

Maintaining exercise tolerance in individuals with cystic fibrosis (CF) is essential to limit the impact of the disease and increase survival.1 The cardio-respiratory responses to exercise provide an indication of exercise tolerance, which can be used to prevent unwanted effects during exercise.2 The 6-minute walk test (6MWT) is the gold standard field test for the evaluation of exercise capacity, however this test requires space and cannot always be performed.3 The one-minute sit-to-stand test (STST1’) can be performed in any setting and has recently been proposed as a reliable alternative for the measurement of exercise capacity in patients with CF.4,5 The measurement of the heart rate (HR) response during the STST1’ is valid and reliable in healthy children, but has not yet been validated in children with CF.6 The aim of this study was to assess the validity and reliability of the measurement of cardiorespiratory responses (HR, respiratory rate (RR) and pulsed oxygen saturation (SpO2)) during the STST1’ in children with CF.
This study is a secondary analysis of a previously published multicentre randomised cross-over trial (NCT03069625) and was approved by the Comité de Protection des Personnes Nord-Ouest III.4 Children with CF, aged from 6 to 18 years who had been clinically stable for 4 weeks were recruited from 3 French CF centres.
Participants performed two rounds of the STST1’ and 6MWT on the same day, with a 30 min minimum delay between each test, in a randomised order (computerised 1:1 block randomisation).4 The HR response (initial and final HR, and percentage ΔHR: ((HRf-HRi)/HRi) x100), RR response and SpO2 response (using the same indicators) were calculated for both the STST1’ and 6MWT; data from the best performance of each test were used. Concurrent validity of the HR, RR and SpO2 responses was evaluated by correlation analysis with the same responses during the 6MWT: 0–0.19 = very weak, 0.20–0.39 = weak, 0.40–0.59 = moderate, 0.60–0.79 = strong and 0.80–1.0 = very strong. Intra-rater reliability was evaluated using intra-class correlation coefficients (ICC): <0.5 = poor, 0.5–0.75 = moderate, 0.75–0.90 = good, >0.90 = very good. Test-retest reliability was evaluated by calculation of the mean bias using the Bland-Altman method (pre-post comparisons [learning effect verification]). Statistical analyses were performed with Graph Pad Prism 8®, and the significance level was set at p < 0.05.
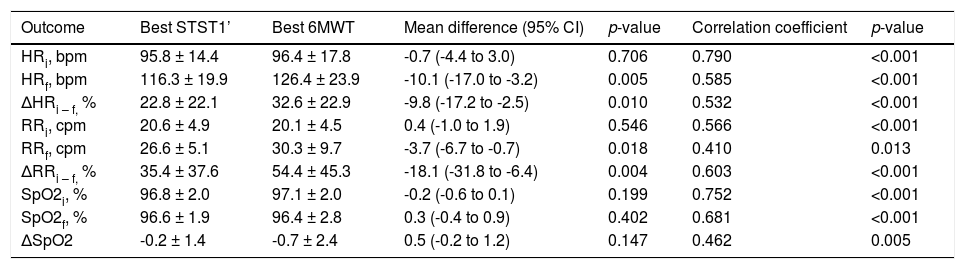
Thirty-six children participated. Mean age was 12.0 ± 3.5 years, and mean FEV1 was 95.8 ± 25.0%. The complete characteristics of the study sample have previously been described.4 Performances during both tests were moderately correlated (r = 0.480; p < 0.01). HR, RR and SpO2 measured before both tests were moderately to strongly correlated (r = 0.566–0.790). Correlations between responses during the STST1’ and 6MWT were moderate to strong and are detailed in the Table 1. The 6MWT elicited a higher cardio-respiratory response (HR and RR) than the STST1’ in 26 out of 36 (72%) of the children.
Concurrent validity of cardio-respiratory responses measured during the STST1’ and 6MWT in children with CF.
