


An increasing number of peripheral pulmonary lesions (PPLs) requiring tissue verification to establish a definite diagnosis for further individualized management are detected due to the growing adoption of lung cancer screening by chest computed tomography (CT), especially low-dose CT. However, the morphological diagnosis of PPLs remains challenging. Transbronchial lung cryobiopsy (TBLC) that can retrieve larger specimens with more preserved cellular architecture and fewer crush artifacts in comparison with conventional transbronchial forceps biopsy (TBFB), as an emerging technology for diagnosing PPLs, has been demonstrated to have the potential to resolve the clinical dilemma pertaining to currently available sampling devices (e.g., forceps, needle and brush) and become a diagnostic cornerstone for PPLs. Of note, with the introduction of the 1.1 mm cryoprobe that will be more compatible with advanced bronchoscopic navigation techniques, such as radial endobronchial ultrasound (r-EBUS), virtual bronchoscopic navigation (VBN) and electromagnetic navigation bronchoscopy (ENB), the use of TBLC is expected to gain more popularity in the diagnosis of PPLs. While much remains for exploration using the TBLC technique for diagnosing PPLs, it can be envisaged that the emergence of additional studies with larger data accrual will hopefully add to the body of evidence in this field.
In recent years, there have been an increasing number of patients with peripheral pulmonary lesions (PPLs) that are being detected as a result of the growing adoption of chest computed tomography (CT) scans performed for lung cancer screening.1,2 Obtaining tissue from PPLs to establish an accurate diagnosis for both prognostic and therapeutic implications remains difficult to achieve. Whilst CT-guided transthoracic needle biopsy (CT-TTNB) previously served as the treatment of choice for identifying PPLs, with a superior diagnostic yield,3 there has been concern regarding a considerable complication rate (pneumothorax and pulmonary haemorrhage),4 which has limited further application of this technique. By comparison, minimally invasive bronchoscopic modalities, such as thin/ultrathin bronchoscopes, radial endobronchial ultrasound (r-EBUS), virtual bronchoscopic navigation (VBN), electromagnetic navigation bronchoscopy (ENB), cone beam CT, confocal laser endomicroscopy (CLE) and optical coherence tomography (OCT), have opened up a new way to diagnose PPLs and are emerging as safer alternatives to CT-TTNB.5-10 However, a suboptimal diagnostic yield for lesion sampling compared with CT-TTNB remains a significant limitation.11 One of the reasons for the insufficient diagnostic outcomes of such technologies is the use of sampling instruments.12 Specimens from PPLs obtained by transbronchial forceps biopsy (TBFB) are generally small and sometimes crushed, which may prevent a successful diagnosis and result in molecular testing failure.13
Transbronchial lung cryobiopsy (TBLC) that can yield larger tissue samples with better cellular architecture preservation and fewer crush artifacts via a tangential/lateral biopsy, as a novel tool for sampling PPLs, is frequently described for the evaluation of interstitial lung disease (ILD).14,15 In addition, placing an endobronchial blocker as the occlusion balloon at the start of the procedure, and the use of r-EBUS with a role of searching for blood vessels at the biopsy site and avoiding them during TBLC, may improve the safety of this technique in the diagnosis of PPLs.16 Given the potential benefits of TBLC, there is an increased focus on the use of TBLC for sampling PPLs, especially over the last 2 years. From studies to date, as promising as TBLC may be, this technique for diagnosing PPLs has not been standardized. We here present a comprehensive overview on the basis of the current literature and focus on the diagnostic yield, safety profile and the quantity and quality of specimen of TBLC in the setting of PPLs.
MethodsA comprehensive and systematical online literature search via PubMed, Web of Science, and EMBASE was performed to identify relevant articles from the date of inception to June 2023, using the following search terms: “cryobiopsy”, “lung”, “peripheral", and “diagnosis”. We also searched specifically for “transbronchial lung cryobiopsy” and “peripheral pulmonary lesions”. Furthermore, we performed an extensive manual screening of reference lists of the selected articles to capture further papers of interest. The aforementioned procedure was conducted repeatedly until all relevant articles were retrieved. Written informed consent was obtained from the patient with the provision of images.
