


Six-minute walk test (6MWT) is used for evaluating functional exercise capacity. To the best of our knowledge, there are no reference equations to predict six-minute walk distance (6MWD) for the Portuguese population. The aims of the present study were to measure anthropometric data and 6MWD in a sample of healthy Portuguese population, to establish reference equations to predict 6MWD and to compare our equations with those obtained by previously published studies.
MethodsWe conducted an observational prospective study. We consecutively recruited 158 healthy 18–70 years old subjects from Porto district, who performed two 6MWTs using a standardized protocol. The best 6MWD was used for further analysis.
ResultsThe mean 6MWD was 627.8m (SD=73.3m). The variables that were significantly associated with the 6MWD were age, sex, BMI and ΔHR (Heart Rateat the end of the test−HRat rest). We found three explanatory models for 6MWD, the best with an explanatory power of 38%: 6MWD=721.7−1.6×Age−4.0×BMI+0.9×ΔHR+58.4×Sex. We verified that 6MWD decreased 1.6m per year of age, and 4.0m per unit of BMI and increased 0.892m per beat per minute. Moreover, on average, males walk 58.4m more than females (p<0.001). Applying equations from other studies to our population resulted in an overestimation or underestimation of the 6MWD.
ConclusionThe present study was the first to describe the 6MWD in healthy Portuguese people aged 18–70 years old and to propose predictive equations. These can contribute to improving the evaluation of Caucasian Mediterranean patients with diseases that affect their functional capacity.
Timed walking tests have been used for a long time to evaluate functional exercise performance.1–4 The six-minute walk test (6MWT) is a safe, simple, submaximal test, for evaluating functional exercise capacity, assessing prognosis and evaluating response to treatment across a wide range of respiratory diseases4–15; it reflects the capacity of the individual to perform activities of daily living.3,8–10 The six-minute walk distance (6MWD) is the primary outcome of the 6MWT, which is a reliable measure associated with death in some diseases.5–7,16–19 There is strong evidence of learning effect for the 6MWD when two or more 6MWT are conducted.1,6,7
Demographic, anthropometric, clinical, psychological and physiological characteristics can affect the test performance.5,16 Since 6MWT is a self-paced test, the results are influenced by external factors such as energy expenditure, clinician's/investigator's encouragement and subject's motivation.4,9,10,15,16,20
The American Thoracic Society (ATS) published the 6MWT guidelines, which aimed to standardize this procedure and encourage researchers to establish reference values for each population.5,11 During the last decade, several studies have elaborated 6MWT reference values,1,4,8–11,13–17,21–29 using different populations and 6MWT protocols.1,10,13,20 To the best of our knowledge, there are no reference equations for predicting 6MWD for the Portuguese population.
The aims of the present study were: to measure anthropometric data and 6MWD in a sample of healthy Portuguese population aged 18–70 years, according to the standardized approach provided by the ERS/ATS guidelines5,6; to establish reference equations to predict 6MWD; and to compare the 6MWD obtained with our reference equations to those obtained using previously published equations.27,28
MethodologyStudy design and subjectsThis was an observational, descriptive, prospective study, conducted in a Pulmonary Function Testing Laboratory, between January 2016 and December 2017.
We consecutively recruited 158 healthy subjects from 18 to 70 years old. All the subjects worked in the district of Porto. The birth place of the subjects was: Aveiro (10%), Braga (9%), Bragança (1%), Lisbon (7%), Portalegre (1%), Oporto (64%), Viana do Castelo (2%), Vila Real (3%) and unknown (3%). Most of the subjects were workers from a public hospital, students and workers at a local medical school. An informative letter was prepared clarifying the objectives of the study and the conditions for participation. This letter was sent by email to the employees of the hospital and the medical school. Accompanying people and patients, who were in consultations or undergoing outpatient examinations at the hospital for reasons other than those determined in the exclusion criteria, were also invited to participate in the study. Approval of the study was obtained from the hospital ethics committee, and written informed consent was given from each healthy subject before participation in the study.
