

End-of-life (EoL) care is a major component in the management of patients with advanced COPD. Patient-physician communication is essential in this process.
AimTo evaluate the practice of Portuguese Pulmonologists in EoL communication and palliative care in COPD.
MethodsAn on-line survey was sent to physicians affiliated to the Portuguese Pneumology Society.
ResultsWe obtained 136 answers from 464 eligible participants (29.3%). About half of the physicians reported that they have rarely introduced EoL discussions with their COPD patients (48.5%). Most had never/rarely suggested decision-making on the use of invasive mechanical ventilation (68.4%). Discussions were described as occurring mostly during/after a major exacerbation (53.7%). Only 37.5% of participants reported treating dyspnoea with opioids frequently/always. Only 9.6% stated that they never/rarely treated anxiety/depression. Most participants perceive the discussion of EoL issues as being difficult/very difficult (89.0%). The reasons most frequently given were feeling that patients were not prepared for this discussion (70.0%), fear of taking away a patient's hope (58.0%) and lack of training (51.0%).
ConclusionPatient and medical staff EoL communication in COPD is still not good enough. Training in this area and the creation of formal protocols to initiate EoL have been identified as major factors for improvement.
Os cuidados terminais (EoL) são um componente importante do tratamento de doentes com doença pulmonar obstrutiva crónica (DPOC) avançada. A comunicação entre o doente e o médico é fundamental neste processo.
ObjetivoAvaliar a prática dos pneumologistas portugueses na comunicação sobre o fim de vida e os cuidados paliativos na DPOC.
MétodosFoi enviado um inquérito online para os médicos sócios da Sociedade Portuguesa de Pneumologia.
ResultadosRecebemos 136 respostas dos 464 participantes elegíveis (29,3%). Cerca de metade dos médicos indicaram que raramente iniciaram conversas sobre o fim de vida com os seus doentes com DPOC (48,5%). A maioria nunca/raramente sugeriram a toma de decisão sobre a utilização de ventilação mecânica invasiva (68,4%). As conversas foram descritas como ocorrendo, na sua maioria, durante/após uma exacerbação grave (53,7%). Apenas 37,5% dos participantes indicaram tratar a dispneia frequentemente/sempre com opiáceos. Apenas 9,6% indicaram que nunca/raramente trataram a ansiedade/depressão. A maioria dos participantes considerou a conversa sobre questões de fim de vida como sendo difícil/muito difícil (89,0%). Os motivos mais frequentemente indicados foram a sensação de que os doentes não estavam preparados para essa conversa (70,0%), medo de tirar a esperança aos doentes (58,0%) e falta de formação (51,0%).
ConclusãoA comunicação sobre o fim de vida entre o doente e os médicos na DPOC ainda não é suficientemente boa. A formação nesta área e a criação de protocolos formais para iniciar os cuidados em fim de vida foram identificados como fatores importantes a melhorar.
Chronic obstructive pulmonary disease (COPD) is a chronic and progressive disease that in its advanced stages may be associated with important physical, psychological and social impairments. Palliative care should be provided to advanced COPD patients so as to reduce the high burden of chronically debilitating symptoms such as dyspnoea and anxiety.
Patient–physician communication on prognosis, preferences for life-sustaining treatments and palliative care, is essential to ensure that COPD patients receive end-of-life (EoL) quality care that is consistent with the values upheld. The uncertain disease trajectory, which frequently involves unexpected deterioration in health status, makes planning of care in advance essential.1
In recent years, there has been a growing interest in EoL care in advanced COPD. Some important scientific societies have published recommendations on this theme and the Global Initiative for Obstructive Pulmonary Disease (GOLD) introduced it for the first time into the 2013 updated revision.2–4 The challenge remains in how EoL care is implemented in practice. At present, there is evidence that COPD patients receive poor EoL care and that there is insufficient patient-physician discussion on EoL preferences.5,6
We developed a survey to characterize the Portuguese Pulmonologists’ practice in EoL communication and palliative care in advanced COPD patients, and identify hurdles to its consistent implementation. With this study, we hope to help establish strategies to overcome the difficulties that physicians face in their every-day practice, which ultimately may lead to an improvement on the EoL care that COPD patients receive.
MethodsParticipant recruitmentIn January 2013 we asked the Portuguese Pneumology Society (SPP) to provide us with the mailing list of all affiliated Respiratory Medicine specialists and fellows with email contact. We obtained a list of 464 members. We only asked physicians who had had clinical activity in the previous year to answer the survey.