Technical outlineTransbronchial lung cryobiopsy (TBLC) requires a cryoprobe that is an insulated catheter inserted through the working channel of a flexible bronchoscope and can extend to the lung periphery through the bronchoscope. The distal metal tip of the cryoprobe cools to a temperature of –79°C (using carbon dioxide) or –89°C (using nitrous oxide) within seconds, which is mediated by the Joule-Thomson effect where the cryoprobe uses compressed gas that is decompressed within its metallic tip, and thereby causing the cooling.17,18 As a consequence, TBLC allows for a 360-degree biopsy, enabling the bronchoscopist to obtain larger tissue specimens with a minimized crush artifact, thereby allowing pathologists to easily identify the immunohistochemical and molecular characteristics of PPLs, which are common in non-small cell lung cancer (NSCLC).19,20
Fig. 1 illustrates the details of r-EBUS guided TBLC. Prior to the procedure, a solitary pulmonary nodule with a positive CT bronchus sign in the left lower lobe was determined on the CT scan. Following moderate-to-deep conscious sedation with intravenous midazolam and fentanyl, a 20-MHz r-EBUS probe with an external diameter of 1.4 mm (UM-S20-17S; Olympus, Tokyo, Japan) was extended into the lung periphery through the working channel of the bronchoscope. r-EBUS imaging showing a concentric lesion (i.e., the r-EBUS probe was within and completely surrounded by the lesion) with no significant surrounding vessels. An endobronchial blocker was then placed at the target segmental bronchi. Subsequently, cryobiopsy was performed (ERBE Cryoprobe 1.9 mm diameter, Medizintechnik, Tuebingen, Germany) with the foot pedal switch of Cryostation being activated for 5 s. The cryoprobe was quickly retracted en bloc together with the flexible bronchoscope from the patient. Upon removal of the cryoprobe, the pre-placed endobronchial blocker was inflated with air immediately in order to control bleeding after procedure. All biopsy specimens were fixed in formalin and sent to the pathology lab immediately for further analysis. Immunohistochemical and molecular analysis revealed lung adenocarcinoma with sensitizing epidermal growth factor receptor (EGFR) mutation.
 guided by radial endobronchial ultrasound (r-EBUS).(a) Computed tomography (CT) scan of the chest showing a solitary pulmonary nodule located in the left lower lobe; (b) The placement of the r-EBUS probe into the target bronchus; (c) r-EBUS imaging showing a concentric lesion with no significant surrounding vessels; (d) An endobronchial blocker is placed in the proximal lobar bronchus from the lesion and is inflated after procedure; (e) The placement of the cryo-probe into the target bronchus; (f) Bioptic specimens with sizing scale collected through TBLC; (g) Immunohistochemical analysis revealing lung adenocarcinoma.")
Details of transbronchial lung cryobiopsy (TBLC) guided by radial endobronchial ultrasound (r-EBUS).(a) Computed tomography (CT) scan of the chest showing a solitary pulmonary nodule located in the left lower lobe; (b) The placement of the r-EBUS probe into the target bronchus; (c) r-EBUS imaging showing a concentric lesion with no significant surrounding vessels; (d) An endobronchial blocker is placed in the proximal lobar bronchus from the lesion and is inflated after procedure; (e) The placement of the cryo-probe into the target bronchus; (f) Bioptic specimens with sizing scale collected through TBLC; (g) Immunohistochemical analysis revealing lung adenocarcinoma.