The data obtained from each participant before undergoing 6MWT were: gender, age, height, weight, smoking history, medication use, medical history, physical examination, chronic obstructive pulmonary disease (COPD) Diagnostic Questionnaire (CDQ).30 The body mass index (BMI) was calculated by the standard formula.31
The exclusion criteria were: history of chronic disease that could influence the ability to perform physical exercises (e.g., impaired cognition, metabolic, cardiovascular, respiratory, neuromuscular or musculoskeletal diseases or use of walking aids); current or former-smokers; presence of respiratory symptoms, flu, or any other lung disease in the past 4 weeks; CDQ greater than 15,30 resting blood pressures higher than 150/100mmHg; resting heart rate (HR) higher than 100 beats per minute, BMI less than 18kg/m2 or greater than 30kg/m2, conditions that could affect walking, involvement in high competition sport; use of drugs that could affect muscle function and/or HR; ethnicity other than Caucasian.
Data collectionThe data were collected by two respiratory registrars and all 6MWT were performed by the same cardiopulmonary technician.
Prior to the 6MWT, age was confirmed, medical history and physical examination were completed, height, weight and blood pressure were evaluated and the CDQ was filled-in.
6MWTEach subject did two 6MWTs (6MWT1 and 6MWT2), with at least a 20-min rest between walks, according to the ERS/ATS guidelines.5,6 The 6MWTs were performed along a straight, flat, 30-m long corridor, with marks at 3m intervals. The 6MWTs were monitored by a single operator who recorded the 6MWD at the same time. A standard explanation was provided just before the first 6MWT. During the test, oxygen saturation and HR were measured by wearable transcutaneous pulse oximetry (Oximeter Nonin WristOx 2™, model 3150, Nonin, Plymouth, MN, USA), already validated.32 If subjects experienced dizziness, leg cramps, chest pain or dyspnea, they were permitted to stop and rest. At the end of each minute, subjects were given feedback on the elapsed time and standardized encouragement in the form of statements. Before and after each 6MWT, pulse rate, blood pressure, oxygen saturation, and Borg value were recorded. Subjects were asked to indicate their level of dyspnea perception using a modified Borg scale.33 The maximum predicted HR (mHR) was calculated as 220 minus age. The two distances walked by each subject were used for the learning effect analysis. The best 6MWD was used for the calculation of the reference equations. Measured 6MWD values were compared with predicted values using three reference equations devised for use in other populations.27,28
Statistical analysisQuantitative variables were reported as mean±standard deviation (SD). Sexes were compared using paired samples Student's t-tests. Correlation between variables was assessed using Pearson's or Spearman's correlation coefficients. Several multiple regression models were studied; gender was included as a binary variable (female=0, male=1) and all remaining variables as continuous; age in classes was categorized through dummy variables, taking as reference class the youngest age≤30. Collinearity was investigated based on the variable inflation factors. Normality of the residuals was evaluated through the Kolmogorov–Smirnov test. Sample size was determined based on G*Power (version 3.1.9.3), for a power of 80% and taking into consideration the number of predictors. All statistics were calculated using the IBM SPSS Statistics (version 24.0) software. A p-value was declared as significant for p<0.05.
ResultsDemographic, anthropometric and 6MWT resultsOf the 178 subjects recruited, 20 were excluded because of: smoking history (n=6), CDQ greater than 15 (n=4), involvement in high competition sport (n=4), ethnicity other than Caucasian (n=3), high blood pressure (n=2) and personal history of respiratory disease (n=1).
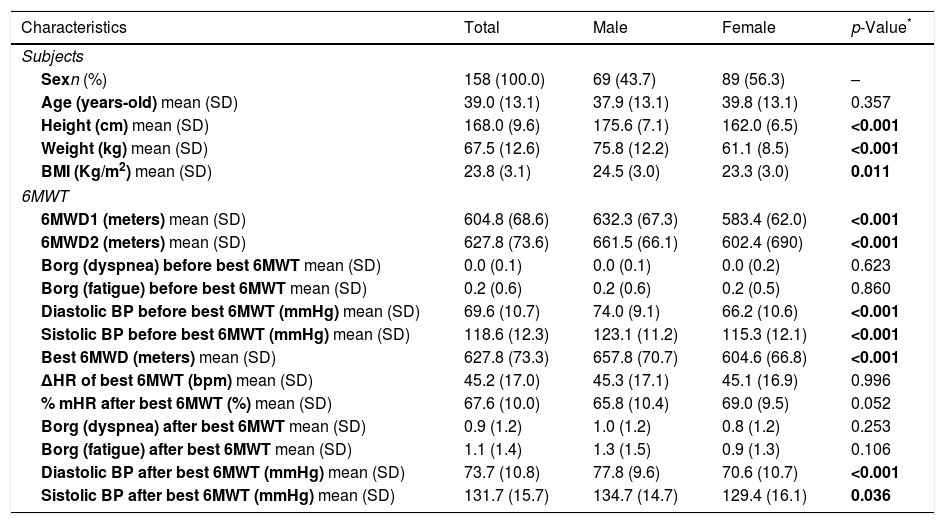
The characteristics of the healthy subjects and of the 6MWT measures are summarized in Table 1. There were significant differences between male and female subjects, with respect to anthropometric characteristics, since men were significantly taller, heavier and had higher BMI.