Questionnaire development and administrationA self-administrated questionnaire was developed specifically for this study. The authors generated questions based on a review of the literature. Questions were drawn up to address four main themes: (1) palliation of symptoms; (2) frequency and topics of EoL communication; (3) timing and interveners of EoL communication; (4) obstacles to EoL communication.
The following data were collected to characterize participants: age, gender, religious beliefs, years of practice, type of institution, region of the country and number of patients with COPD treated per year.
At the beginning of the questionnaire, participants were asked to answer questions with reference to the patients they had treated in the previous year, who had two or more of the following characteristics: forced expiratory volume in first second (FEV1) under 30%, oxygen dependence, one or more hospital admissions in the previous year for an acute exacerbation of COPD, left heart failure or other comorbidities, weight loss or caquexia, decreased functional status, increasing dependence on others and were over 70 years old. We adopted these criterion from Curtis, whose purpose was to identify patients in whom a discussion on preferences about EoL care should be initiated.5
We pretested the questionnaire on a convenience sample of 6 pulmonologists to ensure clarity and comprehensiveness. A web platform was then designed to facilitate survey completion and data collection. Participants received an invitation to answer the questionnaire via an e-mail sent by the SPP, containing a link to the online platform. One month was allowed for questionnaire completion. During the one month period two e-mails of reminder were sent to each applicant, after which time the website was closed. All complete questionnaires were considered eligible so that we are characterizing the reality of our practice.
Statistical analysisDemographic data and the several variables related to palliation and communication were analyzed using descriptive statistics. To verify a possible influence of the participant characteristics on their ability to undertake EoL communication, a univariate analysis was performed between the main characteristics – years of practice, type of institution (university hospital vs other), number of COPD patients treated – and two questions evaluated by a semi-quantitative scale: (a) “How often have you started a EoL discussion on your initiative?”; (b) “How difficult is it for you to discuss EoL issues with your patients?”. Statistical significance values were set at p≤0.05.
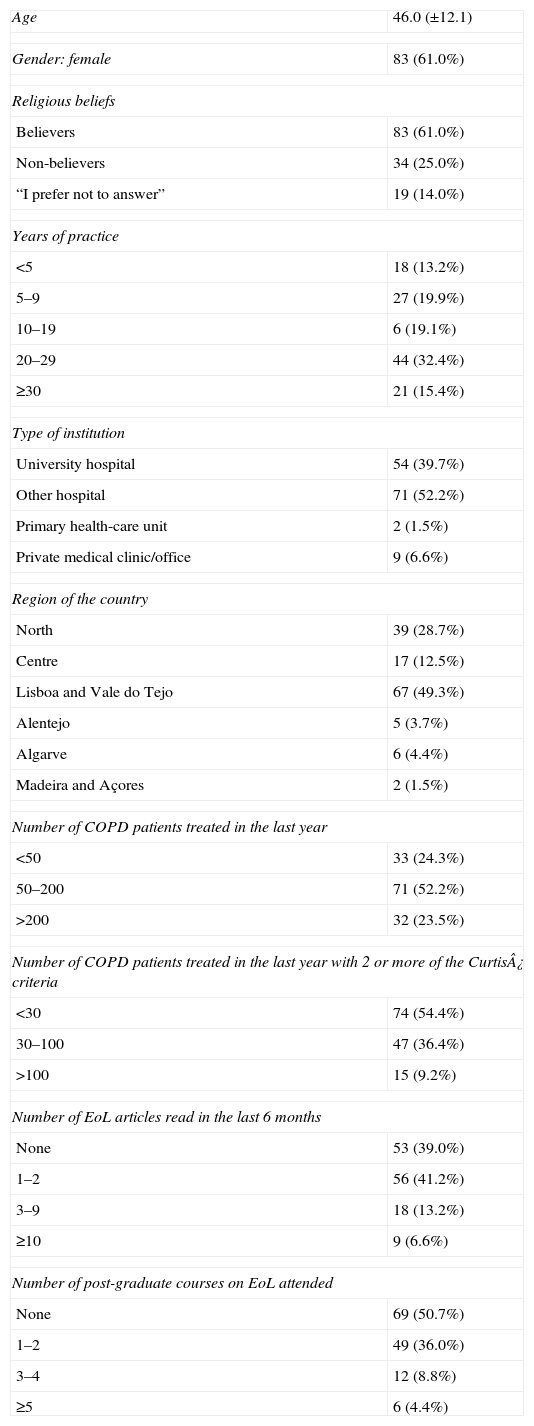
ResultsFrom the 464 eligible participants, 136 completed the questionnaire (participation rate of 29.3%). Characteristics of respondents are summarized in Table 1. Most respondents (52.2%) had treated 50–200 COPD patients in the previous year.
