


Artificial stone slabs, composed of quartz sands and resin, are commonly used for kitchen and bathroom countertops. Workers handling this material are exposed to high levels of respirable crystalline silica (>90%) and have experienced an increase in silicosis cases with rapid disease onset within ten years of exposure.1 Diagnosis entails exposure history, radiographic detection, and exclusion of other causes. Chest computed tomography (CT) is more effective than X-ray for early diagnosis and preventing complicated silicosis. Reported CT findings associated with artificial stone-related silicosis range from non-specific indicators, such as ground-glass opacities, linear and irregular opacities, emphysema, and mediastinal lymphadenopathy, to more characteristic manifestations like centrilobular nodular opacities predominantly in the upper-posterior lung, nodular conglomeration, and large opacities with surrounding cicatricial emphysema.2
Following approval from the institutional review board at the National Taiwan University Hospital and informed consent from participants, a low dose chest CT examination was performed on 19 workers engaged in the production of artificial stone. Among these individuals, 12 exhibited abnormal CT opacities, and four displayed subpleural curvilinear lines in their upper lobes (Fig. 1). The estimated exposure levels to respirable crystalline silica for these four individuals (subjects 1–4) were 0.27, 0.77, 4.44, and 4.44 mg/m³, respectively, resulting in cumulative exposures of 1.35, 2.30, 13.32, and 26.64 mg/m³-year (Table 1). Subjects 1, 3, and 4 were raw material operators who blended quartz sand, resin, curing agents, and additives, and then molded these materials into the desired form. Subject 2 operated a water-suppressed grinding or polishing machine to customize and process artificial stone slabs. All four cases exhibited ground-glass opacities and scattered nodules. Chest X-rays revealed abnormalities only in subjects 1 and 4, both of whom also demonstrated large opacities. Lung function, including forced (forced expiratory volume at one second, FEV1; forced vital capacity, FVC) and static measures (total lung capacity, TLC; residual volume, RV), as well as diffusion capacity for carbon monoxide (DLco), was evaluated using spirometry, plethysmography, and single-breath methods. The Global Lung Initiatives calculator for Southeast Asian ethnicities (https://gli-calculator.ersnet.org/) was utilised to estimate predicted values and the lower limit of normal (LLN, 5th percentile). Subject 2 exhibited a mild obstructive ventilatory defect, characterised by an FEV1/FVC ratio less than the LLN. Subjects 1, 3, and 4 presented a mild restrictive ventilatory defect, as indicated by a TLC less than the LLN. All four subjects demonstrated mildly impaired diffusion capacity, defined by a DLco below the LLN. Both Subject 3 and Subject 4, who had a history of cigarette smoking, reported cumulative smoking quantities of 1.23 and 3.14 pack-years, respectively. All four subjects reported no underlying, physician-diagnosed conditions such as pulmonary tuberculosis, asthma, hypertension, cardiac disorders, diabetes, or autoimmune diseases. During field investigations, discrepancies were observed in the workers' adherence to proper respiratory protective equipment usage. This could potentially explain the absence of a clear linear relationship between exposure and imaging results for subjects 1 to 3.
 in the upper lung and other imaging features associated with silicosis. (A) Subject 1 exhibits scattered lung nodules (white arrow) and a large opacity in the right upper lung. (B) Subject 2 displays centrilobular nodules (white arrow). (C) Subject 3 presents ground-glass opacities and centrilobular nodules. (D) Subject 4 demonstrates scattered lung nodules (white arrow), ground-glass opacities, and a large opacity in the right upper lung.")
Low-dose chest CT images of four artificial stone manufacturing workers reveal subpleural curvilinear lines (black arrowhead) in the upper lung and other imaging features associated with silicosis. (A) Subject 1 exhibits scattered lung nodules (white arrow) and a large opacity in the right upper lung. (B) Subject 2 displays centrilobular nodules (white arrow). (C) Subject 3 presents ground-glass opacities and centrilobular nodules. (D) Subject 4 demonstrates scattered lung nodules (white arrow), ground-glass opacities, and a large opacity in the right upper lung.
