


Chronic obstructive pulmonary disease (COPD) is a disease with great impact on the ability to carry out physical activity.
ObjectiveTo identify the main factors that affect physical activity in the daily life of patients with COPD.
MethodsPhysical activity in daily routine has been evaluated according to the London Chest Activity of Daily Living scale (LCADL) and the pedometer counting the number of steps per day, for a period of three days. Fifty-five male patients with a diagnosis of moderate to very severe COPD were included (aged 67±9.6 years; FEV1 50.8±14.7% predicted).
ResultsPatients walked on average 4972 steps per day. Very severe COPD patients (n=12) walked much less than severe (n=21) and moderate (n=22) patients (respectively 3079.8 versus 4853.5 and 6118.1 steps per day, p<0.001). The number of steps per day had a negative correlation with age, dyspnea (mMRC), depression, BODE index and pulmonary hyperinflation; and a positive correlation with the distance covered in the six-minute walk test (6MWT), forced expiratory volume in the first second (FEV1), carbon monoxide diffusion capacity (DLCO), arterial oxygen saturation (SpO2) and body mass index (BMI).
ConclusionsThe main factors that correlated with limited physical activity in daily life routine of this group of COPD patients were dyspnea and 6min walking distance. These patients form a sedentary group, with a low rate of daily physical activity, which is more evident in patients with GOLD spirometry stage IV. Although pedometer is simpler and less accurate than other devices, it can be used to detect significant restraints daily life physical activity of COPD patients.
A Doença Pulmonar Obstrutiva Crónica (DPOC) é uma doença com grande impacto na capacidade de realizar atividade física.
ObjetivoIdentificar os principais fatores que influenciam a atividade física na vida diária dos doentes com DPOC.
MétodosA atividade física na rotina diária foi avaliada de acordo com a escala London Chest Activity of Daily Living (LCADL) e a quantificação do número de passos por dia avaliada com pedómetro durante um período de 3 dias. Foram selecionados 55 doentes do sexo masculino com o diagnóstico de DPOC moderada a muito grave (com 67±9,6 anos de idade e volume expiratório forçado no primeiro segundo (FEV1) 50,8±14,7% do previsto).
ResultadosOs doentes andaram uma média de 4.972 passos por dia. Os doentes com DPOC muito grave (n=12) andaram muito menos do que os doentes com DPOC grave (n=21) e moderada (n=22) (respetivamente, 3.079,8 versus 4.853,5 e 6.118,1 passos por dia, p < 0,001). O número de passos por dia apresentou uma correlação negativa com a idade, dispneia (mMRC), depressão, índice BODE e hiperinsuflação pulmonar; e apresentou uma correlação positiva com a distância percorrida na prova de marcha de seis minutos (6MWT), FEV1, capacidade de difusão do monóxido de carbono (DLCO), saturação de oxigénio arterial (SpO2) e índice de massa corporal (IMC).
ConclusõesOs principais fatores que se correlacionaram com a limitação da atividade física na rotina da vida diária deste grupo de doentes com DPOC foram a dispneia e a distância percorrida na prova de marcha dos 6 minutos. Estes doentes formam um grupo sedentário, com uma taxa reduzida de atividade física diária, o que é mais evidente em doentes com espirometria de estádio GOLD IV. Embora o pedómetro seja mais simples e menos preciso que outros dispositivos, pode ser usado para detetar restrições significativas da atividade física na vida diária dos doentes com DPOC.
Monitoring of the daily physical activity in patients with COPD has been a subject of study, since physical activity is known to be reduced1,2 due to multifactorial causes and worsened prognosis.
The present recommendations3 point out the benefits of moderately intense daily physical activity for at least 30min 5times/week (or 150min/week) and considers those not meeting this goal as insufficiently active.
Physical activity in daily life can be measured with pedometers,4 which evaluate the vertical body movement, counting the number of steps during a certain period of time, during a recommended evaluation period of three days.5 Although less accurate than accelerometers, these devices provide a low-cost objective measurement of walking, a daily physical activity responsible for a great amount of the total energy expenditure.