Where all the previous studies of TBLC are almost confined to ILD,21,22 Schuhmann et al.17 evaluated for the first time the use of TBLC in patients with PPLs in 2014. In the randomized trial, a total of 31 patients whose lesions could be detected by r-EBUS were randomly assigned to each group; 16 patients undergoing TBLC and 15 patients undergoing TBFB were analyzed. The diagnostic yields were 74.2% and 61.3% for TBLC and TBFB, respectively. Although the statistical difference in yield between both groups was not significant (P=0.42), the increasing trend seemed attractive. Since then, a growing body of studies have highlighted the role of TBLC for the diagnosis of PPLs. Tanaka et al.23 performed a prospective study involving 50 cases to investigate the utilization of TBLC for PPLs, using a new 1.7-mm cryoprobe. Diagnostic yield was reported at 94%, it was notable, however, that there was no statistically significant difference between the 1.1 mm and 1.9 mm cryoprobes used in ILD regarding diagnostic yield, according to recent report from Ravaglia et al.24 Several studies have compared TBLC to TBFB in the diagnosis of PPLs during the same procedure.25-40 A prospective control study whereby patients underwent both TBLC and TBFB revealed diagnostic rates of 75.00% and 64.52%, respectively; when taking only the first sample into account, the diagnostic yield of TBLC (64.29%) was higher than that of TBFB (35.48%).25 Similarly, Torky and colleagues demonstrated diagnostic accuracies of TBLC and TBFB were 76.7% and 69.8%, respectively; when both were combined the yield increased further to 86.7%.26 To date, the largest series which consisted of 2, 724 cases with a propensity score analysis indicated that the diagnostic yield was significantly higher in the TBLC group than in the TBFB group (89.2% vs. 77.6%, P < 0.001).27 Moreover, TBLC has been shown to improve diagnostic yield of PPLs when used in addition to other conventional devices, including TBFB, transbronchial needle aspiration (TBNA) and transbronchial brushing.28,41 Worth noting was that for PPLs less than 2 cm in diameter, TBLC presented an additional benefit with a relatively high diagnostic yield ranging from 69.0% to 76.5%.29,42,43 A prospective study of 32 patients compared the influence of TBLC and TBFB on the diagnosis of PPLs smaller than 20 mm. The diagnostic yield of TBLC was 69% vs. 38% with TBFB (P = 0.044),42 which could be reported in larger series of 152 PPLs patients.29 Also of note is that for eccentrically and adjacently oriented lesions with a suboptimal diagnostic yield for TBFB due to inadequate depth of the forceps biopsy, a number of studies have demonstrated encouraging diagnostic yield with a range of 74.0% to 84.3%, which significantly improves compared to TBFB.29-32,41,44
Rapid on-site evaluation (ROSE) with the aid of conventional microscopy and higher harmonic generation microscopy allowing rapid stain and real-time assessment for direct slides,45,46 because of its high specificity (90.0%) and positive predictive value (93.8%), was considered to be a potential tool in deciding whether TBLC could be finished in a case series of 63 patients with PPLs.47 A meta-analysis by Sryma and colleagues from 9 studies that included 300 patients between 2014 and 2020 compared TBLC to TBFB when combined with r-EBUS for the diagnosis of PPLs.11 TBLC resulted in a higher diagnostic yield than TBFB (77% vs 72%, respectively); however, the statistical difference observed was not significant. This may be attributed to 1.9 mm cryoprobe used in all studies of this meta-analysis. It was reported that the addition of a guide sheath (GS) allowing for cryobiopsy at the same location provided an additional diagnostic gain to TBLC33; its use was, nevertheless, not routinely possible in most cases with a non-ultrathin cryoprobe, as it could hamper this procedure. Another limitation is that the non-ultrathin cryoprobe restricted by the thickness and stiffness of their tip made it difficult to approach some locations such as the subpleural areas and the apical segment of the upper lobe.40 Although special techniques including the crawling up and cryoprobe bending method have been created and demonstrated to be useful for pushing the cryoprobe into the upper field of the lung,41,48 they mostly depended on the bronchoscopists’ individual experience. Also, it is necessary to remove the tissue sample, bronchoscope en bloc, and non-ultrathin cryoprobe from the patient when specimen is adhered to it, which is adverse to repeat biopsy.11
