



Excessive delay in the diagnosis of Tuberculosis may have a negative impact on the epidemiological control and elimination of this disease. An accurate determination and analysis of delay times may help identify where and how to improve Tuberculosis diagnosis according to local needs. The Portuguese Tuberculosis Surveillance System – SVIG-TB – is the main source of data regarding diagnosis delay. However, to our knowledge, there has been no recent evaluation of its data. This study's primary aim was to conduct a thorough quantitative and qualitative evaluation of data obtained from the SVIG-TB registry concerning the delay in Tuberculosis diagnosis in Matosinhos, a Portuguese municipality.
MethodsAll patients living in the Matosinhos municipality diagnosed with Tuberculosis between January 1st 2012 and December 31st 2019 were identified and individual SVIG-TB records retrieved. Patient-related, Healthcare-related and Total delay in Tuberculosis diagnosis were determined based on data obtained from this source and compared to data recovered from patient record review. Missing data, registering errors and differences in diagnosis delay between these two sources were analysed and compared. Subsequently, diagnosis delay data from a recent Portuguese nationwide SVIG-TB paper, covering years 2010 to 2014, was compared to local SVIG-TB and patient record review data.
ResultsThis study identified a significantly greater percentage of cases with missing data on delay in SVIG-TB records when compared to Patient Record Review (57.2% versus 1.11%). The median patient-related, healthcare-related and Total delay in Tuberculosis diagnosis were of 17, 30 and 68 days, respectively, in the SVIG-TB based data. A significant underestimation of healthcare-related and total Tuberculosis diagnosis delay was identified in SVIG-TB data when compared to Patient Record Review. There was no significant difference between Patient-related delays determined from these two sources. Compared to the national study results, missing values were more common in this data set (57.2 vs 44.6%), mainly due to the absence of patient-related delay data. Median Total and Healthcare-related delays were significantly greater in Matosinhos Municipality, regardless of the data source (SVIG-TB or Patient Record Review). The patient-related delay was, conversely, shorter.
ConclusionsSVIG-TB has been crucial in guiding National Public Health policies on the path towards Tuberculosis elimination in Portugal. However, there is still room for improvement. These results provide a basis for further reflection on the shortcomings and potential of SVIG-TB in guiding the national Tuberculosis program.
Despite consistent and effective national Public Health policies towards the elimination of Tuberculosis (TB), Portugal maintains one of the highest incidences of this disease in Western Europe.1 In Portugal, Outpatient TB Clinics have the specific task of TB diagnosis, treatment and prevention. However, TB may be diagnosed in any healthcare setting, ranging from public to private institutions, primary, secondary and even tertiary care establishments with ensuing referral to the former for follow-up.
The Portuguese national surveillance system, “SVIG-TB”, has allowed for the systematic collection of standardized epidemiological data on TB for over two decades.
This surveillance system's main aim is to obtain follow-up data regarding susceptibility testing, microbiological evolution, and treatment regimens. It has been essential in the epidemiological understanding and control of this disease in Portugal.
Within the data collected from SVIG-TB, dates of patient symptom detection, first patient healthcare visit, and diagnosis/treatment initiation allow for the calculation of total, patient and healthcare-related delays in TB diagnosis. Records of this information are subject to bias and error from both the patient reporting (mainly recall bias) and the healthcare professional registering this data.
Excessive diagnosis delay is one of the identified obstacles to adequate epidemiological control of TB (especially of its transmissible presentations) since it may have a negative impact on its severity, mortality-rate, and duration of disease transmission, which may, in turn, increase contact exposure and infection, undermining the control and elimination of this disease in the short and long-term.2
Several studies have analysed delay in TB diagnosis in different country settings.3,4,5,6,7 In 2019, Zão et al. analysed TB diagnosis delay in Portugal based on SVIG-TB data.8 In this report, approximately 44.6% of cases had missing delay data, still allowing for some broad conclusions on this subject. The considerable percentage of cases excluded from this analysis due to missing data and the unknown accuracy of the recorded (time) data may limit the interpretation and generalizability of its results.
A recent paper by Li et al. reports the existence of discordance between two TB data sources and medical records in China's National TB Surveillance System regarding several key variables, including date of diagnosis.9 Diagnosis delay data, however, was not mentioned in this article.
The World Health Organization recommends regular assessment and audit of national TB registries to ensure the validity of its data10, particularly before basing policy and healthcare measures on its results.
