






The overlap between asthma and chronic obstructive pulmonary disease (COPD) (ACO) has been discussed for many years but clinical recommendations for this entity have been diverse. This study is intended to reach a consensus on diagnosis, treatment and patient orientation for ACO, within the Portuguese medical community.
MethodsThis study was conducted by a multidisciplinary panel of experts from three distinct medical specialties (Pulmonology, Family Medicine and Immunoallergology). This panel selected a total of 190 clinicians, based on their expertise in obstructive airway diseases, to participate in a Delphi structured survey with three rounds of questionnaires. These results were ultimately discussed, in a meeting with the panel of experts and some of the study participants, and consensus was reached in terms of classification criteria, treatment and orientation of ACO patients.
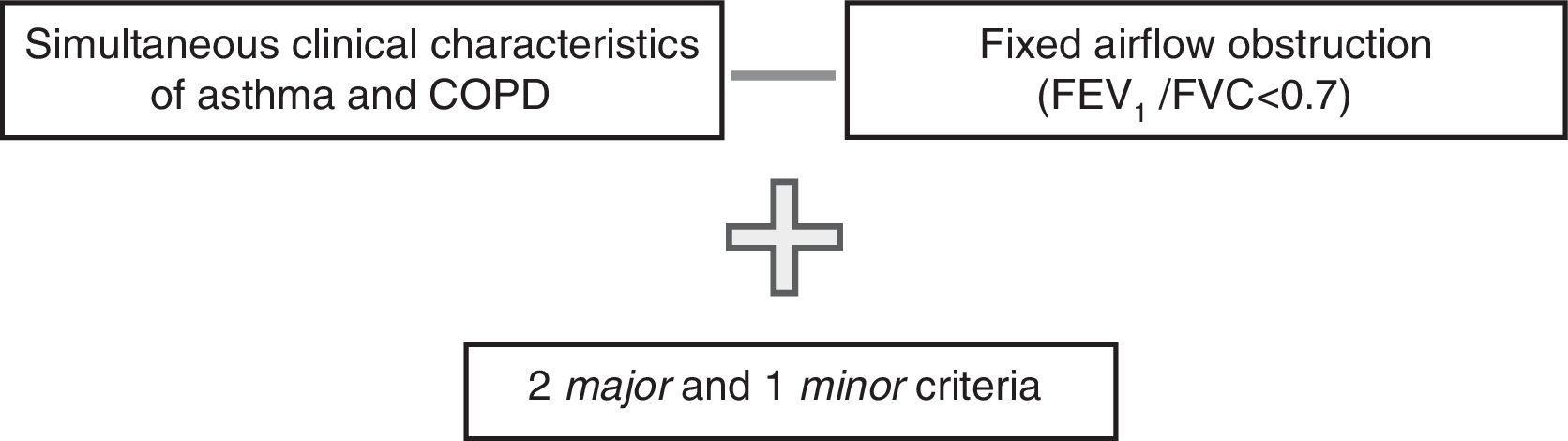
ResultsThe majority of clinicians (87.2%) considered relevant the definition of an overlap entity between asthma and COPD. A consensus was achieved on the diagnosis of ACO – presence of simultaneous clinical characteristics of asthma and COPD together with a fixed airflow obstruction (FEV1/FVC<0.7) associated with 2 major criteria (previous history of asthma; presence of a previous history of smoking exposure and/or exposure to biomass combustion; positive bronchodilation test (increase in FEV1 of at least 200mL and 12%) on more than 1 occasion) plus 1 minor criteria (history of atopy; age ≥40 years; peripheral eosinophilia (>300eosinophils/μL or >5% of leukocytes); elevation of specific IgEs or positive skin tests for common allergens). A combination of inhaled corticosteroid (ICS) with long-acting beta2-agonist (LABA) or long-acting muscarinic antagonist (LAMA) was considered as first line pharmacological treatment. Triple therapy with ICS plus LABA and LAMA should be used in more severe or symptomatic cases. Non-pharmacological treatment, similar to what is recommended for asthma and COPD, was also considered highly important. A hospital referral of ACO patients should be made in symptomatic or severe cases or when there is a lack of diagnostic resources.
ConclusionsThis study highlights the relevance of defining ACO, within the Portuguese medical community, and establishes diagnostic criteria that are important for future interventional studies. Recommendations on treatment and patient's orientation were also achieved.