Characteristics of the study subjects and 6MWT measures.
| Characteristics | Total | Male | Female | p-Value* |
|---|---|---|---|---|
| Subjects | ||||
| Sexn (%) | 158 (100.0) | 69 (43.7) | 89 (56.3) | – |
| Age (years-old) mean (SD) | 39.0 (13.1) | 37.9 (13.1) | 39.8 (13.1) | 0.357 |
| Height (cm) mean (SD) | 168.0 (9.6) | 175.6 (7.1) | 162.0 (6.5) | <0.001 |
| Weight (kg) mean (SD) | 67.5 (12.6) | 75.8 (12.2) | 61.1 (8.5) | <0.001 |
| BMI (Kg/m2) mean (SD) | 23.8 (3.1) | 24.5 (3.0) | 23.3 (3.0) | 0.011 |
| 6MWT | ||||
| 6MWD1 (meters) mean (SD) | 604.8 (68.6) | 632.3 (67.3) | 583.4 (62.0) | <0.001 |
| 6MWD2 (meters) mean (SD) | 627.8 (73.6) | 661.5 (66.1) | 602.4 (690) | <0.001 |
| Borg (dyspnea) before best 6MWT mean (SD) | 0.0 (0.1) | 0.0 (0.1) | 0.0 (0.2) | 0.623 |
| Borg (fatigue) before best 6MWT mean (SD) | 0.2 (0.6) | 0.2 (0.6) | 0.2 (0.5) | 0.860 |
| Diastolic BP before best 6MWT (mmHg) mean (SD) | 69.6 (10.7) | 74.0 (9.1) | 66.2 (10.6) | <0.001 |
| Sistolic BP before best 6MWT (mmHg) mean (SD) | 118.6 (12.3) | 123.1 (11.2) | 115.3 (12.1) | <0.001 |
| Best 6MWD (meters) mean (SD) | 627.8 (73.3) | 657.8 (70.7) | 604.6 (66.8) | <0.001 |
| ΔHR of best 6MWT (bpm) mean (SD) | 45.2 (17.0) | 45.3 (17.1) | 45.1 (16.9) | 0.996 |
| % mHR after best 6MWT (%) mean (SD) | 67.6 (10.0) | 65.8 (10.4) | 69.0 (9.5) | 0.052 |
| Borg (dyspnea) after best 6MWT mean (SD) | 0.9 (1.2) | 1.0 (1.2) | 0.8 (1.2) | 0.253 |
| Borg (fatigue) after best 6MWT mean (SD) | 1.1 (1.4) | 1.3 (1.5) | 0.9 (1.3) | 0.106 |
| Diastolic BP after best 6MWT (mmHg) mean (SD) | 73.7 (10.8) | 77.8 (9.6) | 70.6 (10.7) | <0.001 |
| Sistolic BP after best 6MWT (mmHg) mean (SD) | 131.7 (15.7) | 134.7 (14.7) | 129.4 (16.1) | 0.036 |
The values in bold show significance of p<0.005.
p-Value between male and female subjects.
6MWT: six-minute walk test; 6MWD: six-minute walk distance; % mHR: percentage of the predicted maximum heart rate; BMI: body mass index; BP: blood pressure; BPM: beats per minute; cm: centimeters; HR: heart rate; ΔHR: difference between heart rate at the end and at the beginning of 6MWT; kg: kilograms; m: meters; SD: standard deviation.
No subject prematurely finished or interrupted the test. The difference of the distance covered between 6MWT1 and 6MWT2 was 21.6 (SD=26.2)m (95% confidence interval [CI]: 17.4–25.7), suggesting a learning effect; for males 24.9 (SD=25.6)m (95% CI: 18.7–31.2), for females 19.0 (SD=26.6)m (95% CI: 13.4–24.6). The mean 6MWD was 627.8 (SD=73.3)m (range, 453–831m), with significantly longer distances walked by males than females (p<0.001). Clinically significant oxygen desaturation was not observed during 6MWT.