To the best of our knowledge, there have been no recent studies evaluating the quantitative and qualitative characteristics of data in TB registries specifically concerning TB diagnosis delay, either Portugal or internationally.
This study's main aim was to conduct a thorough quantitative and qualitative evaluation of data obtained from the SVIG-TB registry regarding the delay in TB diagnosis in Matosinhos, a local Municipality with one of the highest TB incidences in Portugal (according to the most recent available statistics from 2018: 21.66 vs 16.6/100 000).11,12
MethodsAll patients living in the Matosinhos municipality locally diagnosed with Tuberculosis between January 1st 2012 and December 31st 2019 were identified based on the local Outpatient TB Clinic records and national SVIG-TB database.
SVIG-TB includes two forms which are preferably completed by the healthcare worker responsible for TB diagnosis or treatment initiation, and treatment follow-up thereafter. In most cases, however, these forms are filled in at the Outpatient TB Clinic. They are considered a reliable and representative source of data both at a national level and in this particular municipality.
SVIG-TB forms from each patient were retrieved, and all included data was registered.
Data extracted from SVIG-TB forms for this particular study included, among others:
- -
Date of patient symptom detection (A) - date of onset of symptoms reported by the patient§;
- -
Date of the first patient healthcare visit (B) - date of the first visit to any healthcare facility, after symptom onset§;
- -
Date of diagnosis/treatment initiation (C) - date of TB treatment initiation; whenever this date is unknown, diagnosis date should be registered§;
When all of these dates were available, the following time delays were calculated:
- -
Patient-related delay in TB diagnosis = [B – A]
- -
Healthcare-related delay in TB diagnosis = [C – B]
- -
Total delay in TB diagnosis = [C – A]
The absence of any of these dates limited the total or partial inference of correlated delays – therefore regarded as “missing data”.
Whenever patients were asymptomatic on first observation in the healthcare setting yet presented radiological abnormalities, subsequently identified as being of Tuberculosis aetiology, “date of patient symptom detection” did not apply. In these cases, the Patient delay was therefore not considered and Total diagnosis delay was considered equal to Healthcare-related delay.
All data extracted from SVIG-TB forms was subsequently completed or corrected based mainly on a thorough Patient Record Review. All collected data was available within the patients' records on the SVIG-TB forms were originally completed and accessible to Healthcare workers initially filling them in. This revised data set was compared with recorded SVIG-TB data.
The collected data evaluated and compared included (among others):
- -
Percentage of missing data
- -
Percentage of identifiable errors in reporting
- -
(Inferred) Median Patient-related delay
- -
(Inferred) Median Healthcare-related delay
- -
(Inferred) Median Total delay in TB diagnosis
The proportion of Missing data in SVIG-TB and Patient Record Review data was compared using Related-Samples McNemar Change Test.
Subsequently, patients' characteristics associated with greater missing values in SVIG-TB data were extracted using Fisher's exact test for categorical variables and T-test for continuous variables.
For descriptive analysis of SVIG-TB and Patient Record Review delay data, the median and interquartile range (IQR) delay values were calculated. Non-parametric, 2–tailed Wilcoxon signed-rank test for median comparisons were applied initially on the total sample to compare delay data from both data sources.
Furthermore, Complete Case Analysis ensured better accuracy excluding cases with “negative” delays and selecting cases where there was no missing data in both samples. Non-parametric tests for related samples were applied to compare Patient-related, Healthcare-related, and Total median delays obtained from SVIG-TB and Patient Record Review data.
In a recent survey, diagnosis delay data from Portuguese national SVIG-TB reports, covering years 2010 to 2014, was obtained and analysed.8 A brief comparison between our current data and results gathered from these SVIG-TB national records was considered relevant despite originating from slightly different, yet partially overlapping time-frames. Non-parametric, 2–tailed Wilcoxon signed-rank test for median comparisons was applied to compare Matosinhos’ delay results from each local data source with national SVIG-TB delay data.
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS), version 26. P-values were assumed significant if less than 0.05.
All data was collected after approval from the local Healthcare [Unidade Local de Saúde Matosinhos (ULSM)] Ethics committee.
ResultsA total of 380 patients were identified in local Outpatient TB Clinic records and SVIG-TB forms. Fourteen cases were excluded due to residence outside the Matosinhos municipality, while six were excluded due to ulterior rejection of TB diagnosis.
There was a clear predominance of male patients (64.7%) and the most commonly affected organs were the lungs: 76.7% of TB cases affected the lung, while 23.3% were exclusively extrapulmonary TB cases. Patient age assumed a roughly normal distribution with a median of 51 years of age [IQ 39.67].