Although asthma and chronic obstructive pulmonary disease (COPD) are considered distinct obstructive airway diseases, the coexistence of features of both diseases in the same patient has been long recognized. In this context, the individualization of an entity of overlap between asthma and COPD has recently been proposed. Several publications from diverse working groups have proposed different terms and classification criteria to describe these patients.1–7 However, none of these terms or criteria has been universally accepted.
The lack of consensus on how to define and categorize such an entity of overlap between asthma and COPD limits the development of prospective studies needed to determine the optimal approach to these patients.
Some authors have already published a diverse set of criteria for asthma/COPD overlap. Most can be grouped by category, such as (1) clinical criteria and related risk factors, (2) lung function and (3) laboratory data/immune-inflammatory markers. Among the proposed criteria are: (1) simultaneous presence of clinical features of asthma and COPD in the same patient, previous history of asthma or atopy, current or past history of smoking or biomass combustion exposure, age >40 years-old; (2) presence of persistent airflow limitation (post-bronchodilator FEV1/FVC<0.7), positive or very positive response to the bronchodilator test (FEV1 increase of at least 200mL and 12% or at least 400mL and 15%, respectively), presence of bronchial hyperresponsiveness; (3) peripheral eosinophilia (>300eosinophils/μL or >5% of the total leukocytes), sputum eosinophilia, elevation of the fractional exhaled nitric oxide (FENO) and elevation of total serum immunoglobulin E (total IgE).1–7 In fact, our group carried out a review of the main definitions and diagnostic criteria which was published recently,8 in addition, in this paper a proposal of recommendations adapted to the Portuguese situation was achieved by a group of respiratory disease experts. In order to obtain a broader consensus, a larger study was needed, leading to the present project.
ObjectivesThe main aims of this project, intended to be adapted and applied in Portuguese clinical practice, were:
- 1.
to assess the need for the recognition of an overlap entity between asthma and COPD within the Portuguese medical community who treat patients with respiratory diseases;
- 2.
to achieve consensus over terminology and classification criteria for such an entity;
- 3.
to achieve consensus on the approach and adequate orientation of these patients.
This study was conducted by a multidisciplinary panel of experts from three distinct medical specialties: Pulmonology, Family Medicine and Immunoallergology.
A committee panel was created with elements from the three specialties described above. This committee selected a total of 190 members from the three medical specialties – Pulmonology (n=85), Family Medicine (n=62) and Immunoallergology (n=43) – to participate in the questionnaires based on their expertise in obstructive airway diseases.
The study followed a Delphi structure with three rounds of questionnaires. The first questionnaire was mainly composed of open-ended questions in order to obtain meaningful answers that reflect the overall non-conditioned opinion of the participants. A classical content analysis was endorsed, organized by tabulating records with the frequency of freely elicited ideas. The results were discussed within the scientific board of a multidisciplinary panel of experts and the subsequent survey was drawn up based on the answers obtained in the first round, the same process was used for the final questionnaire. The second questionnaire was intended to be the cornerstone of the inquiry, containing a detailed and wide range of questions comprising nomenclature and the three main domains of the diagnostic criteria (clinical, lung function and laboratory data/immune-inflammatory markers), as well as treatment approach and orientation of the patients. The third questionnaire aimed at clarifying any topic that had not been fully established in the preceding round or any doubt that had arisen in the discussion of the data obtained previously.
The answers were not conditioned in any way, even if only theoretically. Previously existing ideas and concepts were on the basis of this consensus survey.
These questionnaires were inserted into an online platform specifically created for this study. A link to this platform was sent via electronic mail to the clinicians who answered anonymously and with a user sensitive and confidential password to provide access to the platform. The clinicians were allowed to answer each questionnaire in stages; they did not need to answer everything at once. Answering time ranged from minutes to two weeks, so that the participants had enough time to think about their answers, which did not force a pattern of only immediate opinions.
After the application of the questionnaires, a final meeting took place, involving the committee panel and some of the respiratory experts that had participated in this study, in which the results were discussed and a consensus was obtained in terms of classification criteria, treatment and orientation of ACO.
ResultsEach step of the Delphi had a different number of responders, the first questionnaire having the lowest participation (Table 1).
