
InstrumentsA self-reported questionnaire was administered to all participants. The questionnaire was based on the Changes in Child Exposure to Environmental Tobacco Smoke-Wales (CHETS) questionnaire, which has been validated for the Portuguese population and used in previous studies to assess children's exposure to SHS.11,12 The questionnaire contained multiple choice questions and open-ended questions. Core questions assessed: sociodemographic variables (age, gender, household members, parents’ level of education, place where children live), parental/other relatives smoking (e.g., Does your father/mother/brother(s)/other(s) family member(s) smoke? Answer: “does not smoke”, “yes, sometimes”, “yes, every day” or “I don’t know/I do not have any”), children's exposure to SHS at home (Family members and visitors’ permission to smoke at home (“does not smoke”, “yes, every day”, “yes, sometimes” and “does not smoke at home” or “I don’t know/I do not have any/does not live in my house), and children's exposure to SHS in the car (e.g., Does your father/mother/brother(s)/other(s) smoke in the family car? Answer: always”, “sometimes”, and “never”). Thus, like other studies, children's exposure to SHS at home and inside the car were measured according to the self-reported data given by children in relation to the questions mentioned above.5,13 The questionnaire was piloted among two classes of 4th grade students.
ProcedureThe study was approved by the Direção Regional de Prevenção e Combate às Dependências, and by the directors of the elementary schools included in the study. Teachers were trained by a researcher to administer the questionnaire in the classroom, according to a protocol that included practical instructions. Before the administration of the questionnaire, every participant was asked to deliver an informed consent form signed by their parents. The data collection took place in November 2017 in a single wave of data gathering that included all students from all elementary schools in Azores who delivered the signed informed consent form.
Statistical analysisData were analyzed using the Statistical Package for the Social Sciences (SPSS), 24.0 version for Windows. For statistical analysis, we analyzed frequencies, contingency tables, and performed Chi-square tests. We used bootstrap results based on 1000 bootstrap simple samples to calculate 95% confidence interval (95% CI). A significance level of 0.05 was considered.
ResultsFathers’ education level was inferior or equal to the 9th grade in 59.7% of the cases (95% CI 57.2–62.4); 19.2% completed the 12th grade (95% CI 17.1–21.3); and 21.1% had a college degree (95% CI 18.9–23.3). Mothers’ education level was inferior or equal to the 9th grade in 48.9% of the cases (95% CI 46.3–51.6); 26.0% completed the 12th grade (95% CI 23.7–28.3); and 25.2% had a college degree (95% CI 22.8–27.4).
Table 1 shows that 49.3% (95% CI 47.1–51.6) of the fathers and 29.0% (95% CI 27.1–31.0) of the mothers were smokers, and that more than half (56.1%; 95% CI 54.0–58.2) of the children had at least one smoking parent. The prevalence of mothers who smoked was lower than the prevalence of fathers who smoked.
Prevalence of smokers among children's household members.
| Smoker | Non-smoker | ||||||
|---|---|---|---|---|---|---|---|
| N | n | % | 95% CI | n | % | 95% CI | |
| Father | 1978 | 975 | 49.3 | 47.1–51.6 | 1003 | 50.7 | 48.4–52.8 |
| Mother | 2002 | 581 | 29.0 | 27.1–31.0 | 1421 | 71.0 | 69.1–73.0 |
| At least one parent | 2063 | 1157 | 56.1 | 54.0–58.2 | 906 | 43.9 | 41.8–45.9 |
| At least one household member | 2076 | 1308 | 63.0 | 61.1–65.0 | 768 | 37.0 | 34.9–39.1 |
CI: confidence interval.
Regarding children's exposure to SHS at home, Table 2 shows that 25.6% (95% CI 23.6–27.6) of children claimed that they were exposed to SHS as at least one their parents smoked at home. Children were more exposed to SHS at home due to fathers’ smoke (21.9%; 95% CI 20.0–23.7) than to mothers’ smoke (14.2%; 95% CI 12.6–15.8).