Participant characteristics.
| Age | 46.0 (±12.1) |
| Gender: female | 83 (61.0%) |
| Religious beliefs | |
| Believers | 83 (61.0%) |
| Non-believers | 34 (25.0%) |
| “I prefer not to answer” | 19 (14.0%) |
| Years of practice | |
| <5 | 18 (13.2%) |
| 5–9 | 27 (19.9%) |
| 10–19 | 6 (19.1%) |
| 20–29 | 44 (32.4%) |
| ≥30 | 21 (15.4%) |
| Type of institution | |
| University hospital | 54 (39.7%) |
| Other hospital | 71 (52.2%) |
| Primary health-care unit | 2 (1.5%) |
| Private medical clinic/office | 9 (6.6%) |
| Region of the country | |
| North | 39 (28.7%) |
| Centre | 17 (12.5%) |
| Lisboa and Vale do Tejo | 67 (49.3%) |
| Alentejo | 5 (3.7%) |
| Algarve | 6 (4.4%) |
| Madeira and Açores | 2 (1.5%) |
| Number of COPD patients treated in the last year | |
| <50 | 33 (24.3%) |
| 50–200 | 71 (52.2%) |
| >200 | 32 (23.5%) |
| Number of COPD patients treated in the last year with 2 or more of the Curtis¿ criteria | |
| <30 | 74 (54.4%) |
| 30–100 | 47 (36.4%) |
| >100 | 15 (9.2%) |
| Number of EoL articles read in the last 6 months | |
| None | 53 (39.0%) |
| 1–2 | 56 (41.2%) |
| 3–9 | 18 (13.2%) |
| ≥10 | 9 (6.6%) |
| Number of post-graduate courses on EoL attended | |
| None | 69 (50.7%) |
| 1–2 | 49 (36.0%) |
| 3–4 | 12 (8.8%) |
| ≥5 | 6 (4.4%) |
Data are presented as n (%) or mean (±standard deviation); EoL=end-of-life; COPD=chronic obstructive pulmonary disease.
We questioned physicians about the number of patients that would not cause them surprise if they died in the following year. Seventy-one (52.1%) would not be surprised if up to 30% of their patients died in the following year, 56 (41.1%) admitted that 30–69% could die in that period, and only 9 (6.8%) considered this possibility in 70% or more patients.
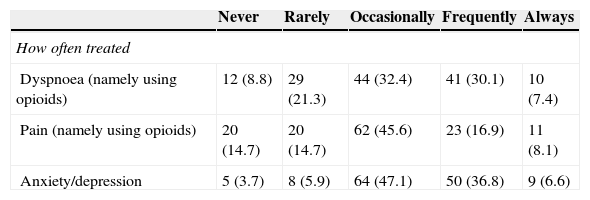
Concerning palliation, we asked physicians how often they treated pain, dyspnoea (namely with opioids) and depression/anxiety. Results are summarized in Table 2. The use of opioids to manage dyspnoea was reported to occur occasionally in 32.4% of cases and frequently/always in 37.5%. Respondents indicated they treated anxiety and depression frequently/always in 43.4% of cases.
Palliation of symptoms.
| Never | Rarely | Occasionally | Frequently | Always | |
|---|---|---|---|---|---|
| How often treated | |||||
| Dyspnoea (namely using opioids) | 12 (8.8) | 29 (21.3) | 44 (32.4) | 41 (30.1) | 10 (7.4) |
| Pain (namely using opioids) | 20 (14.7) | 20 (14.7) | 62 (45.6) | 23 (16.9) | 11 (8.1) |
| Anxiety/depression | 5 (3.7) | 8 (5.9) | 64 (47.1) | 50 (36.8) | 9 (6.6) |
Data are presented as n (%).