Total participants and their basic characterization, by questionnaire.
| 1st questionnaire | 2nd questionnaire | 3rd questionnaire | ||
|---|---|---|---|---|
| Total participants (n) | 47 | 88 | 104 | |
| Age (mean±SD), years | 46.5 (±10.5) | 46.4 (±10.8) | 46.2 (±11.1) | |
| Gender | Male (%) | 42.6 | 52.3 | 51.0 |
| Female (%) | 57.4 | 47.7 | 49.0 | |
| Medical speciality | Pulmonology (n) | 12 | 27 | 28 |
| Family medicine (n) | 15 | 26 | 37 | |
| Immunoallergology (n) | 20 | 35 | 39 | |
We received 47 answers to the first phase questionnaire. The clinicians had a mean (±standard deviation) age of 46.5 (±10) years and 57.4% were female. There was a reasonable participation by each medical specialty (Table 1).
The purpose of the first question was to assess if the participants agreed on the existence of an entity of asthma and COPD overlap. The majority of the clinicians (87.2%) considered that it was necessary to identify such an overlap entity. Only six participants considered that there was no such need.
Those who agreed with the recognition of a distinct entity of overlap between asthma and COPD were asked to propose a designation for that entity. Two terms stand out from the proposals: asthma-COPD overlap syndrome (ACOS), n=15, and asthma-COPD overlap (ACO), n=12. Other designations were proposed, but were not considered to be relevant since each of them was only supported by a residual number of participants.
The participants were also asked if the information in the medical literature was sufficient for identifying the overlap entity and the majority (85.1%; n=40) considered that currently available information was insufficient.
The participants were then requested to propose essential criteria to define the overlap between asthma and COPD entity. A variety of criteria were suggested and these were divided into 3 categories: clinical, lung function and laboratory data/immune-inflammatory markers. The most relevant clinical criteria for the participants were: previous history of asthma, age, clinical features of asthma and COPD, exposure to tobacco smoking or to biomass combustion and atopy. In terms of lung function, clinicians considered that spirometry should be taken into account, considering as criteria the presence of fixed obstruction, obstruction with partial reversibility, positive bronchodilator response and also a positive bronchodilator response in a COPD patient and poor reversibility in an asthmatic patient. In terms of criteria related to laboratory data/immune-inflammatory markers, peripheral eosinophilia was the one most frequently suggested.
Forty clinicians (85.1%) considered that the identification of this entity of overlap had distinct therapeutic implications from those generally adopted in asthma and COPD. The orientation suggested by the participants was divided into pharmacological and non-pharmacological measures. Regarding pharmacological treatment, most suggested inhaled corticosteroid (ICS) in association with long-acting beta2-agonist (LABA) or long-acting muscarinic antagonists (LAMA) (50.0%) and triple therapy with ICS, LABA and LAMA (29.2%). Other measures clinicians considered important were the control of risk factors, such as smoking cessation, ensuring effective vaccination coverage for flu and pneumococcus, the treatment of comorbidities, implementation of a pulmonary rehabilitation program and allergenic eviction.
This first questionnaire was thus answered by a reasonable number of participants of each medical specialty. The answers were almost unanimous, they considered that it was necessary to identify an entity of overlap between asthma and COPD and that the literature available about this issue was not sufficient. Moreover, most of them considered that the recognition of this entity of overlap implied a distinct therapeutic approach. This supported the following steps of our work, leading to the following rounds of questionnaires. These were mainly composed of close-ended questions, taking into account the answers obtained from the previous questionnaire.
Second questionnaireThe second questionnaire was answered by 88 clinicians with a mean (±SD) age of 46.4 (±10.8) years and rather homogenous distribution between the three medical specialties that were consulted – Immunoallergology (n=35), Pulmonology (n=27) and Family Medicine (n=26).
In this questionnaire, the majority of physicians surveyed answered all the questions, which means that the interpretations that are made are effectively derived from the universe of physicians surveyed. Globally, medical specialties did not differ substantially between each other regarding the clinical approach to this entity.
The first question was how to describe the overlap entity between asthma and COPD better. Only 3.4% of the participants answered that there was no need for a definition because they believed the entity did not exist. The majority chose between the two options that were provided – Asthma-COPD overlap syndrome (ACOS) and Asthma-COPD overlap (ACO) – with almost identical numbers between the two – 48.9% vs. 46.6%, respectively.
