



Smoking has been proven to be an important risk factor for disease severity and worse outcomes in Covid-19, the disease caused by SARS-CoV-2.1
The World Health Organization (WHO) recommends not smoking in order to reduce the risk of harm caused by the disease and warns against reports that tobacco or nicotine could benefit Covid-19 as they do not provide sufficient evidence for this statement.2 In our practice at the Antismoking Center of the National Cancer Institute of Milan, the smoker’s assessment has proved particularly useful, in particular, for this purpose, we use carbon monoxide (CO) measure in the exhaled breath.
Starting from June 2020 it was possible, keeping the distance between patients and the use of personal protection devices, to resume the activity of the antismoking center, but the Covid-19 situation has posed non-emergency labs with the question of how to proceed with clinical tests safely while avoiding virus transmission among patients3; so, we addressed the problem of safe CO measurement.
The level of carboxyhemoglobin in the blood can be determined by measuring the exhaled CO through an instrument that provides the CO value in parts per million (ppm). This type of measurement is then configured as an extremely useful tool in smoking cessation assessment, to enhance motivation to quit and for follow-up of smoking cessation programs.
One of the major company for CO analyzers is Bedfont Scientific Ltd with its main product “Smokerlyzer™”, a portable instrument with research and education aims. The model we have available in our antismoking centre is a Micro+ Smokerlyzer™ model purchased in 2012. It is composed of the electronic device (Fig. 1a), the fitting provided with an antibacterial filter (Fig. 1b) which lasts 30 days and the disposable mouthpieces (Fig. 1c). For the latest models Bedfont has produced disposable antibacterial filters, but our model is not compatible.
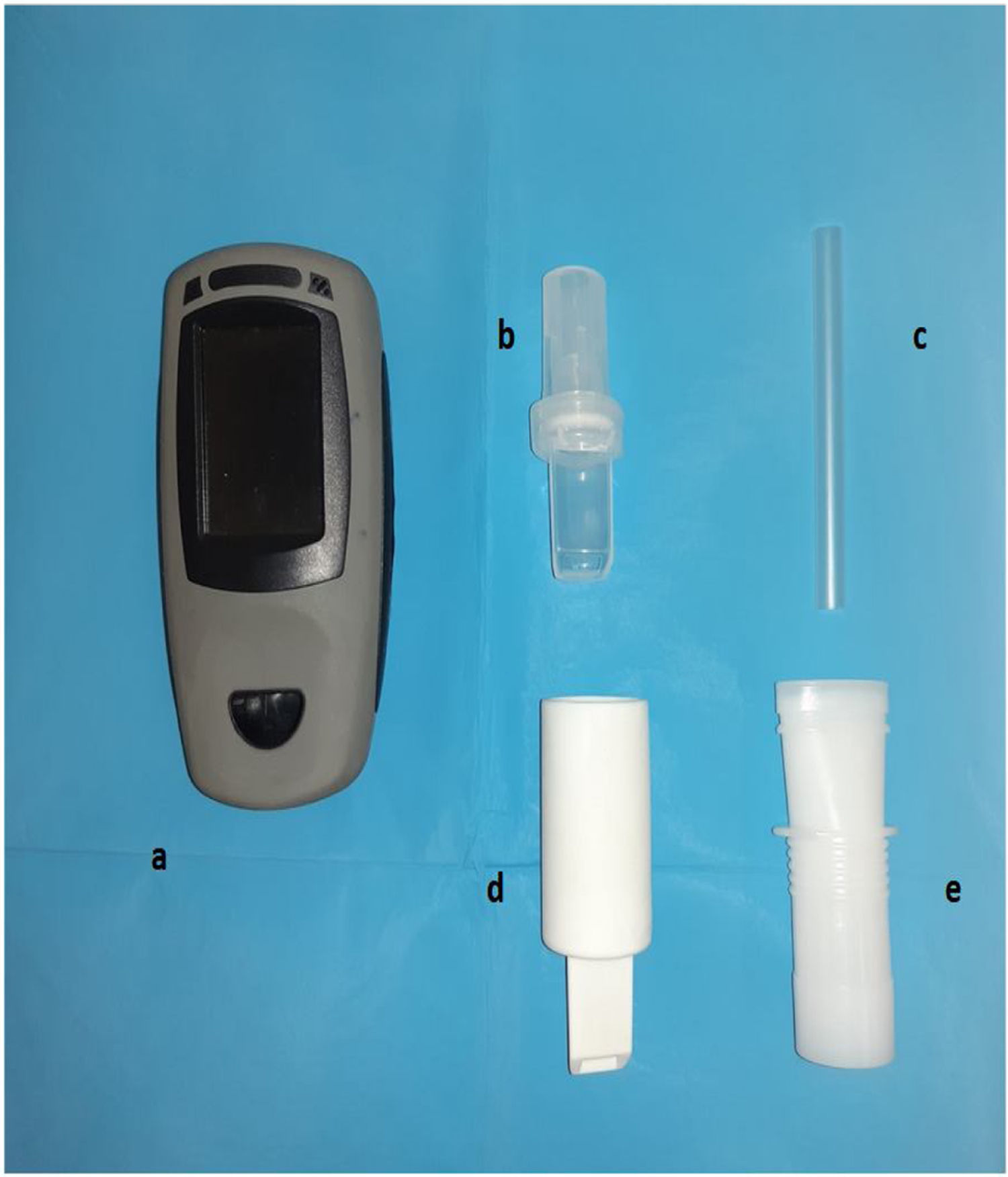
To safely use the CO analyzer, we thought of substituting the fitting with an antibacterial filter with a new one, specially created (Fig. 1d). This fitting, designed with the help of our clinical engineering department, was made of a plastic polymer and printed via a 3D printer. The size of the fitting (section and length) was calculated to make minimum modifications in order not to change significantly the flow rate and the volume of air entering the device; in this way it is possible to avoid alterations related to the detection and calibration of the instrument. It does not contain any filters and it can be washed and disinfected after each use. The fitting has been molded to allow the attachment of disposable mouthpieces that we usually use for the execution of spirometries (Fig. 1e). This mouthpiece contains an electrostatic and certified mechanical filter that removes bacteria and viruses at an efficiency rate of >99%, thus reducing risks of cross contamination during testing. Through this solution we can guarantee the use of a single filter for each patient.