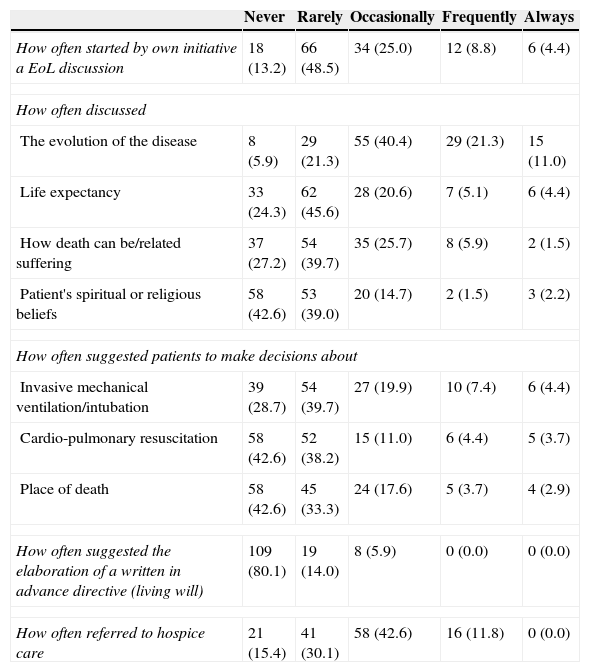
The frequency of EoL communication and the topics are presented in Table 3. Most physicians (61.7%) said they had rarely or never initiated this type of discussion. The progression of disease was the topic most discussed by physicians with patients, but life expectancy and the suffering related to death were less often approached. Most respondents also claimed to have never or rarely asked about patients’ spiritual or religious beliefs (81.6%).
Frequency and topics of EoL communication.
| Never | Rarely | Occasionally | Frequently | Always | |
|---|---|---|---|---|---|
| How often started by own initiative a EoL discussion | 18 (13.2) | 66 (48.5) | 34 (25.0) | 12 (8.8) | 6 (4.4) |
| How often discussed | |||||
| The evolution of the disease | 8 (5.9) | 29 (21.3) | 55 (40.4) | 29 (21.3) | 15 (11.0) |
| Life expectancy | 33 (24.3) | 62 (45.6) | 28 (20.6) | 7 (5.1) | 6 (4.4) |
| How death can be/related suffering | 37 (27.2) | 54 (39.7) | 35 (25.7) | 8 (5.9) | 2 (1.5) |
| Patient's spiritual or religious beliefs | 58 (42.6) | 53 (39.0) | 20 (14.7) | 2 (1.5) | 3 (2.2) |
| How often suggested patients to make decisions about | |||||
| Invasive mechanical ventilation/intubation | 39 (28.7) | 54 (39.7) | 27 (19.9) | 10 (7.4) | 6 (4.4) |
| Cardio-pulmonary resuscitation | 58 (42.6) | 52 (38.2) | 15 (11.0) | 6 (4.4) | 5 (3.7) |
| Place of death | 58 (42.6) | 45 (33.3) | 24 (17.6) | 5 (3.7) | 4 (2.9) |
| How often suggested the elaboration of a written in advance directive (living will) | 109 (80.1) | 19 (14.0) | 8 (5.9) | 0 (0.0) | 0 (0.0) |
| How often referred to hospice care | 21 (15.4) | 41 (30.1) | 58 (42.6) | 16 (11.8) | 0 (0.0) |
Data are presented as n (%); EoL=end-of-life.
Regarding EoL decision-making, the majority of participants said they never/rarely suggested their patients to make decisions about invasive mechanical ventilation/intubation (68.4%), cardio-pulmonary resuscitation (80.8%) or whether they preferred to die at home versus in hospital (75.9%). Most had never suggested the drawing up a written advance directive (80.1%), although almost all of them (95.6%) were aware that the Portuguese law provides for this possibility. Only 11.8% reported to have frequently referred COPD patients to hospice care services.
We also inquired of participants what moment was usually chosen for EoL discussion. Discussion was reported to occur during a major exacerbation in 29.4%, in advanced disease when the patient is stable in 25.0%, after the patient survives a major exacerbation in 24.3%, only if patient or caregiver introduces the subject in 14.0% and early after diagnosis in 7.4%.