Prevalence of children's exposure to SHS at home considering family member smoking status.
| Smokes at home | Does not smoke at home | ||||||
|---|---|---|---|---|---|---|---|
| N | n | % | 95% CI | n | % | 95% CI | |
| Father | 1898 | 415 | 21.9 | 20.0–23.7 | 1483 | 78.1 | 76.2–80.0 |
| Mother | 1977 | 281 | 14.2 | 12.6–15.8 | 1696 | 85.8 | 84.2–87.3 |
| At least one parent | 2042 | 523 | 25.6 | 23.6–27.6 | 1519 | 74.4 | 72.6–76.3 |
| At least one household member | 2079 | 798 | 38.4 | 36.3–40.6 | 1281 | 61.6 | 59.5–63.7 |
CI: confidence interval.
Table 3 shows the results regarding children's overall exposure to SHS at home and in the car. Overall exposure at home was 38.4% (95% CI 36.1–40.8), and inside the car was 27.6% (95% CI 25.8–29.3). There were 373 (17.8%; 95% CI 16.4–19.8) children who reported being exposed to SHS at home and also inside the car.
Prevalence of children's overall exposure to SHS at home and/or inside the car.
| Daily/always | Occasionally/sometimes | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % | 95% CI | n | % | 95% CI | n | % | 95% CI | |
| At home | 2079 | 326 | 15.7 | 14.1–17.3 | 472 | 22.7 | 20.8–24.4 | 798 | 38.4 | 36.1–40.8 |
| Inside the car | 1966 | 102 | 5.2 | 4.2–6.2 | 440 | 22.4 | 20.6–24.3 | 542 | 27.6 | 25.8–29.3 |
| At home or in the car | 2090 | 358 | 17.1 | 15.6–18.6 | 609 | 29.1 | 27.3–31.1 | 967 | 46.3 | 44.2–48.6 |
| At home and in the car | 2090 | 70 | 3.3 | 2.6–4.2 | 303 | 14.5 | 13.0–16.1 | 373 | 17.8 | 16.4–19.8 |
CI: confidence interval.
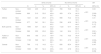
Table 4 shows significant differences in the children's exposure to SHS at home, comparing those with non-smoking parents and those with smoking parents. Children whose parents were smokers reported to be more exposed to SHS at home (63.6%; 95% CI 58.6–68.3) than children whose parents were not smokers (32.3%; 95% CI 30.2–34.6) (p<.001).
Prevalence of children's exposure to SHS at home, comparing those with non-smoking parents and those with smoking parents.
| SHS at home | No SHS at home | OR | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % | 95% CI | n | % | 95% CI | p | [95% CI] | ||
| Father | Non-smoker | 1003 | 235 | 23.4 | 20.9–26.1 | 768 | 76.6 | 73.9–79.1 | <.001 | 3.63 |
| Smoker | 969 | 510 | 52.6 | 49.4–55.7 | 459 | 47.4 | 44.3–50.6 | [2.99–4.40] | ||
| Mother | Non-smoker | 1421 | 423 | 29.8 | 27.5–32.1 | 998 | 70.2 | 67.9–72.5 | <.001 | 3.41 |
| Smoker | 577 | 341 | 59.1 | 55.4–63.3 | 236 | 40.9 | 36.7–44.6 | [2.79–4.17] | ||
| Both parents | Non-smoker | 1660 | 537 | 32.3 | 30.2–34.6 | 1123 | 67.7 | 65.4–69.8 | <.001 | 3.66 |
| Smoker | 396 | 252 | 63.6 | 58.6–68.3 | 144 | 36.4 | 31.7–41.4 | [2.91–4.60] | ||
| Father or Mother | Non-smoker | 906 | 190 | 21.0 | 18.4–23.6 | 716 | 79.0 | 76.4–81.6 | <.001 | 4.10 |
| Smoker | 1150 | 599 | 52.1 | 49.3–55.1 | 551 | 47.9 | 44.9–50.7 | [3.36–4.99] | ||
| Guests | Non-smoker | 768 | 112 | 14.6 | 12.1–17.2 | 656 | 85.4 | 82.8–87.9 | <.001 | 6.44 |
| Smoker | 1300 | 681 | 52.4 | 49.6–55.0 | 619 | 47.6 | 45.0–50.4 | [5.13–8.09] | ||
CI: confidence interval; OR: odds ratio.