One of the most important topics analyzed in this questionnaire was the relevance attributed by the clinicians to the several diagnostic criteria presented.
The diagnostic criteria were divided into three groups – clinical, lung function and laboratory data/immune-inflammatory markers.
Clinicians were asked to rate, on a scale of 1–10, each criterion in terms of its clinical relevance. Scores ≥7 were considered highly relevant.
The majority of the clinicians considered the presence of simultaneous clinical characteristics of asthma and COPD in the same patient (88.6%) to be highly relevant to the clinical criteria. The presence of a previous history of asthma (72.7%) and presence of a smoking history (76.1%) were also criteria where a significant consensus on high relevance was met. On the other hand, other criteria such as a previous history of atopy, exposure to biomass fuel combustion, and age ≥40 years, met with more diverse opinions (percentage of highly relevant considerations: 46.6%, 63.6% and 65.9%, respectively).
Regarding lung function criteria, almost all the clinicians think that the presence of fixed airflow obstruction (FEV1/FVC<0.7) is highly relevant (84.1%). A positive bronchodilatation test and a definition of positive bronchodilation test characterized by an increase in FEV1 of at least 200mL and 12% were also considered to be of great importance (85.2% and 64.8%, respectively). A positive bronchodilation test on more than one occasion was a criterion in which there was a more heterogenic pattern of answers (only 42.1% considered it highly relevant). A very positive bronchodilation test with an increase in FEV1 of 400mL and at least 15% and the presence of bronchial hyperreactivity did not achieve the same consensus (26.1% and 36.4%, respectively, considered it highly relevant). Family Medicine gave greater importance to bronchial hyperresponsiveness than did Pulmonology and Immunoallergology (Sig χ2=0.055), although this was not an indisputable differentiation, it was at least a strong trend.
None of the laboratory data/immune-inflammatory markers, (peripheral eosinophilia, total IgE, FENO, and specific IgEs) achieved a significant degree of consensus in terms of degree of importance (39.8%, 18.2%, 25.0% and 35.2% considered it highly relevant, respectively).
Another of the questions concerned the definition of the overlap entity using major and minor criteria. The majority of the clinicians (75.2%) agreed with this approach.
With regard to treatment, clinicians were asked which should be the first line of treatment. Most of them chose the ICS plus LABA and/or LAMA (69.3%), or ICS plus LAMA and/or LABA (22.7%). Although the majority of participants from the different medical specialties considered the association of ICS plus LABA and/or LAMA as the most appropriate as a first line treatment, Family Medicine participants differed from the other participants, with almost half of them considering the association between ICS plus LAMA as a first line treatment (Sig χ2=0.025).
The clinicians were asked about other non-pharmacological therapeutic measures they thought should be applied in patients with this overlap entity. Almost all of them considered an encouragement of therapeutic adherence (94.3%), a verification of the inhalation technique (100%) and comorbidities treatment (92%) as key measures to adopt.
Other measures such as smoking cessation (97.7%), pulmonary rehabilitation (78.4%), and pneumococcal and influenza vaccination (96.6%) were also considered highly relevant.
Clinicians were divided over where the initial medical diagnostic approach should be performed, whether in a specialist hospital clinic (45.5%) or in primary healthcare (52.3%). The follow-up of these patients should be performed, according to the clinicians, first in a specialist hospital clinic and then in articulation with primary care (47.7%), or in the hospital only in the case of a non-controlled patient (44.3%). On this point, a significant difference in the pattern of approach was noted between medical specialties. Pulmonologists and Immunoallergologists most frequently considered that the initial approach should be performed in a specialized hospital clinic while Family Medicine participants considered they had sufficiently good conditions and the knowledge to perform the diagnosis of ACO with a high degree of autonomy, suggesting that they should be responsible for this first step (Sig χ2<0.01). A similar pattern was observed in relation to patient follow-up (Sig χ2=0.005).
Third questionnaireThe third questionnaire was answered by 104 clinicians, with a mean (±SD) age of 46.2 (±11.1) years and 51% were male. There was an almost homogenous distribution by the three medical specialties: Immunoallergology, n=39, Family Medicine, n=37 and Pulmonology, n=28.
This questionnaire was entirely made up of close-ended questions, taking into account the answers obtained from the previous questionnaires. The first questions intended to reach a consensus on which criteria should be considered for the diagnosis of the entity of overlap and specifically if each criterion should be considered as major or minor. Criteria that were considered highly relevant in the previous questionnaire were included in this round. Those criteria with heterogeneous answers were also included to try to achieve a better clarification.