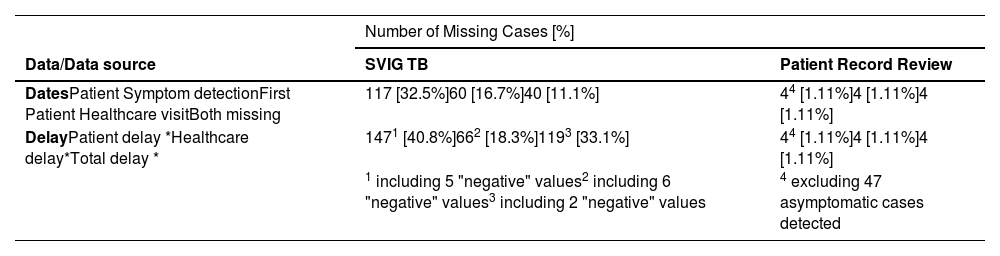
Missing data and reporting errorsWithin the selected 360 cases, no data on the date of diagnosis/treatment initiation was missing from either data sources. Conversely, 32.5% of data from SVIG-TB forms regarding the date of Initial Patient Symptom detection, 16.7% regarding first Patient Healthcare visit and 11.1% regarding both were missing. These missing dates, in turn, impaired delay calculation for these patients (Table 1). In a few cases, “negative” delay values were inferred, suggesting the existence of additional errors in the filling in of SVIG-TB forms and thus excluding them from further analysis (these cases are detailed in Table A.1). In total, 206 (57.2%) cases lacked at least one source of data regarding diagnosis delay in SVIG-TB forms: 147 in patient delay, 66 in Healthcare-related delay and 119 in Total delay.
Missing Cases from SVIG-TB and Patient Record Review sources. Total population = 360; (*p < 0.001).
| Number of Missing Cases [%] | ||
|---|---|---|
| Data/Data source | SVIG TB | Patient Record Review |
| DatesPatient Symptom detectionFirst Patient Healthcare visitBoth missing | 117 [32.5%]60 [16.7%]40 [11.1%] | 44 [1.11%]4 [1.11%]4 [1.11%] |
| DelayPatient delay *Healthcare delay*Total delay * | 1471 [40.8%]662 [18.3%]1193 [33.1%] | 44 [1.11%]4 [1.11%]4 [1.11%] |
| 1 including 5 "negative" values2 including 6 "negative" values3 including 2 "negative" values | 4 excluding 47 asymptomatic cases detected | |
On Patient Record Review missing delay data was significantly decreased to a total of 4 cases in each of these three groups (p < 0.001). Further analysis evidenced 47 asymptomatic patients on first observation in the healthcare setting having, however, at that date abnormal radiological exam results, later identified as being caused by TB. Several of these cases occurred in the setting of contact-screening initiatives.
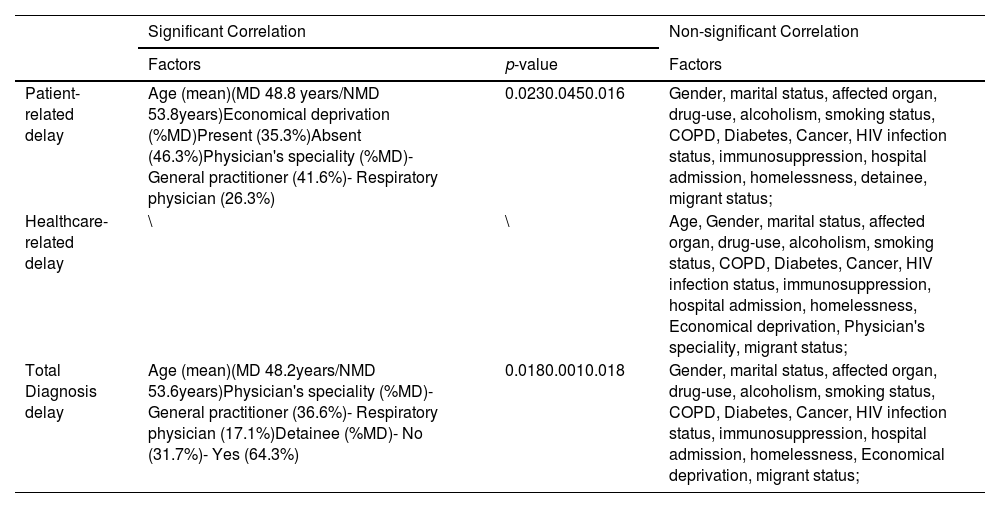
Detailed comparison of the patient population with and without missing delay data in SVIG-TB records evidenced general similarities between them, except for a few factors (the most relevant variables analysed are available in Table 2). Missing data concerning Patient-related delay was significantly more common in younger patients, economically deprived patients, and in SVIG-TB forms completed by General Practitioners (as opposed to respiratory physicians). Missing data concerning Total diagnosis delay was significantly more frequent among younger patients, detainees and in SVIG -TB forms filled in by General Practitioners. There were no significant differences between patient populations with and without Healthcare-related delay missing data.