Data are shown as mean ± SD. Bpm: beats per minute; CI: confidence interval; Cpm: cycles per minute; HRi: initial heart rate; HRf: final heart rate; ΔHRi-f: delta heart rate; RRi: initial respiratory rate; RRf: final respiratory rate; ΔRRi-f: delta respiratory rate; SpO2i: initial pulsed oxygen saturation; SpO2f: final pulsed oxygen saturation; ΔSpO2: delta pulsed oxygen saturation; STST1’: sit-to-stand test; 6MWT: 6-minute walking test
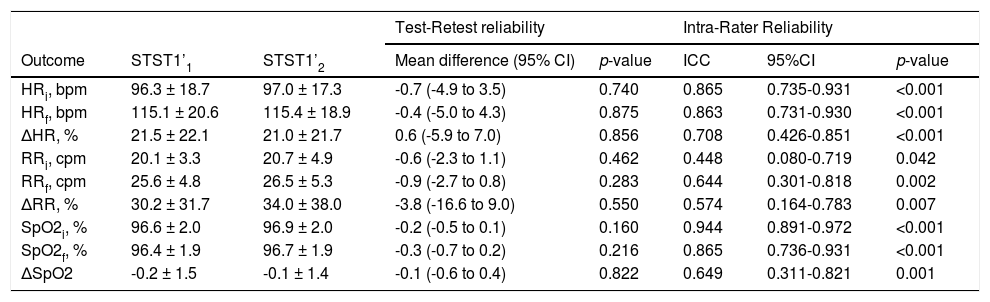
The intra-rater reliability of the STST1’ for the measurement of cardio-respiratory responses during exercise was moderate to very good (ICC>0.5). Evaluation of test-retest reliability showed there was no learning effect (Table 2). Mean bias was 0.6% and the limits of agreement were -36.6% to 37.8% (lower and upper bound) for the HR response; 3.8% (mean bias) and -70.4% to 78.0% (lower and upper bound) for the RR response; and -0.1% (mean bias) and -2.9% to 2.8 (lower and upper bound) for the SpO2 response.
Test-retest and intra-rater reliability of cardio-respiratory responses measured during the STST1’ in children with CF.
Data are shown as mean ± SD. Bpm: beats per minute; CI: confidence interval; Cpm: cycles per minute; HRi: initial heart rate; HRf: final heart rate; ΔHR: delta heart rate; RRi: initial respiratory rate; RRf: final respiratory rate; ΔRR: delta respiratory rate; SpO2i: initial pulsed oxygen saturation; SpO2f: final pulsed oxygen saturation; ΔSpO2: delta pulsed oxygen saturation; STST1’: sit-to-stand test
The results of this study demonstrated the concurrent validity and reliability of cardio-respiratory responses measured during the STST1’ in children with CF, despite large variability. Concurrent validity during exercise testing was moderate to strong, and intra-rater reliability was moderate to very good. Evaluation of test-retest reliability showed there was no learning effect. The values of the correlation coefficients suggest that the STST1’ should be used with caution as a surrogate to the 6MWT but could be relevant when the latter cannot be performed. This is supported by the results of Reychler et al. who found a similar level of concurrent validity for the HR response during the STST1’ (r = 0.522) in healthy children.6
However, in contrast with the results of Reychler et al.,6 in the present study peak HR and RR were higher during the 6MWT than the STST1’. However, peak HRs at the end of the tests in that study were much higher than in the present study (∼140 beats min versus 126 and 116 beats min for the 6MWT and STST1’ respectively). A possible explanation for this difference is that healthy children have a different intrinsic motivation or perception of exercise testing procedures than children with CF.
To conclude, the measurement of cardio-respiratory responses during the STST1’ is reliable and presents a moderate concurrent validity in children and adolescents with CF. The STST1’ could therefore be relevant when the 6MWT cannot be performed.
Funding supportThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors would like to thank the teams of Le Havre, Caen and Rouen Cystic Fibrosis Centres and the GHAHR Association (Le Havre, France) for their support. Authors would also like to thank Johanna Robertson for language assistance and constructive criticism.
Clinical Trial Registration: NCT03069625