Hopefully, a novel commercially available 1.1 mm ultrathin cryoprobe with increased flexibility that can be used with a 1.95 mm GS in a 2.0 mm working channel has been developed to address the diagnostic dilemma of the non-ultrathin cryoprobe for PPLs. A landmark study was done by Yarmus et al.49 in 2016, who first reported the use of 1.1 mm ultrathin cryoprobe through the GS and leaving the GS in situ, with the bronchoscope remaining inside the airway. They demonstrated that this technique was feasible without a significant bleeding risk, however, the pilot study only focused on a porcine model. Subsequently, the feasibility of the ultrathin cryoprobe in the clinical setting was first described by Kho and colleagues in 2020, and they demonstrated that the ultrathin cryoprobe had a dramatic improvement over the non-ultrathin cryoprobe when diagnosing PPLs located in the apical segment of upper lobes.50 Jiang et al.51 retrospectively evaluated 20 PPLs patients with 23 ground-glass opacity lesions (GGOs) (12 pure GGOs, 11 mixed GGOs) who underwent TBLC using a new 1.1-mm diameter cryoprobe, and eventually diagnosis was established in 82.6% of GGOs. The considerable diagnostic yield of the ultrathin cryoprobe for PPLs with GGOs that are relatively difficult to diagnose by TBFB, may be attributed to the fact that detailed information related to alveolar structures can be provided by TBLC. In addition to lesions located in the upper lobe and GGOs, the superiority of 1.1 mm ultrathin cryoprobe in diagnosing lesions near the pleura could be also observed when compared with 1.9 mm conventional cryoprobe.23,52 In order to evaluate the clinical outcomes of TBLC using the ultrathin cryoprobe for the diagnosis of PPLs, Kim et al.53 performed the prospective observational pilot study in which they sampled 50 PPLs and were able to achieve 45 positive samples with a yield of 90%. Furthermore, a comparative study conducted by Chung and colleagues retrospectively examined a consecutive series of 229 patients who underwent TBLC with an ultrathin cryoprobe and TBFB; results indicated that the diagnostic yields of TBLC and TBFB were 84.4% and 65.3%, respectively; when both were combined the overall diagnostic yield increased further to 91.5%.31 It is well established that despite good accessibility to the targeted PPLs, especially combined with advanced bronchoscopic navigation technologies, ultrathin bronchoscopy fails to obtain the large size of biopsy specimens owing to the restricted size of the biopsy instrument.54 Fortunately, the ultrathin cryoprobe inserted through the working channel of the ultrathin bronchoscopy makes up the deficiency. The use of the ultrathin cryoprobe in combination with ultrathin bronchoscopy was first reported by Oki and colleagues in 2022. They demonstrated that TBLC, TBFB and the combination of these two methods provided a definitive diagnosis in 62%, 54%, and 74% of patients with PPLs, respectively.35
Radial endobronchial ultrasound (r-EBUS) confirming the location of the target PPLs is always used when performing TBLC. One major limitation regarding r-EBUS is the absence of real-time guidance during TBLC, a certain amount of tissue samples remain nondiagnostic, which can be overcome by the combination with advanced bronchoscopic navigation techniques.17 The unique characteristics of the 1.1 mm cryoprobe enable TBLC under guidance techniques, such as VBN, ENB and robotic-assisted bronchoscopy platforms.49 The first study performed TBLC, TBFB and TBNA using the Ion™ Endoluminal System in 112 patients with 120 PPLs. The overall diagnostic yield of 90% was reported, and nearly 18% of diagnoses were made exclusively from TBLC.36 A subsequent study evaluated the Monarch™ platform in 58 PPLs patients with a median lesion size of 15mm. 94.8% of the PPLs was successfully localized using r-EBUS, however a diagnostic yield of 74% was reported.44 As encouraging as the results of both studies may be, the use of guidance techniques, especially robotic-assisted bronchoscopy is associated with high economic costs; therefore, evaluation of cost-effectiveness is essential.55 Additionally, the combination of transthoracic ultrasound and flexible cryoprobe has been reported to be a simple, feasible and reproducible modality with low cost and bedside availability for the diagnosis of PPLs, making it a potential surrogate for hospitals with cost-benefit consideration.56 To better confirm these findings, further prospective studies in a larger patient cohort are required.