Tudor-Locke and Bassett6 proposed the following indices of physical activity measured with a pedometer in adults: less than 5000 steps per day – “sedentary”; 5000–7499 steps per day – “low active”; 7500–10,000 steps per day – “somewhat active” and more than 10,000 steps per day – “active”.
The main goal of this study was to identify the factors that influence physical activity in the daily life in COPD patients. Secondary goals were: (1) to find out whether there were differences in physical activity according to airways flow limitation (GOLD spirometry grade7); (2) to compare the number of steps per day measured with the pedometer and daily living activities (reported by London Chest of Activity Daily Living scale) and (3) to relate clinical, nutritional, psychological, lung function and exercise variables with daily living activities of COPD patients.
MethodsSampleThis study included 55 moderate to very severe7 COPD patients, followed in the Pulmonology Unit and selected consecutively in a period of 7 months.
The inclusion criteria were: male sex; smoking history above 10 pack-years; COPD diagnosis; FEV1/FVC% ratio less than 70% and FEV1 less than 80% of predicted post-bronchodilation and stable disease (absence of exacerbation or change in treatment in the last three months). Exclusion criteria were other conditions that could also cause or enhance dyspnea (e.g. asthma, cardiovascular diseases), conditions that could impair physical activity performance (e.g. cerebrovascular, osteoarticular or psychiatric diseases) or already taking part in a pulmonary rehabilitation program.
The study was carried out at the Respiratory Physiopathology Laboratory, Centro Hospitalar de Torres Vedras, after being approved by the Centro Hospitalar de Torres Vedras Ethics Committee, and after obtaining written informed consent from the patients.
Characterization of the samplePatients were clinically evaluated, including their smoking habits and the modified Medical Research Council (mMRC) dyspnea scale quantification. mMRC is formed by 5 grades (0 to 4), the highest value corresponding to the greatest limitation caused by dyspnea in the activities of daily life.8
Anxiety and depression were investigated using the hospital anxiety and depression scale (HADS). This scale is composed of 14 items, 7 being related to anxiety and 7 to depression, with a maximum possible score of 21 for every quotation.9
The nutritional assessment was based on the body mass index (BMI) evaluation, defined as the weight in kilos divided by the height in squared meters. According to the adopted reference values,10 a BMI below 20kg/m2 was considered low weight, from 20 to 24.9kg/m2 normal weight, from 25 to 29.9kg/m2 overweight and obesity from 30kg/m2.
Pulmonary function tests at rest included spirometry with bronchodilation test, evaluation of pulmonary static volumes by plethysmography and carbon monoxide diffusion capacity by the single breath method (Sensor Medics, model AutoBox Vmax 22, Yorba Linda, CA, USA, for all lung tests) according to the standard methods.11,12,13
Two 6MWT were performed according to the standard methods14 with a minimum interval of 30min between them. The one with the longest distance covered was chosen. Arterial blood gases were assessed at the beginning and at the end of the 6MWT (Gas analyser Elnor Nova Biomedical Stat Profile pHOx Plus/c, Waltham, USA). Oxygen saturation by pulse oximetry and dyspnea by the modified Borg scale15 were also evaluated at rest, in the beginning and immediately after 6MWT.
At the end of these evaluations, the BODE index was calculated.16
Evaluation of physical activity in daily lifePhysical activity in daily life was evaluated according to LCADL scale and the number of steps per day, on three consecutive days, between Monday and Friday, was counted using the pedometer.
LCADL contains 15 activities of daily living (ADL) items, divided into four sections (self-care, domestic, physical and leisure), where the patients give to each item a score from 0 to 5, mentioning to what extent dyspnea interferes with these 15 activities. It is possible to get a total score of between 0 and 75. The higher the results on the scale the greater the limitation in ADL.17,18
After completing the scale, a pedometer Geonaute Dista T300 was given to each patient, who then placed it on their waistband when walking (pedometer had to be removed each time the patient takes a shower, lies in bed or in any other situation which might damage the gear), keeping to their daily routine for three days.
Statistical analysisData are expressed as mean±standard deviation (SD).
ANOVAs one-way test was used, followed by tests of multiple a posteriori comparisons of Tukey to assess the differences in physical activity in daily life according to flow limitation (GOLD spirometry grade).