Missing values and analysis of correlated factors.
MD – Cases with Missing data
NMD – Cases with Non-Missing data
The median patient-related, healthcare-related and Total delay in TB diagnosis were of 17 [IQR 46], 30 [IQR 68.25] and 68 [IQR 100,5] days, respectively, in the SVIG-TB based data. On the other hand, in the Patient Record Review data these delays were, respectively, of 18 [IQR 42], 68 [IQR 136.5], and 100 [IQR 137.5] days (Table 3).
Summary of median delay results and Interquartile range [IQR] from three different sources: local SVIG-TB forms, Patient Record Review and National SVIG-TB survey.7
| Data Source | Patient-related | Healthcare-related | Total delay | |||
|---|---|---|---|---|---|---|
| n | Median Delay [IQR] | n | Median Delay [IQR] | n | Median Delay [IQR] | |
| SVIG-TB | 213 | 17 [46] | 294 | 30 [68.25] | 241 | 68 [100.5] |
| Patient Record Review | 310 | 18 [42] | 356 | 68 [136.5] | 356 | 100 [137.5] |
| National SVIG-TB Survey7 | 6838 | 33 [51] | 6838 | 17 [40] | 6838 | 68 [72] |
A preliminary analysis, including all available data from both data sources, revealed significantly shorter median delays based on SVIG-TB registers when compared to Patient Record Review data (p ≤ 0.01; Table A.2). This disparity in results could be partly justified by the absence of data from a large sample of cases in SVIG-TB records when compared to Patient Record Review, particularly when significant differences were identified in the population with and without missing values, as previously described – a possible source of an unforeseen selection bias.
To correct for this “asymmetry” and further improve the accuracy in result comparison, a Complete Case Analysis approach was adopted. Only cases where data was available from both sources, after exclusion of “negative” delays, were compared: 190 cases in Patient delay, 290 cases in Healthcare delay, and 238 cases in Total delay (Table 4).
Complete Case Analysis allowed for the identification of significant differences between Healthcare and Total median delays obtained from SVIG-TB and Patient Record Review data (p < 0.001). In both cases, delays were significantly underestimated in SVIG-TB data. There was no significant difference between Patient-related delays determined from these two sources (p = 0.654).
Comparison with national SVIG-TB survey resultsIn a recent paper, diagnosis delay data from national SVIG-TB reports covering 2010 to 2014 was obtained and analysed.8 In this study, approximately 44.6% of cases had missing data regarding patient and/or healthcare delay (15.8% and 10.5% respectively; 18.2% had both missing) and were more likely to have a drug addiction, to be in prison or to be homeless. The number of cases with data missing on total diagnosis delay was not reported. Patient delay, healthcare delay, and Total Treatment delay medians were 33, 17, and 68 days respectively, in this population sample.
The proportion of cases with any missing data regarding diagnosis delay was greater in the Matosinhos local SVIG-TB data (57.2%), impacted particularly by data missing regarding patient-related delay (40.8%).
Compared to the national study results, median Total and Healthcare-related delays were generally greater in Matosinhos Municipality, regardless of the data source (SVIG-TB or Patient Record Review). The patient-related delay was, conversely, shorter (Table 1).
Significant delay differences were identified between National and this Municipality's SVIG-TB reports in Total (p = 0.008) and Healthcare-related (p < 0.001) delays but not for Patient-related delay (p = 0.078) (Table A.3).
On the other hand, there were significant differences between National SVIG-TB reports and Municipal Patient Record Review data: higher local Total (p < 0.001) and Healthcare-related median delays (p < 0.001) and lower Patient-related (p = 0.013) delay. (Table A.3).