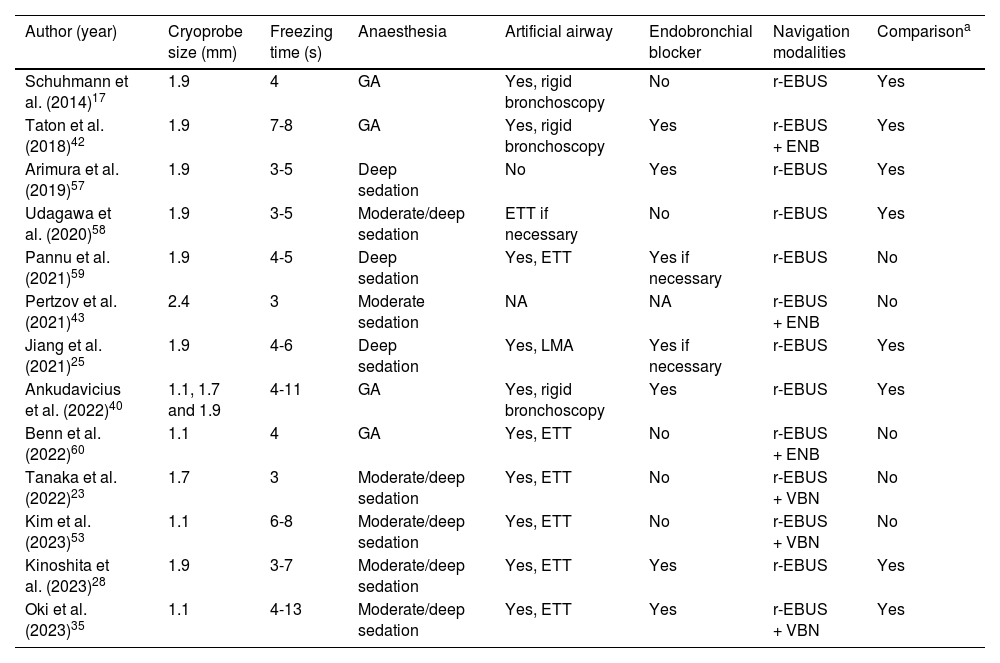
It should be emphasized that the disposable design of the 1.1 mm ultrathin cryoprobe may be cost-prohibitive. Plus, some studies showed that the 1.1 mm and 1.9 mm cryoprobes have similar diagnostic performance for PPLs.37,49 Hence, their use in the clinical field should be based on various factors, such as lesion characteristics and cost-effectiveness. The main characteristics of the prospective trials that describe the utility of TBLC for the diagnosis of PPLs are summarized in Table 1.
Procedural characteristics of prospective trials of TBLC for PPLs.
| Author (year) | Cryoprobe size (mm) | Freezing time (s) | Anaesthesia | Artificial airway | Endobronchial blocker | Navigation modalities | Comparisona |
|---|---|---|---|---|---|---|---|
| Schuhmann et al. (2014)17 | 1.9 | 4 | GA | Yes, rigid bronchoscopy | No | r-EBUS | Yes |
| Taton et al. (2018)42 | 1.9 | 7-8 | GA | Yes, rigid bronchoscopy | Yes | r-EBUS + ENB | Yes |
| Arimura et al. (2019)57 | 1.9 | 3-5 | Deep sedation | No | Yes | r-EBUS | Yes |
| Udagawa et al. (2020)58 | 1.9 | 3-5 | Moderate/deep sedation | ETT if necessary | No | r-EBUS | Yes |
| Pannu et al. (2021)59 | 1.9 | 4-5 | Deep sedation | Yes, ETT | Yes if necessary | r-EBUS | No |
| Pertzov et al. (2021)43 | 2.4 | 3 | Moderate sedation | NA | NA | r-EBUS + ENB | No |
| Jiang et al. (2021)25 | 1.9 | 4-6 | Deep sedation | Yes, LMA | Yes if necessary | r-EBUS | Yes |
| Ankudavicius et al. (2022)40 | 1.1, 1.7 and 1.9 | 4-11 | GA | Yes, rigid bronchoscopy | Yes | r-EBUS | Yes |
| Benn et al. (2022)60 | 1.1 | 4 | GA | Yes, ETT | No | r-EBUS + ENB | No |
| Tanaka et al. (2022)23 | 1.7 | 3 | Moderate/deep sedation | Yes, ETT | No | r-EBUS + VBN | No |
| Kim et al. (2023)53 | 1.1 | 6-8 | Moderate/deep sedation | Yes, ETT | No | r-EBUS + VBN | No |
| Kinoshita et al. (2023)28 | 1.9 | 3-7 | Moderate/deep sedation | Yes, ETT | Yes | r-EBUS | Yes |
| Oki et al. (2023)35 | 1.1 | 4-13 | Moderate/deep sedation | Yes, ETT | Yes | r-EBUS + VBN | Yes |
TBLC: peripheral pulmonary lesions. TBLC: transbronchial lung cryobiopsy. GA: general anaesthesia. r-EBUS: radial endobronchial ultrasound. ENB: electromagnetic navigation bronchoscopy. ETT: endotracheal tube. NA: not applicable. LMA: laryngeal mask airway. VBN: virtual bronchoscopic navigation.