Univariate and multiple regression analysisUnivariate regression models were developed to evaluate the most important relations between 6MWD and the explanatory variables recorded. The variables that were significantly associated with the 6MWD were: age, sex, BMI and ΔHR (Heart Rateat the end of the test−HRat rest) (Fig. 1).

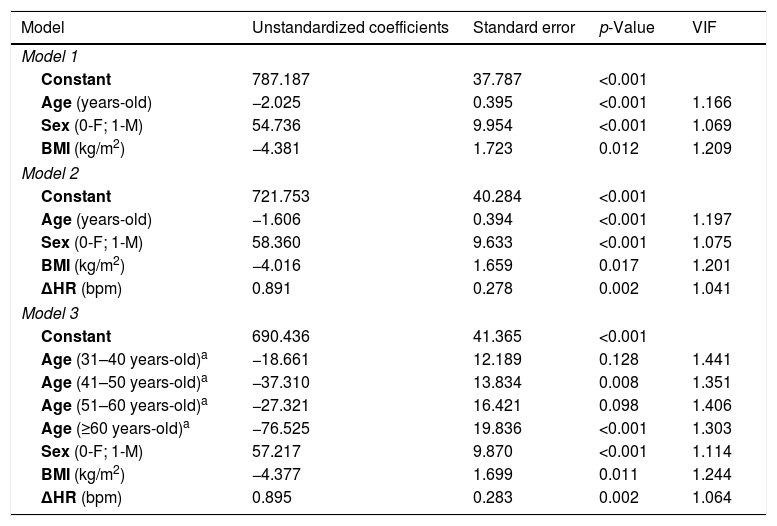
Several multiple regression models were tested, and three explanatory models were found for 6MWD. The first (Table 2) has an explanatory power of 34%, being simpler since it can be applied only with demographic and anthropometric variables (sex, age and BMI).

Multiple regression models 1, 2 and 3.
| Model | Unstandardized coefficients | Standard error | p-Value | VIF |
|---|---|---|---|---|
| Model 1 | ||||
| Constant | 787.187 | 37.787 | <0.001 | |
| Age (years-old) | −2.025 | 0.395 | <0.001 | 1.166 |
| Sex (0-F; 1-M) | 54.736 | 9.954 | <0.001 | 1.069 |
| BMI (kg/m2) | −4.381 | 1.723 | 0.012 | 1.209 |
| Model 2 | ||||
| Constant | 721.753 | 40.284 | <0.001 | |
| Age (years-old) | −1.606 | 0.394 | <0.001 | 1.197 |
| Sex (0-F; 1-M) | 58.360 | 9.633 | <0.001 | 1.075 |
| BMI (kg/m2) | −4.016 | 1.659 | 0.017 | 1.201 |
| ΔHR (bpm) | 0.891 | 0.278 | 0.002 | 1.041 |
| Model 3 | ||||
| Constant | 690.436 | 41.365 | <0.001 | |
| Age (31–40 years-old)a | −18.661 | 12.189 | 0.128 | 1.441 |
| Age (41–50 years-old)a | −37.310 | 13.834 | 0.008 | 1.351 |
| Age (51–60 years-old)a | −27.321 | 16.421 | 0.098 | 1.406 |
| Age (≥60 years-old)a | −76.525 | 19.836 | <0.001 | 1.303 |
| Sex (0-F; 1-M) | 57.217 | 9.870 | <0.001 | 1.114 |
| BMI (kg/m2) | −4.377 | 1.699 | 0.011 | 1.244 |
| ΔHR (bpm) | 0.895 | 0.283 | 0.002 | 1.064 |
All regression coefficients were significant, and it can be observed that the 6MWD decreases with age (approximately −2m per year of age) and BMI (approximately −4m per unit of BMI) and that there is a difference in the walked distance between males and females (approximately, 55m plus for males).
Refining the model with the introduction of ΔHR, we were able to increase the explanatory power to 38% which resulted in the second model (Table 2). From the multiple regression model 2, it can be concluded that the 6MWD decreases 1.6m per each year of age, and 4.0m with each unit of BMI. On the other hand, the distance increases 0.892m per each beat per minute. Moreover, it can be seen that, on average, males walk 58.4m more than females (p<0.001). These findings are in line with the ones of model 1, apart from small variations in the regression coefficients.