The safety of this measurement must be guaranteed not only for patients but also healthcare professionals. The use of appropriate personal protective equipment (PPE) is of pivotal importance for the healthcare workers involved in the care of patients with viral infections, such as the current pandemic, Covid-19.4 In collaboration with Health and Safety Protection Unit, considering that this procedure provides for the emission of exhaled breath, we have reviewed it: workers must carry out the procedure with Covid-19 personal PPE and, as further precaution, the patient is asked to plug his or her nose with disposable forceps so that there is no exhalation from the nasal cavities during the procedure.
Due to the risk of Covid-19 transmission, it was impossible for us to test the CO analyzer for correct measurement of exhaled CO for smokers with and without modified fitting, but during the first period of the modified device use, we verified that the detector has not undergone alterations in the measurement of the CO concentration. In fact, we used the device during our checks among smoking patients and we detected values compatible with the self-reported smoking status.
The completely new situation that arose during the period of the Covid-19 pandemic, characterized by social isolation, physical distancing, possible loss of employment and prolonged lockdown, is highly stressful and therefore predisposing people to find refuge in addictive substance, and among these, tobacco.5
Therefore, smokers and ex-smokers are at greater risk of worsening their health condition by smoke dependence due to the pandemic; furthermore, smoking does not only constitute individual damage: the lockdown has forced many people to stay at home, increasing indoor smoking and therefore the possibility of exposing family and neighbors to secondhand smoke6; in addition, cigarette smoke has been identified as a possible vehicle for the Covid-19 virus as droplets are more easily released into the environment while smoking.7 In addition some studies5 have even indicated that the pandemic has increased the possibility of people wanting to quit smoking.
All these considerations suggest the importance of promoting smoking cessation during the Covid-19 pandemic. In the future it will be necessary not to interrupt the antismoking services, including the measurement of CO safe for patients.
Conflicts of interestThe authors have no Conflicts of interest to declare.