In view of the safety profile of TBLC in the evaluation of ILD, concerns associated with bleeding and pneumothorax have been raised when using TBLC for patients with PPLs.14 Indeed, a meta-analysis involving 9 articles on the application of TBLC in PPLs demonstrated that TBLC-related complications reported were mainly mild to moderate bleeding that settled with the negative pressure suction, local adrenaline instillation or ice adrenaline dilution, and severe bleeding and pneumothorax were only observed after procedure in 1 (0.5%) and 3 (1.4%) of 222 patients, respectively.11 Another meta-analysis of 39 studies conducted by Giri and colleagues compared TBLC and TBFB for the diagnosis of PPLs with respect to utility and safety, showing that TBLC was associated with a significant increase in the incidence of moderate to severe bleeding (OR, 2.17; 95% CI, 1.48–3.19; P < 0.01) based on the unified bleeding grade,61 however, no significant difference was observed in the incidence of pneumothorax between the TBLC and TBFB groups (OR, 0.90; 95% CI, 0.44–1.85; P = 0.78).62 Consequently, bleeding has been of particular concern. In recent years, there has been increased interest in the use of precautionary interventions to control bleeding caused by TBLC.63
As the commonest type of technique used in the guidance of a bronchoscope to PPLs,64 r-EBUS can also identify vascular areas that are hyperechoic, thereby mitigating the risk of bleeding during TBLC in patients with PPLs by manoeuvring the probe to the least vascular area.65 A prospective randomized double-blind pilot trial by Pannu and colleagues assessing the utility of r-EBUS in minimizing bleeding from TBLC showed trends of less severe grade of bleeding towards the decreased grade of bleeding, less time spent to control bleeding and less need for additional interventions were observed under r-EBUS guidance.59 Due to the anticipated higher bleeding risk based on the TBLC data in ILD,66 rigid bronchoscope, endotracheal tube (ETT) and an endobronchial blocker have generally been used to provide airway protection in case of unpredictable bleeding for TBLC of PPLs.67-70 Nevertheless, the use of rigid bronchoscope or ETT is time-consuming and resource intensive, which could be a hindrance for the widespread adoption of this diagnostic modality at majority of centers with a lack of rigid bronchoscopy expertise and intubation skills.71,72 Plus, the presence of an endobronchial blocker during TBLC may be detrimental for the diagnosis of PPLs because it interferes with bronchoscope manipulation and prevents the devices such as r-EBUS, GS, and the cryoprobe guiding into the correct bronchus route toward the targeted PPLs. Recently, the two-scope technique, as a novel alternative method of hemostasis for TBLC of PPLs, have been described to allow the prompt control of bleeding and flexible manipulation of devices during the procedure instead of using an endobronchial blocker; but to date, a direct comparison between the two-scope method and the prophylactic balloon occlusion technique for TBLC is still absent.38 Surprisingly, all aforementioned measures being implemented to control and prevent bleeding are expected to be revolutionized by the introduction of the new 1.1 mm cryoprobe. It is well recognized that the previously used 1.9 mm cryoprobe needs to be removed from the patient with the specimen, GS, and bronchoscope en bloc, on account of the larger size of the tissue sample. As such, the blind period between extracting the cryobiopsy and bronchoscope reinsertion during TBLC, where bleeding may be occurring but unattended, is unbeneficial to early monitoring of bleeding.73 The 1.1 mm cryoprobe could be removed through the GS whilst keeping the bronchoscope and GS in situ, similar to conventional r-EBUS guided TBFB, where the GS provides some measure of mechanical tamponade, and simultaneously the bronchoscope is consistently in the airway to deal with any bleeding, effectively reducing the risk of bleeding.49,74 To confirm the safety of the 1.1 mm cryobiopsy use through the r-EBUS GS, without rigid bronchoscopy, ETT and an endobronchial blocker, additional studies are obviously required.