Concerning the clinical criteria, it was almost unanimous (87.5%) that the presence of simultaneous clinical characteristics of asthma and COPD in the same patient should be considered a major criterion (vs. 8.7% considering it as a minor criterion and only 3.8% answering that it shouldn’t be considered as a criterion). Two other clinical criteria were also classified as major criteria, though not with such an expressive concordance: the presence of a previous history of asthma (69.2 vs. 28.8% considering it as a minor criterion) and the presence of a previous history of smoking exposure and/or exposure to biomass fuel combustion (72.1 vs. 26% considering it as a minor criterion). For each of these criteria only 1.9% of the participants answered that these should not be considered as criteria. The remaining clinical criteria, history of atopy and age ≥40 years, were considered as minor criteria by the clinicians (69.2% and 49%, respectively). For these two last criteria, a higher number of participants did not agree with its inclusion (7.7% and 11.5%, respectively).
In terms of functional criteria, most of the clinicians (83.7%) considered the presence of fixed airflow obstruction (FEV1/FVC<0.7) as a major criterion (vs. 10.6% considering it as a minor criterion and only 3.8% of the participants answering that it should not be considered as a criterion). A positive bronchodilation test, characterized by an increase in FEV1 of at least 200mL and 12%, was also classified as a major criterion by 53.8% of the clinicians (vs. 37.5% considering it as a minor criterion and 7.7% participants answering that it should not be considered as a criterion).
All laboratory data/immune-inflammatory markers were considered as minor criteria by the majority of the participants: peripheral eosinophilia, defined as >300 eosinophils/μL or >5% of leukocytes (54.8 vs. 15.9% considering it as a major criterion), elevation of total IgE (53.8 vs. 3.8% considering it as a major criterion), elevation of FENO (51.0 vs. 5.8% considering it as a major criterion), elevation of specific IgEs or positive skin tests for common allergens (59.6 vs. 10.6% considering it as a major criterion). Also, all of these criteria had a significant number of participants disagreeing with their inclusion as criteria (respectively, 26.9%, 39.4%, 36.5% and 28.8%).
Most of the clinicians considered the presence of at least 2 major and 1 minor criteria (72.1%) as the minimum number of criteria needed for the diagnosis of the overlap entity.
In relation to the periodicity of the clinical evaluation, the majority of the clinicians (83.7%) considered that this should be performed every 3 to 6 months in the early phase, and then adapted to the patient's clinical severity/control. The periodicity of the lung function assessment was considered by most clinicians (76.0%) in the same time frame.
DiscussionThis study was the first to explore the concept of asthma-COPD overlap within the Portuguese medical community, enabling a consensus regarding the need for the recognition of an overlap entity. A significant number of participants and the use of a Delphi method strengthened the study results. After a final meeting, where all the results were discussed, it was possible to reach a consensus over nomenclature, classification criteria, treatment and orientation of these patients.
The existence of patients who have at the same time clinical characteristics of both asthma and COPD has been a well-known fact for many decades,9,10 but only recently has it begun to attract more attention.1–8 The need to define this entity is something that is shared by most clinicians who work in respiratory medicine. In our study, the majority of the respondents to the first questionnaire (87.2%) confirmed this intention. However, there is still a lack of clear and solid diagnostic criteria for this overlap which can be used by all clinicians, an idea shared by most in our study group (85.1%).
There have been a few guidelines, published in recent years, proposing specific criteria for the diagnosis of the asthma-COPD overlap entity. The first was created by the Spanish group GesPOC in 2012,1 followed by the Finnish2 and Czech guidelines3 with similar proposals. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) and the Global Initiative for Asthma (GINA) published a joint document in 2014.4 A more recent consensus between specialists from North America, Asia and Europe was also published.5
Although very recently a Portuguese meeting of experts in respiratory medicine produced diagnostic recommendations for ACOS,8 there was a need for a broader analysis using a more accurate method for assessing the perspective of the Portuguese medical society on the asthma-COPD overlap, by recruiting a considerable number of clinicians in three fields of Medicine (Immunoallergology, Family Medicine and Pulmonology).