We compared the number of steps per day measured with the pedometer and LCADL through the Spearman correlation coefficient. The number of steps per day was a dependent variable. The independent variable selection was achieved by Pearson's correlation coefficient analysis.
Finally, a stepwise multiple linear regression analysis was done, in order to estimate the influence of the variables on physical activity in the daily routine, according to the pedometer. The level of significance was set at p<0.05.
All analysis was done with SPSS v.16.0 software (Statistical Package for the Social Sciences) for Mac.
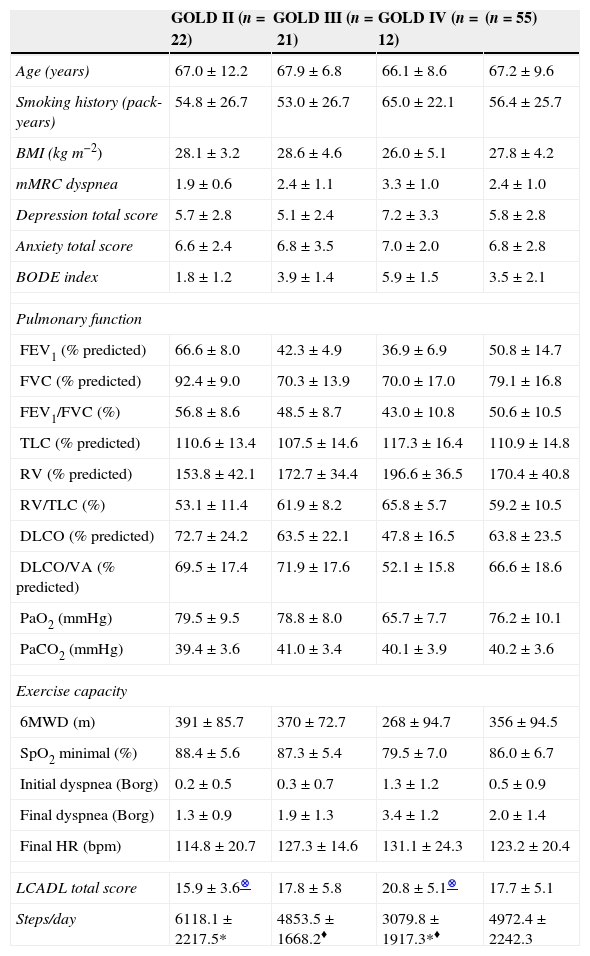
ResultsThe clinical, nutritional, psychological, lung function features as well as features of physical activity of the sample are shown in Table 1.
Clinical, nutritional, psychological, respiratory function and physical activity characterization.
| GOLD II (n=22) | GOLD III (n=21) | GOLD IV (n=12) | (n=55) | |
|---|---|---|---|---|
| Age (years) | 67.0±12.2 | 67.9±6.8 | 66.1±8.6 | 67.2±9.6 |
| Smoking history (pack-years) | 54.8±26.7 | 53.0±26.7 | 65.0±22.1 | 56.4±25.7 |
| BMI (kgm−2) | 28.1±3.2 | 28.6±4.6 | 26.0±5.1 | 27.8±4.2 |
| mMRC dyspnea | 1.9±0.6 | 2.4±1.1 | 3.3±1.0 | 2.4±1.0 |
| Depression total score | 5.7±2.8 | 5.1±2.4 | 7.2±3.3 | 5.8±2.8 |
| Anxiety total score | 6.6±2.4 | 6.8±3.5 | 7.0±2.0 | 6.8±2.8 |
| BODE index | 1.8±1.2 | 3.9±1.4 | 5.9±1.5 | 3.5±2.1 |
| Pulmonary function | ||||
| FEV1 (% predicted) | 66.6±8.0 | 42.3±4.9 | 36.9±6.9 | 50.8±14.7 |
| FVC (% predicted) | 92.4±9.0 | 70.3±13.9 | 70.0±17.0 | 79.1±16.8 |
| FEV1/FVC (%) | 56.8±8.6 | 48.5±8.7 | 43.0±10.8 | 50.6±10.5 |
| TLC (% predicted) | 110.6±13.4 | 107.5±14.6 | 117.3±16.4 | 110.9±14.8 |
| RV (% predicted) | 153.8±42.1 | 172.7±34.4 | 196.6±36.5 | 170.4±40.8 |
| RV/TLC (%) | 53.1±11.4 | 61.9±8.2 | 65.8±5.7 | 59.2±10.5 |
| DLCO (% predicted) | 72.7±24.2 | 63.5±22.1 | 47.8±16.5 | 63.8±23.5 |
| DLCO/VA (% predicted) | 69.5±17.4 | 71.9±17.6 | 52.1±15.8 | 66.6±18.6 |
| PaO2 (mmHg) | 79.5±9.5 | 78.8±8.0 | 65.7±7.7 | 76.2±10.1 |
| PaCO2 (mmHg) | 39.4±3.6 | 41.0±3.4 | 40.1±3.9 | 40.2±3.6 |
| Exercise capacity | ||||
| 6MWD (m) | 391±85.7 | 370±72.7 | 268±94.7 | 356±94.5 |
