


Pulmonary rehabilitation (PR) is an evidence-based intervention to improve symptoms, exercise capacity and quality of life of people with chronic respiratory diseases (CRD), such as those with chronic obstructive pulmonary disease (COPD) and asthma.1 However, evidence from these specific CRD shows that these benefits diminish over time.2,3 Non-adherence to health-enhancing behaviours is one of the key factors associated with this decline.2,4 Therefore, novel approaches to promote long-term adherence and preserve the benefits gained are needed.
There is a growing evidence base for the use of internet/web-based approaches to support self-management and empowerment of patients with chronic diseases. Internet-based interventions have been shown to effectively improve health behaviours, such as physical activity.5 A web-based self-management program for patients with CRD may have the potential to be a novel and effective approach to support patients’ long-term compliance with health-enhancing behaviours.5 However, few studies have evaluated the access to the internet or other digital technologies (e.g., smartphones) among patients with CRD, which are fundamental for the implementation of web-based approaches. The objective of this study was to explore if patients with CRD have access to digital technology and if they feel confident using it.
Patients with CRD were recruited from community-based PR programmes in seven healthcare centres of the centre region of Portugal, between October 2017 and September 2018. Inclusion criteria were having a diagnosis of CRD, at least 18 years old, and being referred by their general practitioner to a community-based PR programme. Exclusion criteria were history of a neoplasic/immunologic disease or presence of acute cardiac condition or a significant cardiac, musculoskeletal, neuromuscular or psychiatric condition. The study was approved by the Center Health Regional Administration (73/2016) and by the National Data Protection Committee (NDPC – 7295/2016).
All referred patients attended an initial visit at their primary healthcare centre, where they completed a structured questionnaire with the support of two trained physiotherapists. Sociodemographic (age, sex, marital status, education and occupation), anthropometric and clinical (diagnosis, smoking habits, history of exacerbations and health resources use in the previous year) data were first obtained. Disability resulting from dyspnoea was also collected using the modified Medical Research Council questionnaire (mMRC).6 The primary outcome measures were access to technology and level of confidence in using it. Patients were surveyed regarding the use of internet; access to computers, smartphones (combination of mobile phone, web browser and computer capabilities)/tablets and cell phones (simple devices mainly for voice calls and text messages). Their level of confidence in using these technologies was assessed with two structured questions (How confident do you feel using the internet?How confident do you feel using this device?). Patients rated their confidence on a numerical scale from 0 (not at all confident) to 10 (completely confident) and were considered confident when a score of 6 or greater was selected. A previous study showed a mean of 6 represented confidence in computer experience.7 All data, collected after obtaining the informed consent of patients, were anonymised and processed in bulk according to the requirements of the NDPC and to comply with the General Data Protection Regulation. Descriptive statistics were used to describe the sample. Chi-square tests for categorical data or independent t-tests for continuous data were used to explore if access to digital technology was related to patients’ characteristics. Variables that were statistically different were used as independent variables in one multivariate logistic regression using the Stepwise method. The overall model was evaluated using the Nagelkerke's R-square.