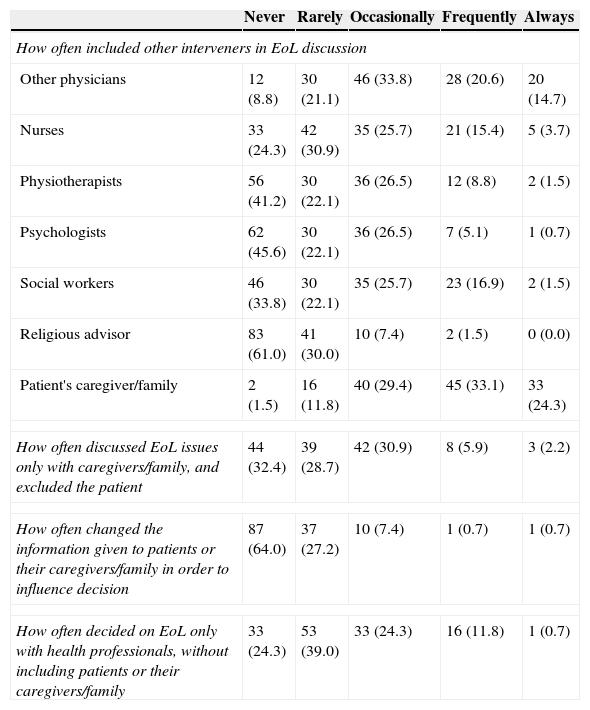
Interveners usually included in EoL discussion are listed in Table 4. Among healthcare professionals, other physicians were the main interveners, followed by nurses. Most (91.0%) respondents indicated that they never or rarely include religious advisors. About half (57.4%) claimed to frequently/always include relatives.
Interveners in EoL communication.
| Never | Rarely | Occasionally | Frequently | Always | |
|---|---|---|---|---|---|
| How often included other interveners in EoL discussion | |||||
| Other physicians | 12 (8.8) | 30 (21.1) | 46 (33.8) | 28 (20.6) | 20 (14.7) |
| Nurses | 33 (24.3) | 42 (30.9) | 35 (25.7) | 21 (15.4) | 5 (3.7) |
| Physiotherapists | 56 (41.2) | 30 (22.1) | 36 (26.5) | 12 (8.8) | 2 (1.5) |
| Psychologists | 62 (45.6) | 30 (22.1) | 36 (26.5) | 7 (5.1) | 1 (0.7) |
| Social workers | 46 (33.8) | 30 (22.1) | 35 (25.7) | 23 (16.9) | 2 (1.5) |
| Religious advisor | 83 (61.0) | 41 (30.0) | 10 (7.4) | 2 (1.5) | 0 (0.0) |
| Patient's caregiver/family | 2 (1.5) | 16 (11.8) | 40 (29.4) | 45 (33.1) | 33 (24.3) |
| How often discussed EoL issues only with caregivers/family, and excluded the patient | 44 (32.4) | 39 (28.7) | 42 (30.9) | 8 (5.9) | 3 (2.2) |
| How often changed the information given to patients or their caregivers/family in order to influence decision | 87 (64.0) | 37 (27.2) | 10 (7.4) | 1 (0.7) | 1 (0.7) |
| How often decided on EoL only with health professionals, without including patients or their caregivers/family | 33 (24.3) | 53 (39.0) | 33 (24.3) | 16 (11.8) | 1 (0.7) |
Data are presented as n (%); EoL=end-of-life.
When asked how often they excluded the patient and discussed EoL only with caregivers, most (61.1%) claimed to have never/rarely done so. Also, 63.3% indicated they never/rarely made EoL decisions just with health providers. Most (64.0%) claimed to have never changed the information given to patients/caregivers in order to influence decision according to what they believe is best, and from the remaining, most said they only did this rarely (27.2%).
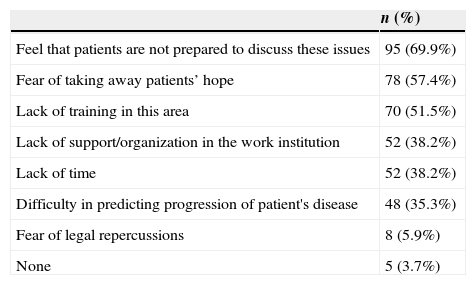
We questioned closely as to how difficult it was for physicians to hold EoL discussions with their patients. Twenty-seven answered it was very difficult (19.9%), 94 said it was difficult (69.1%), 4 were indifferent (2.9%), 8 said it was easy (5.9%) and 3 very easy (2.2%). From a 7-item list, we asked them to select all the difficulties usually felt in EoL discussions. Results are summarized in Table 5.