| SpO2 minimal (%) | 88.4±5.6 | 87.3±5.4 | 79.5±7.0 | 86.0±6.7 |
| Initial dyspnea (Borg) | 0.2±0.5 | 0.3±0.7 | 1.3±1.2 | 0.5±0.9 |
| Final dyspnea (Borg) | 1.3±0.9 | 1.9±1.3 | 3.4±1.2 | 2.0±1.4 |
| Final HR (bpm) | 114.8±20.7 | 127.3±14.6 | 131.1±24.3 | 123.2±20.4 |
| LCADL total score | 15.9±3.6⊗ | 17.8±5.8 | 20.8±5.1⊗ | 17.7±5.1 |
| Steps/day | 6118.1±2217.5* | 4853.5±1668.2♦ | 3079.8±1917.3*♦ | 4972.4±2242.3 |
BMI: body mass index; mMRC dyspnea: modified Medical Research Council dyspnea scale; BODE: BODE index (B: body mass index; O: obstruction; D: dyspnea; E: exercise); FEV1: forced expiratory volume in one second; FVC: forced vital capacity; TLC: total lung capacity; RV: residual volume; DLCO: carbon monoxide diffusion capacity; DLCO/VA: DLCO corrected to alveolar volume; PaO2: arterial oxygen pressure; PaCO2: carbon dioxide arterial pressure; 6MWD: six-minute walk distance; SpO2: arterial oxygen saturation; HR: heart rate; bpm: beat per minute.
Values are shown as mean±SD. Respiratory failure patients were classified as GOLD IV.
In the evaluation of daily life activities using the LCADL scale, there were differences with statistical relevance between the very severe patients (grade IV) and the patients with moderate COPD (grade II), with the former showing, on average, a higher total score in the LCADL scale (20.8±5.1 versus 15.9±3.6, p<0.027).
The evaluation of physical activity in daily life measured with pedometer in all groups of patients showed that the average number of steps per day was 4972.4, distributed through different stages of the disease according to Fig. 1. There were statistical differences between patients with COPD spirometry stage IV and patients with stages II and III, the very severe patients being those who walk less (on average 3079.8 versus 4853.5 and 6118.1 steps per day, p<0.001).

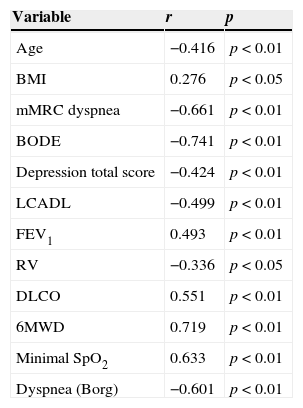
Examining the linear correlation coefficients (Table 2), the number of steps per day has shown a negative correlation with age, dyspnea, depression, BODE index, pulmonary hyperinflation and LCADL; it is positively correlated with the distance covered and with minimal oxygen saturation in 6MWT, FEV1, DLCO, and BMI.