The designation of the overlap entity was one of the points addressed in the first questionnaire. Most of the clinicians chose between two of the most commonly accepted names – asthma-COPD overlap syndrome (ACOS) and asthma-COPD overlap (ACO). Since the overlap between these two chronic lung diseases is not really a syndrome or a single disease, we believe that ACO should be the chosen designation, which is in line with what is recommended by the latest GOLD and GINA joint guideline on ACO.6
We can divide the diagnostic criteria into three main categories: Clinical, Lung function and Laboratory data/immune-inflammatory markers.
In terms of clinical criteria, the presence of simultaneous clinical characteristics of asthma and COPD in the same patient was considered highly relevant and should be listed, according to the majority of the clinicians, as a major diagnostic criterion. This is in line with what is sustained in several guidelines, such as the Spanish, Finnish and Czech, although with some slight differences in some of them. Also seen in most guidelines is the presence of a previous history of asthma and smoking history/exposure to biomass fuel combustion, which were also considered relevant criteria in this survey.
One of the main concerns in clinical practice is to identify which COPD patient would benefit from the use of ICS. This is where the algorithm for ACO can play a role, and so it seems more important that we have a diagnosis of COPD in a patient that may also have a diagnosis of asthma or have evidence of positivity on bronchodilation tests. The need for having a COPD diagnosis is stated in a recent GesPOC and GEMA algorithm.7 However, this diagnostic approach was not assessed in our study, so we cannot comment on what the clinician's opinion would be on this.
On the other hand, other criteria such as a previous history of atopy and age ≥40 years were considered as minor criteria.
Regarding lung function, almost all clinicians agreed that the presence of a fixed airflow obstruction (FEV1/FVC<0.7) is highly relevant for the diagnosis of ACO and should be considered as a major criterion. This criterion is also present in most of the guidelines. There is more heterogeneity in terms of bronchodilation test positivity. In our Delphi, a positive bronchodilation test, with an increase in FEV1 of at least 200mL and 12%, and a positive bronchodilation test on more than one occasion were considered highly relevant and major criteria. A very positive bronchodilation test, with an increase in FEV1 of 400mL and at least 15%, was not considered as relevant, contrary to several guidelines, where this is listed as a major criterion.1–3 By lowering the threshold for the bronchodilation criteria we risk over diagnosing COPD patients with ACO, and so it is important to register the maintenance of these results on more than one occasion for a more accurate ACO diagnosis. Although we might have a more “definitive diagnosis” of ACO with a very positive bronchodilation test, we might be missing some patients who could benefit from the use of ICS.
In terms of laboratory data/immune-inflammatory markers, the participants in our study did not consider any of them as highly relevant or as major criteria. Peripheral eosinophilia, defined as >300 eosinophils/μL or >5% of leukocytes, and elevation of specific IgEs or positive skin tests for common allergens, were the criteria that received most consensus (>70% of the participants agreeing with their inclusion) and should be considered as minor criteria. Some guidelines considered the inclusion of an elevation of total IgE and FENO as diagnostic criteria of ACO in a COPD patient. FENO is an immune-inflammatory marker of increasing importance and application, but the lack of established cut-offs justifies the decision not to include this criterion in the diagnostic algorithm. Also, the fact that it is not widely available in many clinical settings limits its applicability. However, in some cases, it might be taken into account in order to help support the diagnosis.
The clinicians in our study considered a minimum of 2 major and one minor criteria for the diagnosis of ACO. In most guidelines, the presence of a least 2 major or 2 minor and 1 major is considered sufficient.
The definition of an algorithm for the diagnosis of ACO was established after the final meeting of respiratory experts. It was assumed that this diagnosis should only be considered in patients that have “simultaneous clinical characteristics of asthma and COPD” and “fixed airflow obstruction (FEV1/FVC<0.7)”. As a result, these two criteria must always be present and do not count as major criteria. The diagnostic algorithm can be seen in Fig. 1. The proposed criteria for establishing the diagnosis of ACO are listed in Table 2.