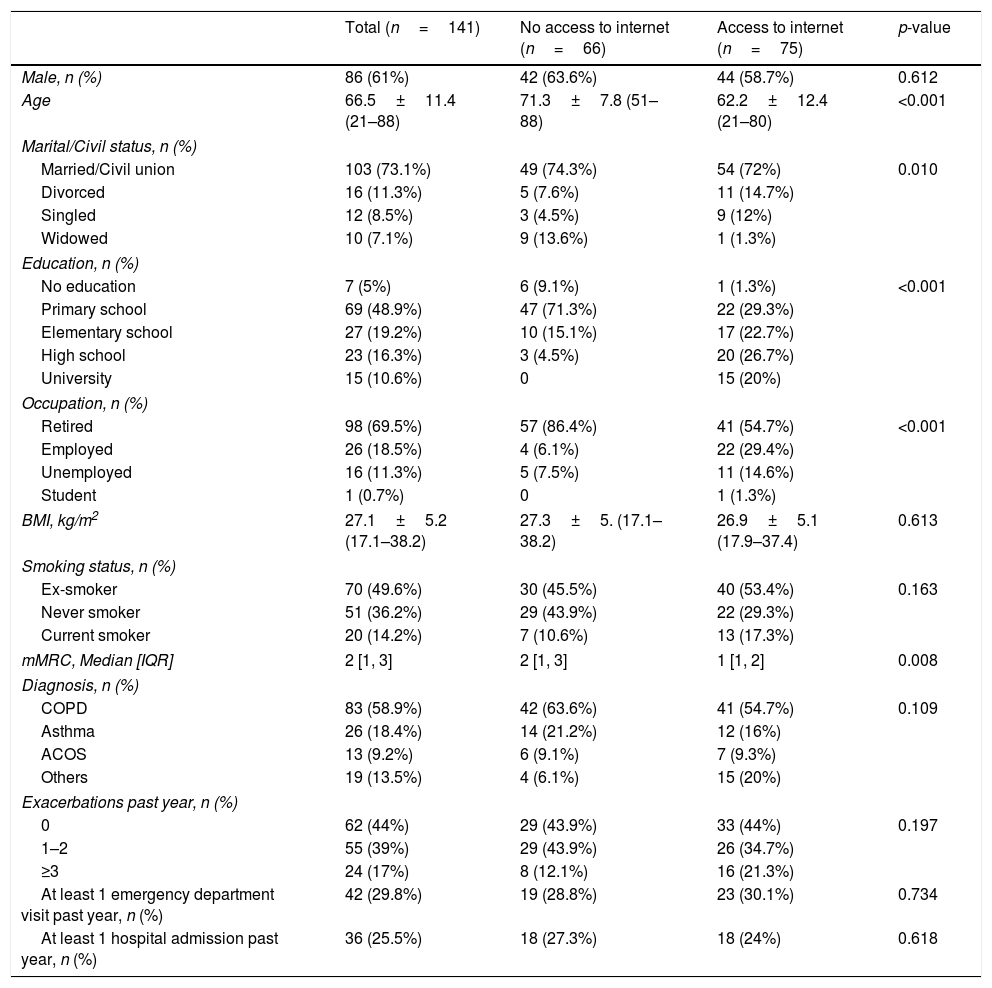
A total of 141 patients were enrolled, with a mean age of 66.5±11.4 [21–88] (Table 1). Patients were mostly married (73.1%) and almost half had only completed primary school (48.9%) (Table 1). COPD (n=84; 59.6%) and asthma (n=26; 18.4%) were the most common diagnosis (Table 1). A total of 115 (81.6%) patients reported having access to digital technology: 62 (44%) used the smartphone or tablet, 53 (37.6%) used the computer and 52 (36.9%) the cell phone. 81% of patients reported themselves to be confident using these technologies (median 7, interquartile range 5–9.5). Median confidence was similar across the distinct technologies (Fig. 1). More than half of the patients (n=75; 53.2%) used the internet and, from these, 85% felt confident in using it (median 8, interquartile range 5.75–10) (Fig. 1).
Characteristics of the participants (n=141).
| Total (n=141) | No access to internet (n=66) | Access to internet (n=75) | p-value | |
|---|---|---|---|---|
| Male, n (%) | 86 (61%) | 42 (63.6%) | 44 (58.7%) | 0.612 |
| Age | 66.5±11.4 (21–88) | 71.3±7.8 (51–88) | 62.2±12.4 (21–80) | <0.001 |
| Marital/Civil status, n (%) | ||||
| Married/Civil union | 103 (73.1%) | 49 (74.3%) | 54 (72%) | 0.010 |
| Divorced | 16 (11.3%) | 5 (7.6%) | 11 (14.7%) | |
| Singled | 12 (8.5%) | 3 (4.5%) | 9 (12%) | |
| Widowed | 10 (7.1%) | 9 (13.6%) | 1 (1.3%) | |
| Education, n (%) | ||||
| No education | 7 (5%) | 6 (9.1%) | 1 (1.3%) | <0.001 |
| Primary school | 69 (48.9%) | 47 (71.3%) | 22 (29.3%) | |
| Elementary school | 27 (19.2%) | 10 (15.1%) | 17 (22.7%) | |
| High school | 23 (16.3%) | 3 (4.5%) | 20 (26.7%) | |
| University | 15 (10.6%) | 0 | 15 (20%) | |
| Occupation, n (%) | ||||
| Retired | 98 (69.5%) | 57 (86.4%) | 41 (54.7%) | <0.001 |
| Employed | 26 (18.5%) | 4 (6.1%) | 22 (29.4%) | |
| Unemployed | 16 (11.3%) | 5 (7.5%) | 11 (14.6%) | |
| Student | 1 (0.7%) | 0 | 1 (1.3%) | |
| BMI, kg/m2 | 27.1±5.2 (17.1–38.2) | 27.3±5. (17.1–38.2) | 26.9±5.1 (17.9–37.4) | 0.613 |
| Smoking status, n (%) | ||||
| Ex-smoker | 70 (49.6%) | 30 (45.5%) | 40 (53.4%) | 0.163 |
| Never smoker | 51 (36.2%) | 29 (43.9%) | 22 (29.3%) | |
| Current smoker | 20 (14.2%) | 7 (10.6%) | 13 (17.3%) | |
| mMRC, Median [IQR] | 2 [1, 3] | 2 [1, 3] | 1 [1, 2] | 0.008 |
| Diagnosis, n (%) | ||||
| COPD | 83 (58.9%) | 42 (63.6%) | 41 (54.7%) | 0.109 |
| Asthma | 26 (18.4%) | 14 (21.2%) | 12 (16%) | |
| ACOS | 13 (9.2%) | 6 (9.1%) | 7 (9.3%) | |
| Others | 19 (13.5%) | 4 (6.1%) | 15 (20%) | |
| Exacerbations past year, n (%) | ||||
| 0 | 62 (44%) | 29 (43.9%) | 33 (44%) | 0.197 |
| 1–2 | 55 (39%) | 29 (43.9%) | 26 (34.7%) | |
| ≥3 | 24 (17%) | 8 (12.1%) | 16 (21.3%) | |
| At least 1 emergency department visit past year, n (%) | 42 (29.8%) | 19 (28.8%) | 23 (30.1%) | 0.734 |
| At least 1 hospital admission past year, n (%) | 36 (25.5%) | 18 (27.3%) | 18 (24%) | 0.618 |
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; mMRC, modified Medical Research Council Dyspnoea Scale; ACOS, Asthma COPD Overlap Syndrome. Data are presented as mean±SD (range) or n (%), unless otherwise indicated.