Linear correlation coefficients.
| Variable | r | p |
|---|---|---|
| Age | −0.416 | p<0.01 |
| BMI | 0.276 | p<0.05 |
| mMRC dyspnea | −0.661 | p<0.01 |
| BODE | −0.741 | p<0.01 |
| Depression total score | −0.424 | p<0.01 |
| LCADL | −0.499 | p<0.01 |
| FEV1 | 0.493 | p<0.01 |
| RV | −0.336 | p<0.05 |
| DLCO | 0.551 | p<0.01 |
| 6MWD | 0.719 | p<0.01 |
| Minimal SpO2 | 0.633 | p<0.01 |
| Dyspnea (Borg) | −0.601 | p<0.01 |
BMI: body mass index; mMRC dyspnea: modified Medical Research Council dyspnea scale; BODE: BODE index (B: body mass index; O: obstruction; D: dyspnea; E: exercise); LCADL: London Chest Activity of Daily Living scale; FEV1: forced expiratory volume in one second; RV: residual volume; DLCO: carbon monoxide diffusion capacity; 6MWD: six minute walk distance; SpO2: arterial oxygen saturation.
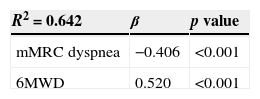
In order to test the contribution of every variable to explain the variance with the number of steps per day in the patients with COPD studied, we set a stepwise multiple regression analysis, so as to eliminate redundant variables. To this effect, all variables that had shown relevant correlations in the simple linear correlation analysis were included in the multiple regression analysis.
As a result, we got a model where the significant variables that helped to explain the number of steps per day (64.2% of its variance – R2=0.642) were dyspnea (mMRC) and the distance covered in 6MWT (Table 3).
DiscussionIn this study we identified the key factors related to physical activity in the daily life of a group of COPD patients at GOLD spirometry stage II to IV. These factors were dyspnea and the distance covered in 6MWT. Moreover, in our sample, there were differences between patients with stage IV and patients with moderate and severe COPD (stages II and III), the most severe cases being those patients who walk less in their daily routine (3079.8 steps per day) when compared to less severe patients (4853.5 steps per day) and the moderate ones (6118.1 steps per day). Even our moderate COPD patients are markedly sedentary, which classifies them as low active, as set out by Tudor-Locke and Bassett.6
Watz et al.19 also verified a larger reduction in COPD patients’ daily life physical activity according to the severity of the disease, but present at all COPD stages, compared to chronic bronchitis patients.
In relation to LCADL scale, there were significant differences between COPD stage IV (20.8) and COPD stage II patients (15.9); the most severe patients were those who showed greater restrictions during activities of daily living.
Comparing the pedometer and LCADL scale, we verified a negative and moderate correlation (r=−0.499; p<0.01) showing that the higher the ADL restraint, the lower the daily physical activity in these patients, assessed by the number of steps per day.
Among the factors that can limit physical activity in daily life, dyspnea is known to be rather variable in this population and its origin is recognized as multifactorial.20 The present study found a negative and moderate correlation (r=−0.661; p<0.01) between dyspnea (mMRC) and the number of steps per day, and it was one of the main factors that contributed to its variance (β=−0.406, p<0.001), reflecting the effect of the downward spiral of COPD, derived from the interaction of dyspnea, inactivity and physical deconditioning, since the higher the dyspnea is, the higher the ADL restraint and the lower the number of steps per day will be. Dyspnea assessed on the Borg scale was also negatively correlated with the number of steps per day, suggesting that the degree of dyspnea developed in the walk test is similar to the one realized in ADL evaluated by mMRC scale.21
Another determining factor for the variation of the number of steps per day was the distance covered in 6MWT (β=0.520, p<0.001). The high linear association between the daily physical activity assessed with the pedometer and the distance covered in 6MWT (r=0.719; p<0.001) suggests that the pedometer gives a valid measurement of physical activity in this group with functional restraint, quantifying walking, which is the most common and available physical activity modality and seems to strongly contribute to the level of total daily physical activity.22 Furthermore, this close relationship between the pedometer and 6MWT is comparable to what Fabio Pitta et al. also showed: the distance covered by 6MWT (functional exercise) has a high correlation with the physical activity level that patients develop in daily life.1 In Pitta's study, activity was also positively related to accelerometer data, showing that a reduction in the distance covered in 6MWT is the best marker of inactivity during the daily life of patients with COPD.