DiscussionSVIG-TB forms are mainly used to obtain feedback on the follow-up and evolution of TB cases. They may also be used as a source of other complementary data such as TB diagnosis delay.
Regular assessment and audit of national registries is recommended by the WHO to identify and minimize some of its drawbacks: missing data, record errors, and reporting bias. Thorough record scrutiny through patient record review is an accessible and readily available, yet time-consuming means of assessing and minimizing the latter.
Cross-checking SVIG-TB delay data from this particular Municipality with Patient Record Review data hints of the existence of several limitations in SVIG-TB forms as a source of this information and provides clues to the possible presence of patient and healthcare-worker errors and biases in reporting and recording the former, namely:
- -
a significantly larger proportion of missing data in SVIG-TB forms;
- -
a small percentage of identifiable registering errors (presenting mainly as “negative” delay values);
- -
a significantly greater number of missing values in SVIG-TB forms filled by General Practitioners and those referring to younger patients;
- -
a possible tendency to significantly underestimate healthcare-related and total diagnosis delay;
This study has the limitation of analysing only one Municipality with certain specificities: a relatively high incidence TB rate when compared to national values (21.66 vs 16.6 cases/100 000 people)11,12; local healthcare structures which promote integration and close cooperation between primary and secondary care in a slightly different setting to the Portuguese NHS in general; an apparently greater proportion of missing data in local SVIG-TB record, when compared to a recent National SVIG-TB delay data review (57.2 vs 40.8%).
The impact of these specificities on the results obtained is unknown and may hamper the generalization of its conclusions to the national level. Nevertheless, this Municipality and its local healthcare units are a part of the NHS and are ruled by the same policies and regulations, including TB diagnosis and treatment guidelines, rendering these results potentially relevant.
Moreover, heterogeneity within healthcare structures and teams responsible for data registry is expected in different geographical, socio-economic and cultural settings worldwide.
Regardless of these shortcomings, missing data in more than 40% of reported cases, compounded with the possibility of reporting bias, is bound to negatively impact the accuracy and interpretation of SVIG-TB data as well as policy choices based on the former.
These results suggest that preventive measures such as encouraging the accurate filling in of SVIG-TB forms and regularly training TB Healthcare-providers on concepts such as symptom detection, healthcare observation and diagnosis dates as well as organizing regular random SVIG-TB record audits may aid in the evaluation and improvement of the reliability of this source locally and, consequently, nationally.
The significantly greater median (total and healthcare-related) diagnosis delay identified in Matosinhos Municipality may contribute to the greater local incidence of TB. However, a causal relation cannot be asserted. Furthermore, the different time-frames analysed, the significant amount of missing data, and the absence of an evaluation of registering errors and data review in the national SVIG-TB study do not allow for reliable conclusions on its meaning.
For further clarification, random blind SVIG-TB records audits and analysis of the correlation between local SVIG-TB reported diagnosis delay and TB incidence rates on a national scale could provide an evidenced-based ruling on these hypotheses. The results of this research could establish a strong foundation for:
- -
assessing SVIG-TB's use as a reliable source of data for policymaking with respect to diagnosis delay;
- -
objectively identifying some of the main SVIG-TB reporting issues regarding the latter;
- -
addressing strategies to minimize these issues and improve data records hereafter;
- -
estimating the objective impact of TB diagnosis delay in impairing TB control and elimination in Portugal;
Excessive delay in TB diagnosis may undermine the control and elimination of this disease in the short and long-term. An accurate determination and analysis of delay times may help identify where and how to improve and hasten TB diagnosis according to local needs.
To the best of our knowledge, this is the first study analysing the Portuguese TB Surveillance System's accuracy concerning date registry and, consequently, diagnosis delay reporting by quantitative and qualitative comparison of SVIG-TB registered information and extensive Patient Record Review.
Concerning date records (and indirectly delay time determination), this study identified a few registering errors, a significantly greater percentage of missing data, and a significant underestimation of healthcare-related and total TB diagnosis delay in SVIG-TB records when compared to Patient Record Review. These results provide a basis for further reflection on the shortcomings and potential of SVIG-TB in guiding the national TB program.
SVIG-TB has been a crucial tool in guiding National Public Health policies on the path towards TB elimination. However, there is still room for improvement using tools such as regular auditing and training of healthcare staff involved in national surveillance registry. An increase in the reliability of SVIG-TB could prove to be useful on the path towards enhanced understanding and control of the TB epidemic nationwide.
According to the Portuguese National Health System guidelines
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declarations of interest: None.