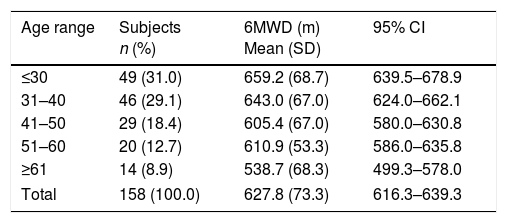
Regarding age range, per decade, it can be observed that the decrease in distance progresses with age; there was a significant difference with respect to the younger decade (≤30) from the age range 41–50 and ≥61, and close to significance in the age range 51–60 (Table 3). Taking into consideration that the maximal distance walked declines with age, a third multiple regression model was developed where age was categorized in decades (Table 2). In this model the coefficients associated with sex, BMI and ΔHR were very similar to the previous models. For this model, the residuals were also well behaved.
6MWD per age range.
| Age range | Subjects n (%) | 6MWD (m) Mean (SD) | 95% CI |
|---|---|---|---|
| ≤30 | 49 (31.0) | 659.2 (68.7) | 639.5–678.9 |
| 31–40 | 46 (29.1) | 643.0 (67.0) | 624.0–662.1 |
| 41–50 | 29 (18.4) | 605.4 (67.0) | 580.0–630.8 |
| 51–60 | 20 (12.7) | 610.9 (53.3) | 586.0–635.8 |
| ≥61 | 14 (8.9) | 538.7 (68.3) | 499.3–578.0 |
| Total | 158 (100.0) | 627.8 (73.3) | 616.3–639.3 |
6MWD: six-minute walk distance; CI: confidence interval; SD: standard deviation.
For all regression models, multicollinearity was assessed by the Variable Inflation Factor (VIF), which were all below 2, indicating that multicollinearity was not a problem. Likewise, for all models the residuals are also well behaved, uniformly distributed around zero and approximately normal (Kolmogorov–Smirnov test, p>0.2).
Comparison with published regression equations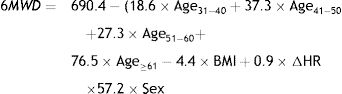
The regression equations from the models of Gibbons et al.27 and Britto et al.28 were developed on the same age range as our multiple regression model. Applying these equations to our data, showed that there was an overestimation of 157 meters with the Gibbons equation (only considering age and sex as explanatory variables),27 an underestimation of approximately 12 meters with Britto Eq. (1) (which considers age, age,2 sex and BMI),28 and an overestimation of 1 meter with Britto Eq. (2) (which considers age, sex, height and ΔHR).28
DiscussionTo the best of our knowledge, the present study was the first to describe the 6MWD in healthy Caucasian Mediterranean people aged 18–70 years-old and to present predictive equations.
The 6MWT is one of the several modalities available for the objective evaluation of functional exercise capacity.5 In our sample of healthy adults, no spirometry was performed because only subjects who never smoked and without respiratory diseases were included after applying a COPD Diagnostic Questionnaire.30 The original papers on reference values for the 6MWT (published in English) included: unhealthy individuals,23 six papers with age ranges greater than 4 decades4,10,17,20,26,29 and only eight had more than 150 individuals.1,11,14,17,21,25,28,29 In the present study, the 158 healthy subjects were balanced both by sex and decades of age.
The 6MWD is influenced by learning effect,1,5–7,11 being large enough to be clinically important.5 In order to avoid bias caused by the learning effect in our study, two standardized tests were performed, and the best of both was used in the analysis. Our results showed that 6MWT2 was, on average, 3% better than 6MWT1. 6MWT2 was higher than documented in the study of Casanova et al.,11 which included a population analysis of seven countries, but very similar to the data from 13 studies of COPD patients.7
There was a significant difference in the 6MWD between male and female, with men walking a greater distance than women. This may be due to the fact that men were significantly taller – a higher height is associated with a longer stride, which generates a longer distance.1,4,26,29 In addition, men have a greater absolute muscle strength and muscle mass.9,11,16
The average 6MWD measured in this study was relatively shorter than those of Caucasian studies20,22,24,27 and longer than those of North and South American1,9,13–15,28 and Asian studies.16,17,26,29 The explanation for these differences may lie not only in racial and demographic differences, but also in 6MWT methodology.