Obstacles to EoL communication.
| n (%) | |
|---|---|
| Feel that patients are not prepared to discuss these issues | 95 (69.9%) |
| Fear of taking away patients’ hope | 78 (57.4%) |
| Lack of training in this area | 70 (51.5%) |
| Lack of support/organization in the work institution | 52 (38.2%) |
| Lack of time | 52 (38.2%) |
| Difficulty in predicting progression of patient's disease | 48 (35.3%) |
| Fear of legal repercussions | 8 (5.9%) |
| None | 5 (3.7%) |
Data are presented as n (%); EoL=end-of-life.
We inquired about the participants’ opinion on the importance of discussing EoL with advanced COPD patients. Most (76.5%) rated it as very important, 31 (22.8%) as a subject of some importance, with only one participant indicating that it was of little importance. Finally, we asked if participants would like this subject to be further discussed in scientific meetings. Almost all (98.5%) agreed, and only 2 (1.5%) respondents claimed that the issue is being sufficiently addressed already.
There were no statistical significant differences between years of practice, type of institution or number of COPD patients treated and the main outcomes.
DiscussionDespite the increasing interest on EoL communication and palliative care in end-stage COPD, this is, to our knowledge, the first study performed in Portugal to evaluate Pulmonologists¿ perception of this matter.
Palliation of symptomsAlthough the majority of physicians reported that they treated symptoms at least occasionally, our findings suggest that symptom management may not be optimized. Only a few reported using opioids routinely in the treatment of dyspnoea and pain. Since opioids are the only drug proven to be effective in controlling dyspnoea in these patients, these results are clearly unsatisfactory.7 Previous studies have shown evidence of poor palliation in COPD.8–10 The study SUPPORT, for instance, revealed that dyspnoea occurs more often in these patients than in lung cancer patients. In the same study, 21% of patients with COPD reported suffering from severe pain.10 There is a strong possibility that analgesics are withheld in COPD because of concerns about adverse effects, in particular respiratory depression. This fear is unfounded, since there is no evidence to date that the doses of opioids used to treat breathlessness causes clinically detectable respiratory depression or increases mortality.7
It has been suggested that anxiety/depression affects as many as 90% of advanced COPD patients, but previous studies have reported that only 4–31% were receiving pharmacological treatment.11,12 We found a better performance, which may reveal a rising awareness of the beneficial effects of antidepressants in improving mood and decreasing dyspnoea in COPD patients.13 Treating depression is essential since it may modify patient decisions concerning EoL care.14
Frequency and topics of end-of-life communicationAnother important outcome of this study was to realize that more than half of Portuguese Pulmonologists never or rarely introduce EoL discussions with their patients. Previous reports, both from physician and patient point of view, have also shown insufficient EoL communication.15–17 One of the topics most neglected by physicians was spiritual/religious beliefs, although there is evidence that the majority of patients want to discuss these issues.18
Although advance care planning seems to increase patient satisfaction and reduce emotional distress, our results show that physicians have used little initiative in introducing it.18 The lack of certainty on prognosis strengthens the need for advance directives in COPD, but the evidence is they are rarely used. A Survey carried out in the European Respiratory Intermediate care units showed that only 30% of patients admitted to having had a formal discussion about EoL decisions and/or signed a living will.19 As a result, COPD patients are more likely to die with aggressive, technological care directed at preservation of life and less likely to receive palliative care, despite having preferences favouring palliation.10 In fact, the majority of COPD patients die in the hospital, mostly in intensive care units, although at least half of clinically stable advanced COPD patients would prefer to die in their home environment.8,20
Hospice care in end-stage COPD is another emerging issue. The recent revised version of GOLD recommends that clinicians should identify COPD patients who could benefit from palliative care services and help find available resources within their community.4 In our study, about half the respondents indicated they occasionally/frequently refer patients to hospice care. Nonetheless, patients dying of end-stage COPD are in general less likely to be offered hospice services compared to patients with lung cancer.5 Uncertainty about prognosis as well as doubts as to whether a traditional hospice model is suitable for patients with COPD, may explain this difference, although it should not impede access to hospice care.2
Timing and interveners in end-of-life communicationRecent consensus recommends that EoL care should be available early during the course of the disease, from when the patient becomes symptomatic.3 However, contrary to this, we found that most physicians discuss it during/after a major exacerbation. Another study also reported that discussions occur mainly in advanced stages of COPD, that is when dyspnoea became severe.21
There are more growing recommendations on the use of interdisciplinary health-care teams to ensure quality EoL care.2 Nonetheless, we found poor interdisciplinary work in our study. Results were similar in the previously mentioned European survey, which found that nurses were involved in 55.9%, but only in a small minority of cases were opinions sought from other professionals. In the same study, patient's relatives were involved in discussion in only about half the cases.19 We in turn, found a better performance in terms of engaging the family, although often without patient participation. Interestingly, our participants rarely reported modifying the information provided in order to influence decisions, a phenomenon that was reported to commonly occur in previous studies.21,22
Obstacles in end-of-life communicationMost participants described the discussion of EoL issues as being difficult or very difficult, which makes it essential to understand what the barriers are that physicians face, especially the ones that can be modified.