This study aimed to be the first cross-sectional regional study using a convenience sample with a high collaboration rate to identify the prevalence of exposure to SHS at home and in the car among children attending the 4th grade in Azores.
The results showed that the prevalence of smokers among children's household members in Azores is high and it tends to be higher than the prevalence found in mainland Portugal.5 Also the standardized mortality rate for trachea and lung tumors in Azores is significantly higher than in mainland Portugal.10
Regarding the prevalence of children exposed to SHS at home in Azores, the results were similar to another study that found that the exposure to fathers’ smoke is more common than the exposure to the mothers’ smoke among Portuguese children.5
The results showed that the prevalence of children's exposure to SHS at home in Azores was higher than the prevalence found in Portugal (mainland and islands).14 Besides being exposed to SHS at home, children may also be exposed to SHS inside the car.6 The prevalence of SHS exposure inside the car found in the present study was similar to the prevalence found among 4th grade students in Portugal (mainland and islands).13
Comparing the subgroups with smoking and non-smoking parents, it was found that children whose parents were smokers reported being more exposed to SHS at home than children whose parents were not smokers. Thus, having parents who smoke is a major risk factor for children's exposure to SHS at home. This result was confirmed in other studies.5 These results highlight the need to raise awareness about the negative effects of SHS among parents and to implement measures to prevent it.5
One limitation of this study is that it relied on self-reported measures. Although the level of exposure to SHS can be assessed by the measurement of cotinine, nicotine metabolite, plasma, urine, saliva, and carbon monoxide in expired air, we decided to administer a questionnaire as it was more practical and economical. Biomarkers were not used due to budget constraints. Fifteen percent of the children did not obtained permission from their parents to participate in the study. As the probability of non-respondents having parents who smoke is high, children's exposure to SHS may be underestimated.
The tobacco law approved in 2007 was designed to protect non-smokers from SHS exposure in workplaces and public places. However, it is necessary to go further and develop a set of legislative, educational and therapeutic measures to protect children from the harmful effects of SHS.9 As the main source of children's exposure to SHS is parental smoking, it is crucial to implement effective parental smoking control measures. Banning smoking inside the car should be regarded as a way to protect children from exposure to SHS, and to avoid car accidents.15 Smoking control policies should also focus on health education campaigns at school and in community settings. Preventive programs targeting children are crucial to raise awareness about the importance of implementing smoke-free environments at home and in the car. Smoking cessation consultations should be reinforced in order to reduce the prevalence of parents who smoke and, consequently, prevent children's exposure to SHS. According to WHO guidelines, health professionals should approach systematically all tobacco users at each consultation and advise them to quit smoking; assess whether the patient wishes to make an attempt to quit and help him in his quit attempts; and schedule follow-up appointments.16 In fact, a minimal approach to smoking conducted by health professionals (that can last for about five to ten minutes) has been reported to achieve 5% to 10% smoking cessation rates.16
ConclusionsThe present study contributes to our understanding of the real situation of children's exposure to SHS in Azores. The high prevalence of children's exposure to SHS at home and in the car in Azores, as well as the high rates of mortality from lung cancer, justify a population-wide intervention plan to prevent tobacco consumption in this region.10,17 Therefore, it is our purpose to implement the school-based program “Domicílio e carros sem fumo” in all elementary schools in Azores.12
Authors’ contributionsJosé Precioso conceived this study and supervised all aspects of its implementation. Suzete Frias, Carla Natal Silva, and Filomena Gonçalves collected the data. José Cunha Machado and Isabel Sousa designed and carried out statistical analysis. Vânia Rocha revised the manuscript critically, wrote the final version and contributed to the interpretation of data for the work. All authors contributed substantially to the interpretation of data, critical discussion and revision of the manuscript, and approved the final version.
Conflict of interestThe authors declare no conflict of interest.