.")
Patients with access to the internet were younger (p<0.001), were mostly married or single/divorced (p=0.010), had higher levels of education (p<0.001); were mostly of active age (employed, unemployed, student) and had lower mMRC scores (p=0.008). Lower age (odds ratio – OR=.935; 95% confidence interval – 95%CI .889–.982) and a higher level of education (OR=3.633; 95%CI 2.093–6.307) increased the likelihood of using the internet. This logistic regression model was statistically significant (χ2(2)=59.67, p<0.001) and explained 46% (Nagelkerke R2) of the variance in internet use.
Most patients had access to digital technologies: more than 1/3 used the internet or computer and almost half used a smartphone/tablet. Similar data (i.e., 33% used the internet daily, 44% had a computer and 41% a smartphone), have been reported in a European study about patients’ preference for using technologies to participate in COPD clinical trials.8 In the United States, 40.2% of the elderly have access to a computer and 39.9% to the internet.9 However, confidence in using digital technologies was lower (computer 36.1%; internet 29.9%; tablet 22.1%).9 Nevertheless, the patients enrolled were older than the ones included in the present study, and a different data collection method (10-point numerical scale vs. 5-point Likert-scale) was used.9 Younger patients and those with higher levels of education were most likely to use the internet. A previous study with 512 patients recruited in primary healthcare also found that internet use was associated with age less than 60 years, college education and household income level.10 This study has some limitations. Our sample was mainly composed of patients with COPD and asthma recruited from Portuguese primary healthcare centres, hindering the generalisation of our findings to all CRD, healthcare settings and different countries. In addition, we assessed both access and confidence using patients’ self-report, which may reflect bias in reporting. Future studies with larger samples of subjects with distinct CRD recruited from primary and secondary care centres should be conducted combining subjective and objective data.
This study shows that patients with CRD from the community, namely those with COPD and asthma, have access to and feel confident using digital technologies. These results reinforce the potential of using digital technologies as a resource for self-management/maintenance strategies in this population.
FundingThis work is integrated in the project Revitalizing Pulmonary Rehabilitation (3R), SAICT-POL/23926/2016, was funded by Fundo Europeu de Desenvolvimento Regional (FEDER) – Comissão Diretiva do Programa Operacional Regional do Centro and by Fundação para a Ciência e Tecnologia (FCT) and partially funded by Programa Operacional Competitividade e Internacionalização (COMPETE), through COMPETE 2020 (POCI-01-0145-FEDER-016701) and FCT (UID/BIM/04501/2013, UID/BIM/04501/2019, and POCI-01-0145-FEDER-007628-iBiMED). CJ is a pos-doc fellow (SFRH/BPD/115169/2016) funded by Fundação para a Ciência e Tecnologia (FCT), reimbursed by Fundo Social Europeu and by national funds of MCTES.
Conflicts of interestNone.
We would like to acknowledge the primary healthcare centres involved (Unidade de Saúde Familiar (USF) Marquês de Marialva, Unidade de Cuidados de Saúde Personalizados (UCSP) Mira, Unidade de Cuidados na Comunidade (UCC) Cubo Mágico, Unidades do Centro de Saúde de Agueda, Unidades do Centro de Saúde de Aveiro, UCSP Estarreja).