Immunohistochemical and molecular testingWith the emergence of precision medicine for lung cancer, target therapy and immunotherapy improving the prognosis of NSCLC have revolutionized the management of these patients; however, this has led to more urgent requirement for adequate quantity and quality of specimens.75-77 Apart from helping to provide consistent personalised management for patients with lymphoproliferative disorders,78 mediastinal lymph nodal involvement for oncologic reasons79,80, and Covid-19 via complete immunohistochemical and molecular analysis,81-83 TBLC retrieving the larger size of the tissue samples with more preserved cellular architecture and less biopsy artefacts has opened possibilities for increasing personalization of antineoplastic treatments. Several studies have reported that TBLC yielded significantly larger specimens than TBLB in the diagnosis of PPLs.11,17,28,29,35,39,40,42,57,58,62 As for different sizes of cryoprobes, it has been reported that the sample size obtained by 1.1 mm cryoprobe was comparable to that with 1.9 mm cryoprobe.52 Haentschel et al.84 evaluated the detection rate of EGFR mutations in TBLC specimens in comparison to specimens obtained by non-TBLC techniques (TBFB, TBNA and CT-TTNB) in NSCLC patients. Their retrospective analysis showed that cryobiopsy might be able to substantially increase the number of NSCLC patients that could receive targeted therapy, by increasing the detection rate of molecular genetic alterations (TBLC, 21.6% vs. non-TBLC, 13.8%, respectively). Remarkably, an exploratory randomized study performed by Herath and colleagues suggested that all positive TBLC specimens for malignancy were capable of EGFR mutation analysis.72 Furthermore, freezing and thawing during TBLC had virtually no effect on the immunohistochemical results of the expression of HER2 and HER3, according to the study by Nishimatsu et al.85 Importantly, prospective data from Udagawa and colleagues revealed the significantly higher success rates for whole-exome sequencing (TBLC, 90% vs TBFB, 15%, respectively) and RNA sequencing (75% vs 10%, respectively).58 In other studies, that the success rate of NGS for TBLC specimens was 100% has also been reported.28,57 The aforementioned results could be explained by the fact that larger amounts of DNA and RNA could be extracted from TBLC specimens compared to TBFB specimens.57,68,8687 Moreover, tumor cell necrosis that is not always a disadvantage when using immunohistochemical techniques may serve as a factor for failed NGS results, but r-EBUS avoiding TBLC in areas with necrotic lesions plays a role in increasing the NGS success rate, which could not be ignored.28,88,89
For NSCLC patients with the absence of targeted molecular alterations, immune checkpoint inhibitor (ICI) could be essential for a better survival rate.90 The expression of programmed death ligand 1 (PD-L1) serves as an important predictor for the effect of ICIs.91 Arimura et al.86 attempted to evaluate the tumor cell count in specimens collected by TBLC and TBFB, in 16 patients with PPLs. The total and average numbers of tumor cells obtained by TBLC were significantly larger than those obtained by TBFB. TBLC also had the tendency to yield greater rates of both PD-L1 expression >1% (TBLC, 18.8% vs TBFB, 12.5%, respectively) and >50% (56.3% vs 37.5%, respectively), in line with another prospective study,58 as well as the latest data from one participating institution.85 It was noted that despite being cut in half one of the tissue samples obtained by TBLC contained sufficient DNA and RNA to successfully perform molecular analysis, even the other tissue sample was sufficient for the evaluation of PD-L1 expression.57,86
A research group from the German Centre for Lung Research reported the 5-year experience of prospective biomaterial acquisition in advanced NSCLC. They demonstrated that obtaining the cryoconserved biopsies was feasible in 89% of the treatment-naïve NSCLC patients and in particular, the highest tissue amounts received were through cryobiopsies compared to core- and forceps biopsies. In the future, routine collection of cryopreserved tissue specimens may play a promising role in significantly extending the possibilities of optimized molecular workup of NSCLC and maximizing the benefit of targeted therapy and immunotherapy, thereby improving the quality of life and prognosis of the patient.92 Also, lung cancer organoids (LCOs) mimicking the tumor microenvironment have the potential to predict the response to targeted and immunology therapies, and there are still many challenges, such as a low success rate for culturing LCOs due to small amounts of tissue specimens obtained by conventional lung biopsy techniques and few cancer cells in later passages of LCO culture owing to the overgrowth of normal lung cells.93 Hopefully, LCOs derived from TBLC with the ability of providing enough specimens with high purity of cancer cells have been proven to be a breakthrough method for offering a promising solution to the critical limitations associated with conventional LCOs in the routine clinical practice,87 which seems attractive and was worth all the effort.