Age, sex, BMI and ΔHR were the most important factors that significantly influenced the 6MWD of our healthy subjects. Age is a variable that significantly influenced 6MWD in almost all29 previous studies on 6MWD reference equations. We found that age and BMI were negatively associated with the 6MWD. The negative association with age could be explained by the fact that muscle mass, muscle strength and maximal oxygen uptake gradually decreases with age.9,13,16 The six-minute walk work (6MWW) is the product of 6MWD and body weight. 6MWW increases with obesity; as a result, the obese walk shorter distances since changes in weight can significantly affect the energy requirement and, therefore, the amount of work performed.34 In our study, we found that the ΔHR was significantly positively associated with 6MWD, which may be because ΔHR represents the level of effort the subject expended while performing the test,17 the subjects who tried harder walking more. Another measure for level of effort may be the percentage of mHR, which in our study was 67.6%, a value lower than that described by Camarri et al. in a Caucasians study, where 6MWD was greater,20 reinforcing the idea that less effort may have influenced outcomes.
In the present study, three equations were derived for 6MWD in a sample of healthy Portuguese population aged 18–70 years old. The first proposed model seems advantageous given its simplicity. We considered the second model (with explanatory power of 38%), to be the reference equation for the Portuguese population aged 18–70 years old. In agreement with the literature,1,4,8–11,13–17,20–28 we verified that there was a decrease of 6MWD with increase in age. Consequently, it seemed pertinent to propose the third model in which the age range, by decade, was included.
The use of predictive equations for 6MWD created for populations other than the one studied, was associated with errors on the predicted distances. The difference between the measured and predicted 6MWD values might be caused by multiple factors. A systematic review identified many published studies from 1998 to 2017 that included 6MWD prediction equations from healthy adults.1,4,9–11,13–17,20–22,24–29 These studies were conducted using a wide variety of populations and methodologies. Casanova et al.11 studied a population of 7 countries, including Spain. In spite of having included a Mediterranean population, the conclusions reached by this group was that there were wide regional and geographic differences not explained by the variables used to obtain the reference equations. Thus, considering that a single reference equation was generated for a population of 6 American and one Mediterranean countries, we do not consider this equation to be representative of Mediterranean population. We selected the regression equations from the models of Gibbons et al.27 and Britto et al.,28 because these studies included populations with an age range similar to our study population. Applying the Gibbons and Britto equations, we found that there was an overestimation with the first and an underestimation with the equation 1 of the second one. Further, our study adds to the evidence that the predictive equations derived from other populations27,28 would not apply to Portuguese population.
Our research had some limitations: our sample may not be representative of the entire Portuguese population (although subjects were selected consecutively on the basis of inclusion criteria); the sample size was sufficient to elaborate a reference equation, but it was a relatively small sample, in particular the age group over 60 years old for which this test is widely used and has a particular interest (rehabilitation and exercise capacities in clinical groups); we did not recruit underweight and obese people, our reference equations are not applicable to the subjects with 18<BMI>30kg/m2 and although we have excluded high competition athletes we haven’t objectively measured physical activity. Despite the limitations, we found, for the first time, reference values for the 6MWD for Caucasian Mediterranean healthy population aged 18–70 years old.
ConclusionThe present study was the first to describe the 6MWD in healthy Portuguese people aged 18–70 years old and to propose predictive equations. Age, sex, BMI and ΔHR were the most significant predictors of the 6MWD and the regression equations explained approximately 34–38% of the variance in the 6MWD. We conclude that our equations can improve the evaluation of Caucasian Mediterranean patients with diseases that affect their functional capacity.
Author contributionsConceptualization: Miguel Guimarães, Maria João Oliveira.
Data curation: Maria João Oliveira, Raquel Marçôa, José Moutinho.
Formal analysis: Pedro Oliveira.
Writing: Maria João Oliveira, Raquel Marçôa, Pedro oliveira.
Writing±review & editing: Maria João Oliveira, Raquel Marçôa, Pedro Oliveira, José Moutinho, Inês Ladeira, Ricardo Lima and Miguel Guimarães.
Ethics statementThe protocol was approved by our ethics committee, and written informed consent was obtained from each patient prior to the study.
Statement of interestNone declared.
Conflicts of interestThe authors have no conflicts of interest to disclose.
The authors express sincere gratitude to Praxair, Institute of Biomedical Sciences Abel Salazar of the University of Porto, Vila Nova de Gaia Chest Disease Center and to all the subjects who participated in the present study.