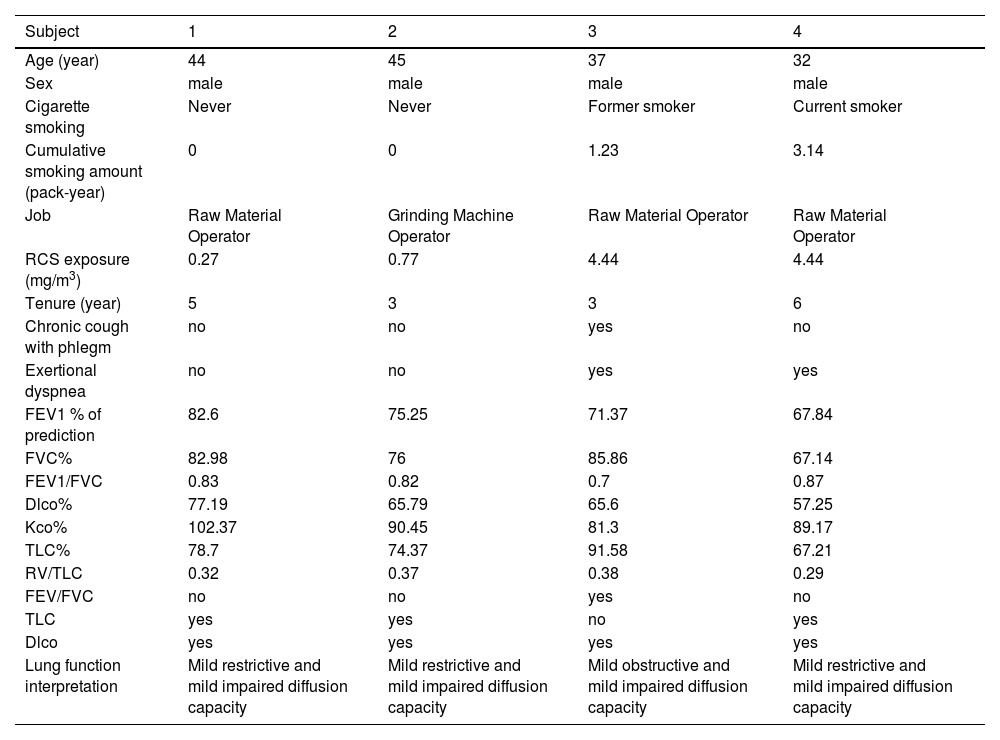
The characteristics and lung function indices of the patients.
Abbraviations: DLco%, percent of predicted diffusion capacity for carbon monoxide; FEV1%, percent of predicted forced expiratory volume at one second; FVC%, percent of predicted forced vital capacity; Kco%, percent of predicted carbon monoxide transfer coefficient; LLN, lower limit of normal. RCS, respirable crystalline silica; RV, residual volume; TLC%, percent of predicted total lung capacity.
Subpleural curvilinear lines, typically situated 2 to 3 mm from the inner chest wall, have been considered a distinguishing characteristic on chest CT, used to differentiate lung parenchyma affected by asbestos from idiopathic pulmonary fibrosis (IPF)3 or other interstitial lung diseases.4 Arakawa et al. have demonstrated the corresponding pathological feature of alveolar wall fibrosis of respiratory bronchioles in the subpleural area, aligning with the subpleural curvilinear lines observed in patients with asbestosis.4 This specific radiographic finding has not been reported in cases of silicosis. Upon revisiting previous literature, subpleural curvilinear lines were indeed present in the chest CT images of some reported cases,2 yet this finding had not been accorded significant attention in prior studies.
Subpleural curvilinear lines have been documented in non-dust-related diseases, such as COVID-19 pneumonia5 and interstitial lung diseases (comprising both IPF3 and non-IPF cases4,6). These lines are generally positioned 0.5 to 1 cm away from the inner chest wall in lower dependent lungs.3,5,6 In contrast, artificial stone silicosis is characterised by an upper predominant distribution and closer proximity to the inner chest wall (less than 0.5 cm), distinguishing it from other non-dust-related lung diseases. The subpleural distribution is hypothesised to be akin to that observed in asbestosis, potentially representing inflammation and fibrotic processes occurring near the small respiratory bronchioles.3,4 The upper lung distribution may be attributed to the relatively poor blood and lymphatic flow, hindering the clearance of inhaled dust particles.7
This study has several limitations that should be acknowledged. Firstly, the small sample size raises concerns about the generalizability of our findings. Secondly, the study design was uncontrolled, which limits our ability to clearly demonstrate relationships between exposure and disease. Lastly, the lack of follow-up data prevents us from understanding the long-term impacts of subpleural curvilinear lines on the disease, such as the progressive changes in imaging features and the complications that may arise from these changes. These limitations highlight the need for future research with larger sample sizes, controlled designs, and follow-up data to verify and expand upon our findings.
The presence of subpleural curvilinear lines in subjects with low cumulative silica concentrations and normal chest X-rays underscores their importance in the early diagnosis of artificial stone silicosis. The recognition of distinctive early imaging changes associated with the disease and exposure can facilitate the timely diagnosis of artificial stone silicosis, thereby enabling more effective interventions in occupational safety and health.
This study was supported by grants from the Institute of Labor, Occupational Safety, and Health, Ministry of Labor, R.O.C. (Taiwan). We express our gratitude to the field personnel who contributed to data collection and the workers who participated in this study.