ConclusionsTransbronchial lung cryobiopsy (TBLC) contributing not only to the increased success rate in reaching a conclusive diagnosis without affecting safety but also to improved biopsy quality for potential molecular-based selection of personalized therapeutic strategy, has been an important supplement to the armamentarium of interventional pulmonology and a promising first-line tool for the diagnosis of patients with PPLs. For a benign diagnosis in particular, the pathologist can obtain additional confidence in establishing a definite benign diagnosis due to the ample TBLC samples. Additionally, with the introduction of the 1.1 mm cryoprobe that will be more compatible with advanced bronchoscopic navigation techniques, the use of TBLC is expected to gain more popularity in the diagnosis of PPLs.
However, several technical issues related to TBLC remain to be addressed. First, the use of an endobronchial blocker, anesthesia and artificial airway varied across studies. Standardizing the procedural technique is, therefore, necessary for promoting widespread utilization of this procedure. Second, there is a learning curve for sampling PPLs using TBLC that improves with case experience. A structured education has been recommended for improving the operator's technical expertise.94–96 Udagawa et al.58 suggested that approximately 20 procedures might be required for a pulmonologist to acquire the desired level of expertise in this technique, but 30 procedures were recommended in another study.40 Accordingly, the learning curve of the procedure is still in need to be clarified. Third, although TBLC has been demonstrated to increase diagnostic yield of PPLs in combination with other conventional biopsy methods, such as TBFB and TBNA,26,28,31,35,41 the optimal sequence of biopsy methods has not been established. Finally, for the optimum freezing times and number of TBLC performed to make a balance between larger specimen and fewer complications, various authors described different modalities. According to the clinical evidence of the published studies, the following recommendations can be made: the freezing time should be set at 2-5s for each biopsy and 2–4 biopsies should be performed in each procedure.23,25,40,43,44,48,60,86 In large-scale clinical practice, however, the optimum freezing times and number of TBLC for PPLs remain to be defined.
While much remains to be explored using the TBLC technique for diagnosing PPLs, hopefully the emergence of additional studies with larger data accrual will add to the body of evidence in this field. Furthermore, we have to emphasize that TBLC is solely a component of an integrated management for patients with PPLs; with the idea of incorporating the advantages and minimizing the disadvantages of every single technique, a multimodal approach for PPLs in which TBLC can be combined with other conventional devices and advanced bronchoscopy navigation techniques should be the preferred strategy.
ContributorsY.T. contributed to conceptualization, data curation, and manuscript drafting. S.T. contributed to conceptualization, figure realization, manuscript drafting. H.C. contributed to literature search, data curation, and manuscript revision. X.L. contributed to conceptualization and table realization. X.P., X.Z., Y.Z. and Y.L. offered critical suggestions to this article. H.H. and C.B. contributed to supervision of this manuscript and reviewed the manuscript. All authors read and approved the final version of the manuscript.