Criteria for the diagnosis of ACO.
| Major | Minor | ||
|---|---|---|---|
| Clinical criteria | Previous history of asthma | X | |
| Presence of a previous history of smoking exposure and/or exposure to biomass combustion | X | ||
| History of atopy | X | ||
| Age ≥40 years | X | ||
| Lung function criteria | Positive bronchodilation test (increase in FEV1 of at least 200mL and 12%) in more than 1 occasion | X | |
| Laboratory data | Peripheral eosinophilia (>300 eosinophils/μL or >5% of leukocytes) | X | |
| Elevation of specific IgEs or positive skin tests for common allergens | X |
Concerning treatment, most clinicians agreed that ACO should have a specific therapeutic approach. The combination of ICS with LABA or LAMA was considered the first line of treatment by the majority, and the use of triple therapy with ICS plus LABA and LAMA in more severe or symptomatic cases (Table 3). Although there is still a lack of scientific evidence to support these choices, there seems to be some consensus on this subject with the use of ICS plus LABA or triple therapy being recommended by the majority of the guidelines.1–8 The use of ICS plus LAMA was also considered as a valid first-line therapeutic option by a considerable number of clinicians. This differs from what is recommended by most consensus documents1–8 but could be a plausible choice and should be the subject of future interventional studies on ACO patients.
Proposed treatment for a patient with the diagnosis of ACO.
| First-line | Second-line (in more severe or symptomatic cases; no response to first line) | |
|---|---|---|
| Pharmacological treatment | ICS with LABA or LAMA | ICS plus LABA and LAMA |
ICS – inhaled corticosteroid; LABA – long-acting beta2-agonist; LAMA – long-acting muscarinic antagonist.
Non-pharmacological treatment also plays a very important role in ACO patients and this was stressed by the clinicians in this study. Smoking cessation, pulmonary rehabilitation, pneumococcal and influenza vaccination, reinforcement of the therapeutic adhesion, verification of the inhalation technique and comorbidities treatment were considered key components in the management of these patients. The importance of these measures has a very high consensus in the medical community and is present in most guidelines, not only for ACO but also for COPD or asthma.
The place for initial assessment and clinical orientation of ACO patients was also evaluated in this study. Clinician's answers were divided between a specialist hospital clinic and primary healthcare on the subject of initial diagnostic medical approach and follow-up. The latter option was mainly considered by Family Medicine specialists, which might be a bias since the majority of them had a clinical focus on chronic airway diseases and might not correspond to the overall reality of Family Medicine practice in Portugal. Moreover, in settings with a lack of diagnostic resources, there might be a more consensual need for a hospital referral. Additionally, we believe that a patient with a symptomatic or severe ACO should also be referred to a specialist. Although there is no established definition on what constitutes severe ACO, we suggest following the national recommendations for hospital referral in asthma and COPD patients.11,12 Regarding the periodicity of clinical and lung function evaluation, according to the majority of the clinicians, it should be performed every 3–6 months in the early phase, and then adapted to the patient's clinical severity and symptoms.
This Delphi survey is the first one to analyze the opinion on asthma/COPD overlap of the Portuguese medical community. The fact that we have clinicians from different medical specialties, who manage patients with respiratory conditions, enables us to have a broader understanding of this entity. This is also one of the largest studies, in terms of number of participants, on this subject, which strengthens the relevance of the results. The use of a Delphi methodology also enabled to access the different items more accurately, in a step by step approach.
The fact that we had a rather low participation in the first questionnaire, probably because of its open ended based questions, and the lack of mandatory consecutive answers to all the questionnaires, are weaknesses of this study.
ConclusionAsthma-COPD overlap has been a matter of interest and debate in the last few years. Different criteria and diagnostic algorithms were proposed for establishing the diagnosis of ACO. However, there is a lack of consensus regarding this issue. This study had a nationwide participation of clinicians from different medical specialties that manage patients with chronic obstructive airways diseases. It was clear that the information previously available regarding this entity was not sufficient for their daily clinical practice and there was a general agreement about the need to define ACO. Based on the Delphi method, sequential steps of a set of questionnaires were applied and analyzed in order to establish diagnostic criteria and an algorithm for the approach of ACO, adapted to our national context.
Conflicts of interestThe authors have no conflicts of interest to declare.
We would like to thank the participation of a group of experts in obstructive airway diseases from Pulmonology, Family Medicine and Immunoloallergology that participated in this nationwide survey, as members of the Delphi ACO Portugal. Once anonymity has been guaranteed, their names cannot be listed.
We would also like to thank to Prof. Henrique Lopes, who collaborated in the study design.
It is recognized the support in the form of Educational Grant from Mundipharma Pharmaceuticals Ltd.