In this study, FEV1 was related in a positive and moderate way to the number of steps per day (r=0.493; p<0.01), as is also referred to in other studies.1,2,19 Other authors, however, have not found any correlation between physical activity and the severity of COPD, probably owing to differences in the degree of obstruction, sample size and the instruments used to assess physical activity in daily routine.23–26
As also mentioned in other papers,27–31 most of the patients in this sample (80%) showed pulmonary hyperinflation at rest. As one of the most important factors associated with dyspnea in patients with COPD, in our study, pulmonary hyperinflation also showed a negative and moderate correlation with the daily physical activity assessed by the pedometer (r=−0.511; p<0.01). However, it did not contribute to the variance in the number of steps per day in the multiple regression analysis.
Concerning gas exchanges, DLCO was positively correlated with the number of steps per day. Other authors32,33 also found a significant contribution of DLCO to the physical activity performance of COPD patients.
In this study, 76% of the patients showed arterial oxygen desaturation during the 6MWT and the minimal SpO2 correlated positively with the number of steps per day (r=0.633; p<0.01)
Age was negatively correlated (r=−0.416; p<0.01) with the level of physical activity registered by the pedometer, suggesting that older people are less active, walking fewer steps per day, as has already been shown.34
BMI was associated in a positive, significant and weak way (r=0.276; p<0.05) to the number of steps per day, as also shown in other studies.2,35
The BODE index showed a negative and strong correlation with the number of steps per day (r=−0.741; p<0.01). However, in the model of multiple linear regressions, its influence on the variance of the number of steps per day loses statistical relevance.
Psychological factors, such as anxiety and depression, have been described as frequent in these patients, contributing to a lower level of physical activity, even after well structured pulmonary rehabilitation programs. In this sample, the prevalence found was much lower than in other studies,36–39 but depression was correlated in a negative but moderate way with the number of steps per day (r=−0.424; p<0.01). Besides dyspnea and exercise capacity, psychological factors such as anxiety and depression, behavioral factors such as lack of motivation and self-efficacy, and social and environmental barriers are all capable of influencing physical activity and further studies should be directed at their identification and management.
There are some limitations to consider in this study. Since the sample only included male patients, we cannot apply the results to the female population. Although the prevalence of COPD is increasing in women, in Portugal it is still much more prevalent in men [18.7 versus 10.5% – Bárbara et al.43]. When recruiting patients for this study, there were so few COPD female patients that it would not have been possible to generalize the conclusions from these gender patients. Moreover, if there had been a control group it would have allowed us to compare the patients with another patient population group or to healthy people, thus marking their level of daily physical activity.
In this study the LCADL scale showed a low average total score (17.7), probably because the sample was formed by a male population, 73% of which stated they did not do any kind of household tasks, or because most of the patients underestimated the severity of their disease.18,39–42 While most of them considered themselves as suffering from a light dyspnea, their average number of steps per day was low, showing how inactive they are in their daily lives.
Concerning pedometer data, it is not possible to control possible sources of error, such as low walking speed, forgetting or incorrectly setting the equipment or vibrations, e.g. when driving a car or a bicycle. These errors are assumed to have been reduced by keeping with a three-day record, as recommended.5 As was demonstrated by Van Remoortel et al. in a recent systematic review (PROactive consortium), uniaxial pedometers are significantly less accurate than multisensor devices, particularly at slow walking speeds.44 Therefore the results of our study should be treated cautiously.
In conclusion, the main factors that contributed to physical activity restraint in male COPD patients daily life assessed with a pedometer were dyspnea (mMRC) and the low functional exercise capacity (distance covered in the 6MWT). These results point to the need for a better control of these two issues in clinical practice. These patients are markedly inactive and show limitations in ADL, becoming these features more evident in patients with very severe COPD.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
Master's degree dissertation on Health and Respiratory System, Faculdade de Ciências Médicas, Universidade Nova de Lisboa, Portugal.