As in a previous study, the feeling that patients may be unprepared to discuss these matters and the fear of taking away their hope, were pointed out as major obstacles to communication.17 Patient failure to understand COPD as a life-threatening disease and their will to concentrate on staying alive play an important role in this process.17 Cultural differences possibly have an influence as well. In a European survey evaluating public preferences for self-involvement in EoL decision-making, about 60% of the Portuguese participants wanted to be involved, which was less than the European mean (74%).23 These barriers may be overcome with education about illness progression and encouragement to communicate.
Other obstacles mentioned by our respondents have to do with organizational aspects, namely lack of time, lack of training and absence of protocols. The lack of formal protocols to initiate EoL was also pointed out by Partridge et al.24 Additionally, educational practices are inadequate, as revealed in a survey performed in the United States.25 These aspects represent important targets for intervention. Each institution should develop policies to guide health staff in initiating the kind of EoL care that is feasible in their context.2 Scientific societies, in their turn, are responsible for ensuring that there is appropriate education on EoL care in medical schools and for promoting continuous education among attendant health-care givers. There is evidence that educational programmes and even smaller interventions result in measurable improvements in communication skills.26–28 Moreover, our study demonstrates that Pulmonologists are interested in further education on this subject.
Limited resources are a significant impediment to effective EoL care. In Portugal, the need for fiscal consolidation has led to major cuts in the financing of the health sector in recent years.29 Despite the National Program for Palliative Care which was created in 2010, numbers show that resources (regarding number of hospice care beds and the availability of domiciliary services) are still far behind recommendations by the European Association for Palliative care.29 These restrictions are recognized by Portuguese citizens, who call for more hospital palliative care units and more palliative care access.30 Evidence-based service development using existing resources may be part of the solution.6
According to our results, the particular characteristics of a physician do not seem to influence their ability to communicate on EoL issues, which suggests that the barriers identified are transversal to different practice settings.
Limitations and conclusionsThe present study has a number of potential limitations.
The Curtis criterion to identify candidates for EoL discussion may be subject to criticism. It is a presumptive criterion, since it has not been proven that patients who are included die sooner or have more symptoms. Other proposed criteria, namely the CART and BODE scores, both able to predict mortality in patients with COPD, would be equally valid.31–33 Nonetheless, we believe the former is more suitable for the purposes of this type of questionnaire, since it includes a list of clinical characteristics, which are easier to answer with a yes/no response, when mentally profiling the type of patients. Whereas CART is a tree-algorithm and BODE requires a numeric grading of each variable, both of which cases would make this process more difficult.
Concerning the use of opioids in the treatment of dyspnoea, we retrospectively realized that the question should have been put in a more objective way. Since current recommendations to treat dyspnoea include a multimodal approach, we recognize that the way the question was phrased may not reveal the true scale of opioids use for this purpose.
We recognize that our participation rate was low. However, our universe included an unknown number of retired physicians, who were asked not to answer the questionnaire, and thus underestimated the overall response rate. Also, the choosing to use a web platform to perform the survey, may have influenced the response rate and the profile of the respondents.
Another obvious limitation is that the self-reported information may not reflect what Pulmonologists actually do in practice. Future studies should find ways of quantifying EoL communication more objectively, while recognizing that research in this area is hampered by important ethical and methodological challenges.34
In conclusion, our study demonstrated that our palliative care and EoL communication are a long way from being from what they should be. Awareness, training in this field and the creation of formal protocols have been identified as major areas for improvement, and should be encouraged. Future studies should focus on developing and testing the effectiveness of practical strategies to improve EoL communication and palliative care in COPD.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank the Portuguese Society of Pulmonology for providing us the contacts of their affiliates and inviting them to participate in this survey.
This study was performed at: Serviço de Pneumologia do Centro Hospitalar Lisboa Norte, EPE - Hospital Pulido Valente, Lisbon, Portugal.


